
WRIST JOINT
- The wrist joint (also known as the radiocarpal joint) is a synovial joint in the upper limb, marking the area of transition between the forearm and the hand.
- In this article, we shall look at the structures of the wrist joint, the movements of the joint, and the relevant clinical Structures of the Wrist Joint
- Articulating Surfaces
The wrist joint is formed by:
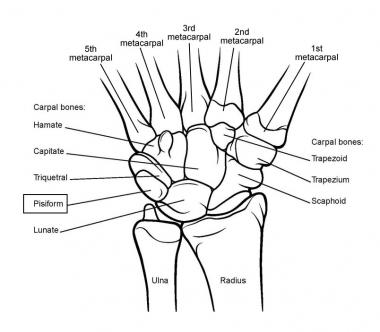
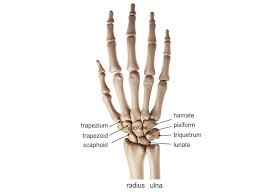
- Distally – The proximal row of the carpal bones (except the pisiform).
- Proximally – The distal end of the radius, and the articular disk (see below).
- The ulna is not part of the wrist joint – it articulates with the radius, just proximal to the wrist joint, at the distal radioulnar joint.
- It is prevented from articulating with the carpal bones by a fibrocartilaginous ligament, called the articular disk, which lies over the superior surface of the ulna.
- Together, the carpal bones form a convex surface, which articulates with the concave surface of the radius and articular disk.
Joint Capsule
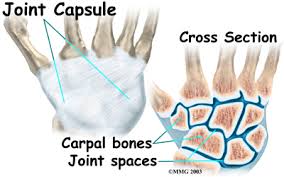
- Like any synovial joint, the capsule is dual layered.
- The fibrous outer layer attaches to the radius, ulna and the proximal row of the carpal bones.
- The internal layer is comprised of a synovial membrane, secreting synovial fluid which lubricates the joint.
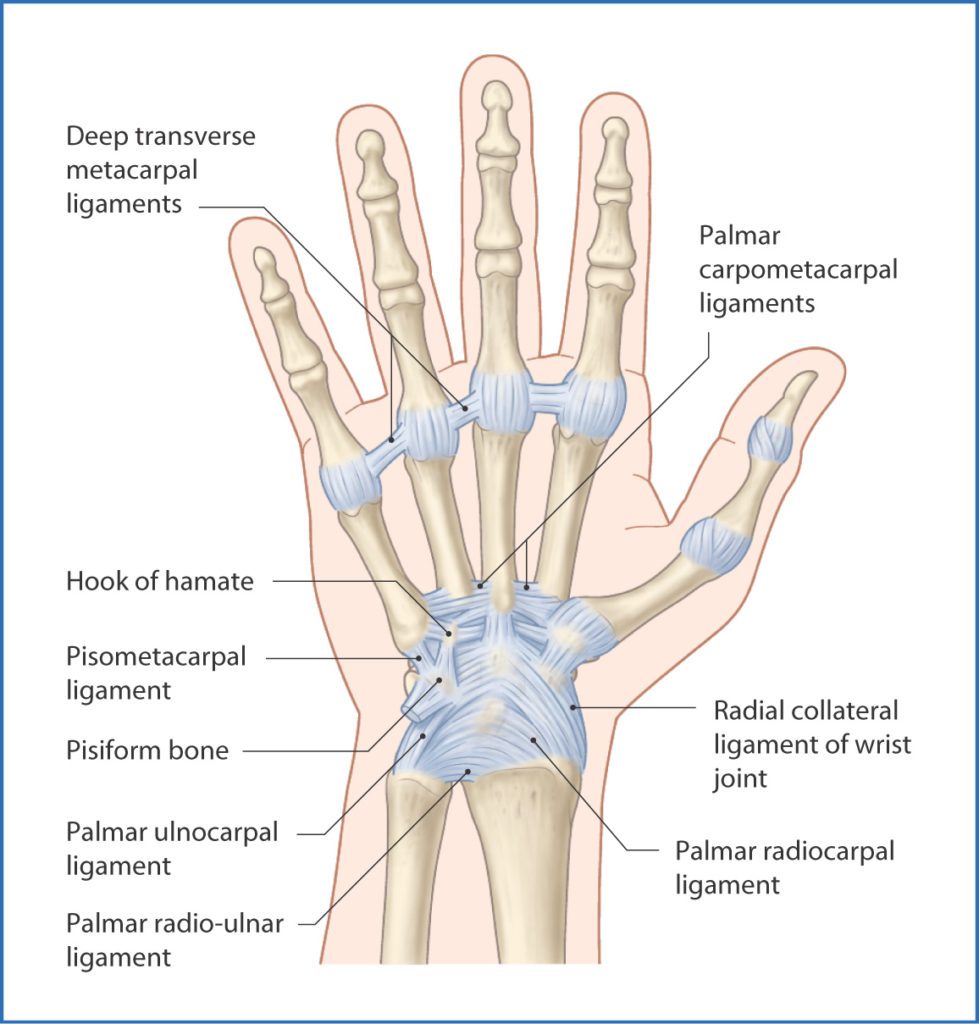
Ligaments
There are four ligaments of note in the wrist joint, one for each side of the joint
Palmar radiocarpal –
- It is found on the palmar (anterior) side of the hand.
- It passes from the radius to both rows of carpal bones.
- Its function, apart from increasing stability, is to ensure that the hand follows the forearm during supination.
Dorsal radiocarpal –

- It is found on the dorsum (posterior) side of the hand.
- It passes from the radius to both rows of carpal bones.
- It contributes to the stability of the wrist, but also ensures that the hand follows the forearm during pronation.
Ulnar collateral –
- Runs from the ulnar styloid process to the triquetrum and pisiform.
- Works in union with the other collateral ligament to prevent excessive lateral joint displacement.
Radial collateral –
- Runs from the radial styloid process to the scaphoid and trapezium.
- Works in union with the other collateral ligament to prevent excessive lateral joint displacement.
Neurovascular Supply
- The wrist joint receives blood from branches of the dorsal and palmar carpal arches, which are derived from the ulnar and radial arteries.
Innervation to the wrist is delivered by branches of three nerves:
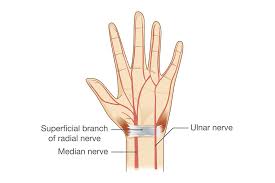
- Median nerve – Anterior interosseous branch.
- Radial nerve – Posterior interosseous branch.
- Ulnar nerve – deep and dorsal branches.
Movements of the Wrist Joint
- The wrist is an ellipsoidal (condyloid) type synovial joint, allowing for movement along two axes.
- This means that flexion, extension, adduction and abduction can all occur at the wrist joint.
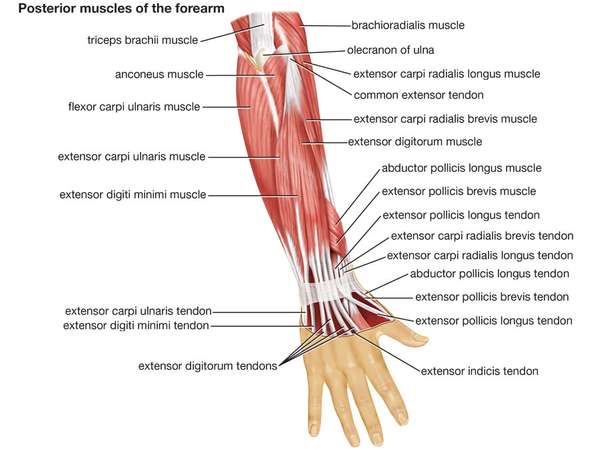
- All the movements of the wrist are performed by the muscles of the forearm.
Flexion –
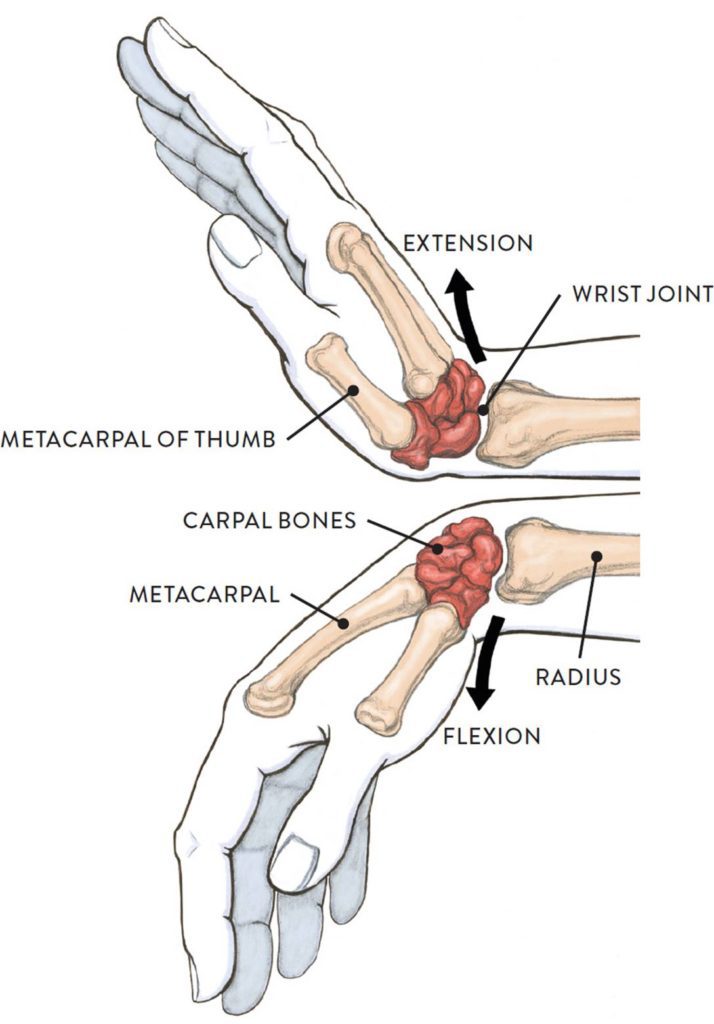
- Produced mainly by the flexor carpi ulnaris, flexor carpi radialis, with assistance from the flexor digitorum superficialis.
Extension –
- Produced mainly by the extensor carpi radialis longus and brevis, and extensor carpi ulnaris, with assistance from the extensor digitorum.
Adduction –
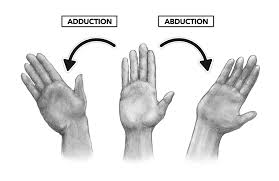
- Produced by the extensor carpi ulnaris and flexor carpi ulnaris
Abduction –
- Produced by the abductor pollicis longus, flexor carpi radialis, extensor carpi radialis longus and brevis.
Clinical Relevance: Injuries to the Wrist Joint
- injuries of the wrist
- Fractures of distal radius.
Adults children
- Colle’s fracture. 1. Fracture distal radial epiphysis
- Smith’s fracture. 2. Fracture distal radial mataphysis
- Barton’s fracture.
- Radial styloid fracture.
Injuries of the carpus :any of the bones of the carpus may be injured or dislocated. The common and important injuries are,
- Scaphoid fracture.
- Lunate dislocation.
- Peri-lunate dislocation.
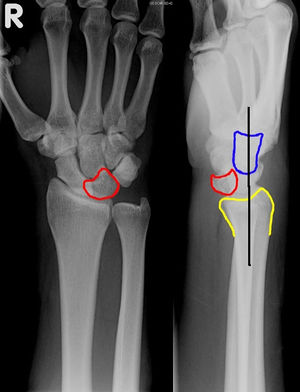
- Dorsal chip fracture.
- This is fracture of the distal end of the radius produced by a fall on to the palm of the outstretched hand.
- This injury is uncommon below the age of 50 years.
- After this, it is one of the commonest fracture, particularly common in women, the high incidence being related to the onset of postmenopausal osteoporosis.
- Fracture line about 2 to 2.5 cm proximal to the distal articular surface of radius. Distal fragment is shifted dorsally, proximally into the shaft, angulated radially and supinated.
- There is always an associated injury to the inferior radio-ulnar joint.
Clinical features :
- (a) The appearance of wrist is typical and described as a ‘dinner – fork’ deformity. Viewed from the side the dorsal aspect of the wrist is unduly prominent, viewed from the dorsum the lateral aspect of the wrist is slightly prominent and hand is radially deviated.
- (b) The fracture site is tender.
- (c) The radial styloid process is no longer distal to the ulnar styloid process, instead the two styloid processes are approximately at the same level.
Diagnosis by x-ray wrist A-P and lateral view.
Complications : malunion, stiffness of wrist, shoulder and fingers, carpal tunnel syndrome.
This clinical condition produces what is known as the ‘dinner fork deformity’.
Smith’s fracture
- This is the reverse of Colle’s fracture, the distal fragment is flexed rather than dorsiflexed.
- It is uncommon.
- It is due to a fall on the dorsum of the palmar – flexed wrist or due to a backward fall on the outstretched hand.
Barton’s fracture:
- This is an intra articular fracture of the distal radius with anterior displacement of a small fragment along with the carpus.
- Redisplacement is very common after closed reduction.
- The fracture is best managed by open reduction and application of an Ellis T – plate.
Radial styloid fracture (chauffer’s fracture):
- This injury occurs following a direct blow on wrist or occasionally following a fall on the wrist .
- The fracture line is transverse extending laterally from the articular surface of radius and the fracture is more often undisplaced.
Fractures in children
Fracture distal radial epiphysis :
- This is child’s Colle’s fracture.
- Due to separation of the distal radial epiphysis resulting in a displacement similar to the Colle’s fracture.
Fracture distal radial metaphysis:
- This may occur at any level proximal to the epiphyseal plate.
- The fracture may be of the greenstick variety or may be complete.
Scaphoid fracture
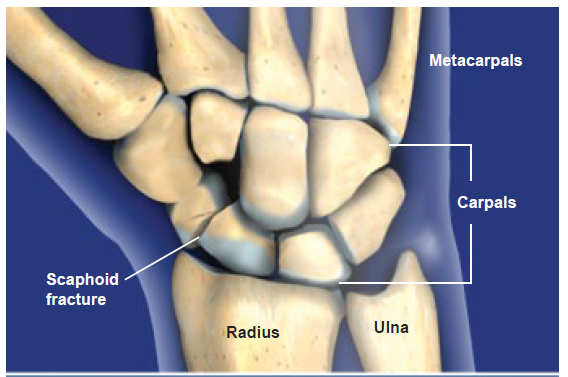
- The commonest injury of the carpus.
- Injury occurs following a fall on the outstretched hand, typically in young adults.
- Clinical features : patient presents with pain in the wrist, but function of the wrist may not be grossly impaired.
- On examination, there will be a tenderness over the scaphoid in the anatomical snuff box, a little swelling and no bruising.
- These physical signs suggest a ‘sprained wrist’ rather than a fractures.

- Radiologically examination : AP view, lateral view and two oblique view should be taken to confirm the diagnosis.
- X-ray may not display the fracture immediately after injury since no displacement occurs at the fracture site.
- Repeated X-ray after one or two weeks when the suspicion still remains after negative X-ray.
- The fracture may be in the proximal pole, waist, distal pole or tubercle of scaphoid and may be displaced or undisplaced.
Complications : Non union, avascular necrosis of the proximal fragment.
Lunate & perilunate dislocation:
- The mechanism is fall on the palm of outstreched, dorsiflexed hand which displaces the whole of carpus backwards leaving only the lunate in contact with radius called perilunate dislocation.
- The dislocation may reduce but displaces the lunate forward out of position causing lunate dislocation.
- This may be associated with fracture of scaphoid.
Clincal features :
- The wrist and fingers are stiff and the wrist is swollen and tender.
- If the lunate has dislocated, it may compress the median nerve to cause median nerve signs.
- A well centered lateral X ray clearly reveals the dislocated lunate in front of the carpus.
- The AP view is important to exclude the associated fracture of scaphoid and close inspection of X ray AP view will show that the bones of the proximal row of carpus (scaphoid, lunate, triquetral) are not disposed round the head of the capitate with the intervention of a regular joint space as in the normal wrist.
- If lunate is displaced , it appears triangular rather than quadrangular in outline.
Dorsal chip fracture
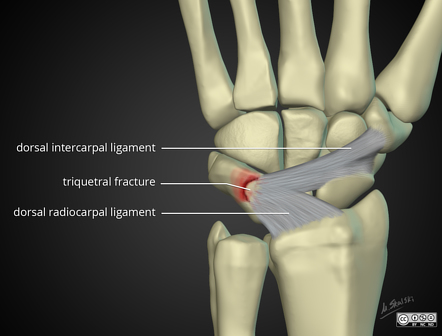
- This ligamentous or capsular avulsion of a flake of bone from the dorsal aspect of the carpus.
- It results from forced palmar flexion of the wrist.
Articular disorders of the wrist
- Deformities
- Arthritis
- Miscellaneous
I DEFORMITIES: some rare disorders are ,
Carpal fusions :

- Coalescence of two or more of the carpal bones.
- It is the commonest congenital abnormality.
- Inherited as autosomal dominant trait and may be bilateral and often associated with other abnormalities.
- Will not cause problems and treatment is not necessary.
Radial club hand :

- The infant is born with the wrist in marked radial deviation.
- There is absence the whole or part of the radius and usually also the thumb or the entire first two rays of the hand.
- It may occur as an isolated abnormality or as part of a generalised dysplasia.
- Treatment : Gentle manifestation and splintage. Operation to centralise the carpus over the ulna probably before the age of three years.
Madelung’s deformity:

- It is the congenital subluxation or dislocation of lower end of ulna from malformation of the bones.
- There may be minor generalised abnormalities of bone structure often with short stature.
- It may be also be caused by disease or fracture – a fracture at the lower end of the radius with upward displacement of the lower fragment.
- The deformity varies in degree from a slight prominence of lower end of ulna at the back of the wrist to complete dislocation of the inferior radio- ulnar joint with marked radial deviation of the hand.
- The more sever form is associated with congenital absence of the radius.
Ulnar club hand :

- Ulnar deviation present at birth and is due to partial or complete absence of the ulna.
- The radial head may dislocate as the child grows.
Distal ulnar dysplasia :
- In older children with hereditary multiple exostoses there is dispropotionate shortening of ulna, its distal end becomes carrot – shaped and the radius is bowed.
Wrist drop:
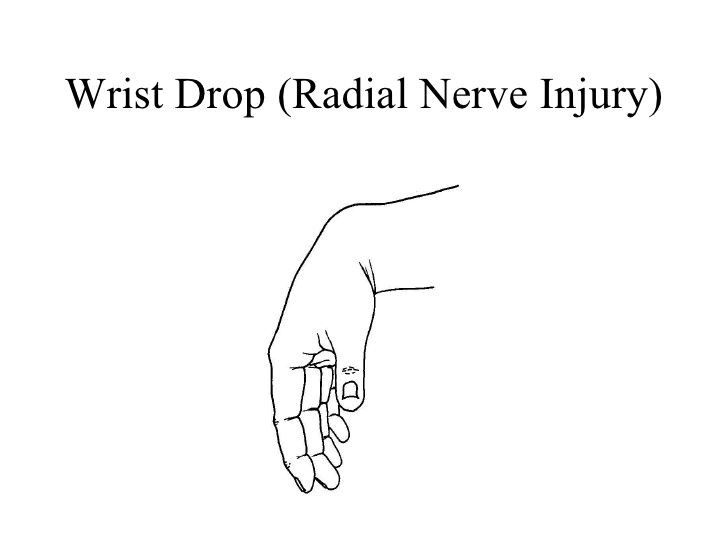
- radial nerve palsy : With radial nerve palsy the wrist drops into the flexion and active extension is lost.
II ARTHRITIS:
Pyogenic arthritis :

- Pyogenic arthritis of the wrist is uncommon.
- Infection may be haematogenous or it may be introduced through a penetrating wound.
- Clinical features : Acute onset with constitutional symptoms, pain and swelling about the joint, increased local warmth and marked impairment of movement.
- Radiographic features : In the early stages X rays do not show any alteration from the normal.
- Later, if the infection persists there is diffuse rarefaction with loss of cartilage space and some destruction of bones.
Rheumatoid arthritis :

- It commonly affects the wrist and hands and is a major cause of serious loss of function and ugly deformities.
- Affected joints are swollen from synovial thickening and movement is restricted.
- In the later stages articular cartilage and the underlying bones are eroded and the fingers tend to deveiate medially – ulnar deviation.
- X- ray : Radiography do not show any abnormality at first.
- Later there is diffuse rarefaction of the bones.
- As the disease progresses there will be destruction of cartilage leading to narrowing of the joint space & subchondral bone erosion.
Osteoarthritis :

- It is uncommon and develops as a sequel of injury.
- The commonest predisposing factors are fracture of the lower end of the radius with involvement of articular surfaces, fracture of scaphoid bone complicated by avascular necrosis of the distal fragment, dislocation of the lunate bone, Kienbock’s disease of the lunate bone and long established rheumatoid arthritis.
- Predominant pathological change is degeneration and wearing away of the articular cartilage lining the joint surfaces.
- Patient complains of gradully increasing pain and stiffness of wrist worse on activity.
- Movements are markedly limited and painful if forced at the extremes.
- The skin temperature is normal.
- X- ray : narrowing of the joint space & spurring or sharpening of bone at joint margins.
III. MISCELLANEOUS :
Kienbock’s disease:

- It is a rare affection of the lunate bone characterised by softening, fragmentation & liability to deformation.
- Later it may lead to osteoarthritis of the wrist.
- Exact aetiology is unknown. Repeated injury is a predisposing factor
- Clinical features : pain in the wrist, most marked at the centre of the joint over the lunate area which is worse during active use of wrist.
- Strength of the grip is impaired due to pain.
- X –ray : Lunate appears slighly more denser than surrounding bones, later the bone has a fragmented appearance.
EXTRA-ARTICULAR DISODERS ABOUT THE WRIST:
Chronic infective tenosynovitis:

- Chronic inflammation of flexor tendon sheath in the lower forearm and hand occuring in response to low grade infection.
- Flexor sheaths are commonly affected.
- The affected sheaths are greatly thickened and show changes of chronic inflammation, contain excess of fluid.
- Patient presents with gradual onset of swelling with mild aching pain, in the region of the affected tendon sheath.
- The function of the fingers and thumb impaired. Affects the lower 5 or 6 cms of the front of the forearm and proximal part of palm.
- Treatment : Of mild cases – wrist and forearm immobilisation.
Stenosing tenovaginitis:
- This is a condition of unknown aetiology in which the sheath of a tendon thickens spontaneously, so as to entrap the tendon.
a) De Quervain’s tenovaginitis:

- the common sheath of abductor pollicis longus and extensor pollicis brevis tendons at the wrist are affected.
- Women between 40 – 50 years are usual victims.
- Pateint complains of pain andd difficulty in abducting and extending the thumb.
- A bulge is detected on examination on the tendons over the radial styloid process.
b) Trigger finger :
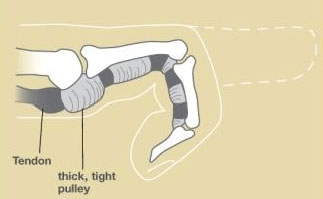
- The fibrous sheaths of the flexor tendons of the fingers and thumb are involved.
- The flexor tendons gradually develops a constriction under the retinaculum and a bulge distal to it.
- Patient complains of tenderness at the base of the affected finger and locking of finger in full flexion.
- The locking can be overcome either by a strong effort or by extending the finger passively with the other hand, then the flexion is released with a distinct snap, like a trigger of a pistol.
- Treatment : Dividing appropriate retinaculum
Carpal tunnel syndrome :
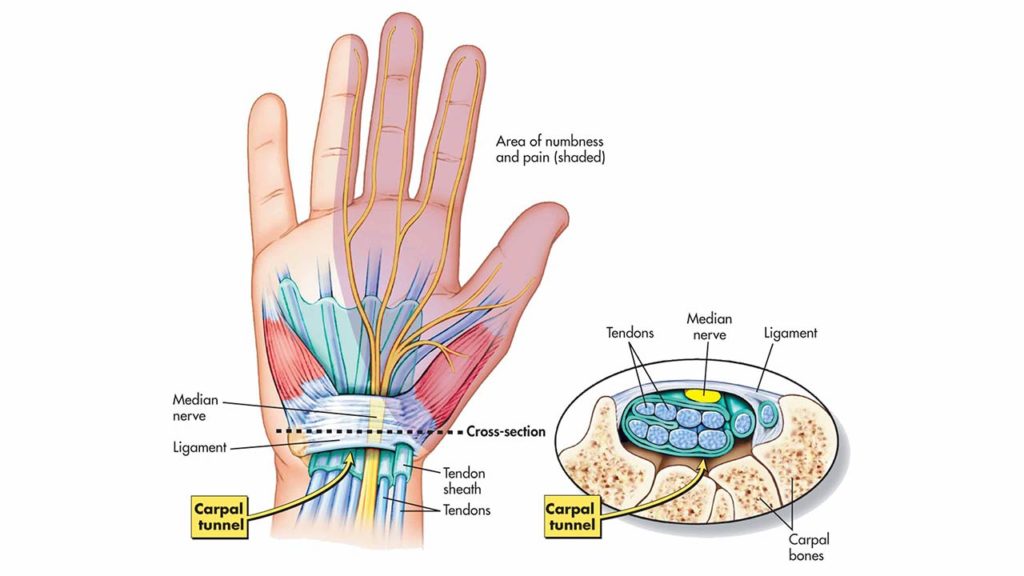
- The carpal tunnel is formed by the flexor retinaculum anteriorly and by the distal row of the carpus posteriorly through which flexor tendons and median nerve passes.
- Any swelling likely to result in compression and ischaemia of median nerve in carpal tunnel – this may occur in acromegaly, myxoedema, multiple myeloma, rheumatoid arthritis, pregnancy, osteoarthritis of wrist etc. causes carpal tunnel sydrome.
- Clinical features : tingling, numbness or discomfort in the radial three and half digits and difficulty in carrying out fine movements.
- Shaking the hands in the air gives relief – flick test.
- Flexion of wrist for 60 sec causes pain – Phalen’s sign.
- Tinel’s sign – sharp, shooting pain along the distribution of median nerve when the flexor retinaculum is tapped gently.
- Treatment : longitudinal incision of flexor retinaculam gives relief.
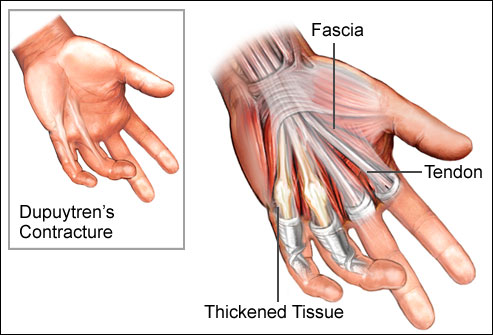
- There is localized thickening and contracture of the palmar fascia and there may be nodules in the fascia or in the subcutaneous tissue.
- This condition mostly affects the medial part of the palmar fascia in which the ring finger and less often little finger become flexed.
- Aetiology is not clearly known. There is hereditary predisposition. It is seen in cirrhotics and epileptics who takes sodium hydantoin and may also develop in diabetics.
- Treatment : Night splintage and gentle stretching by the patient and excision of fascia.
Ganglion:
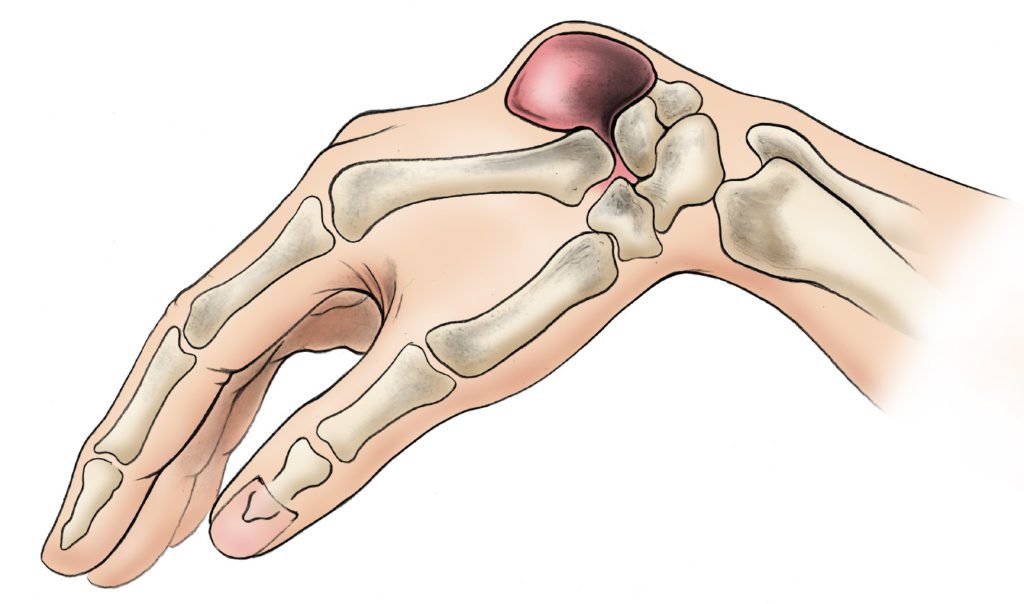
- This is a tense and cystic swelling containing gelatinous material in it.
- Mostly arises from the capsule of joint or tendon sheath.
- Commonly seen on the dorsum of the wrist or the palm of the hand.
- They are caused by the myxoid degeneration of fibrous tissue of capsule, ligaments and retinaculae, sometimes predisposed by injury.
- If it originates from a tendon sheath it can be moved sideways slightly but not at all along the length of the tendon particularly when the tendon is made taut.
There is chance of reccurence of ganglion after surgical excision.

26 Comments