
Ulnar Impaction Syndrome
Table of Contents
Definition
Ulnar Impaction Syndrome, also known as ulnar abutment syndrome, is a medical condition affecting the wrist and hand. It is characterized by chronic compression and wear of the ulnar side of the wrist joint, particularly between the ulna bone (one of the two forearm bones) and the carpal bones of the wrist. This impingement can lead to pain, inflammation, and decreased wrist function.
Ulnar impingement can cause irritation, inflammation, and wear and tear on adjacent structures, including the triangular fibrocartilage complex (TFCC), the ulnar styloid process, and the femur. Over time, this repetitive impact can cause pain, swelling, limited wrist motion, and possibly degenerative changes and wrist instability.
Epidemiology
Specific epidemiological data on ulnar impingement syndrome (UIS) were limited and prevalence rates were not established. UIS is relatively rare compared to other wrist and hand problems.
However, here are some general points related to the epidemiology of UIS based on the information available so far:
Incidence and Presence:
- UIS is considered rare compared to other wrist conditions.
- The exact incidence and prevalence varies between different population groups and may depend on several factors such as age, occupation, and level of physical activity.
- It is more commonly seen in people who deal with repetitive wrist strains, such as athletes and manual workers.
Age and gender:
- UIS can occur in people of any age but is most often diagnosed in young and middle-aged adults.
- There does not seem to be a significant gender predilection for this disease; both men and women can be affected.
Sports and professional associations:
- People who participate in sports or activities that involve repetitive wrist movements, such as gymnastics, weightlifting, and racquet sports, may be at a higher risk for UIS.
- Additionally, people who work in certain occupations that require repetitive stress on the wrist, such as construction workers or assembly workers, may also be at greater risk.
Anatomical factors:
Anatomical variations such as ulnar positive variance (when the ulna is longer than the radius) and changes in the ulnar styloid may predispose individuals to the development of UIS.
- It is important to note that epidemiologic data may change over time as more research is conducted and medical knowledge advances.
- For the most up-to-date and accurate information on the epidemiology of ulnar infarction syndrome, it is best to consult recent medical literature and research or seek guidance from health professionals or orthopedists.
Anatomy of ulnar impingement syndrome
Ulnar impingement syndrome (UIS) involves excessive contact and pressure between the ulna (ulna) and surrounding structures of the wrist. Understanding the correct anatomy is crucial to understanding how this condition can occur and its possible consequences. Here are the main anatomical structures involved in ulnar impingement syndrome:
Ulna:
- The ulna is one of two bones in the forearm, located on the medial (inner) side of the hand. It extends from the elbow to the wrist and runs parallel to the beam.
- At the distal end of the ulna is a bony projection known as the ulnar styloid process.
Radius:
- The radius is the second bone of the forearm, located on the lateral (outer) side of the hand.
- It also extends from the elbow to the wrist and plays an important role in forearm rotation.
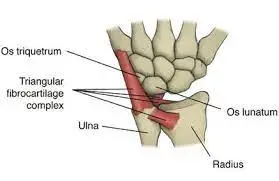
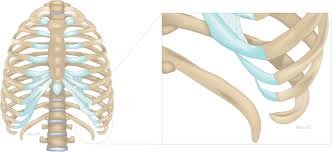
Triangular Fibrocartilage Complex (TFCC):
- The TFCC is a complex structure composed of cartilage, ligaments, and tendons.
- It is located in the ulnar part of the wrist joint and provides stability and support to the wrist.
- It connects the ulna to the wrist bone (carpal bone) and acts as a cushion and shock absorber.
Ulnar styloid process:
- This is a bony projection at the end of the ulna, on the opposite side of the radius.
- The ulnar styloid process can become involved if it is in excessive contact with surrounding structures, especially the TFCC, and talus.
Lunate Bone:
The Lunate is one of the eight bones in the wrist. It is located near the middle of the wrist and plays an important role in wrist movement.
- In ulnar impingement syndrome, anatomical factors such as ulnar positive variance, where the ulna is longer than the radius, can exacerbate the condition.
- This can lead to increased contact between the ulnar head and tibia, causing wear and tear on both structures. Repeated impact can also damage the TFCC, causing pain and inflammation.
- In addition, traumatic injuries or fractures to the carpus can also contribute to ulnar syndrome by changing the anatomy of the carpus and creating conditions that promote excessive contact between the ulna and surrounding structures.
- It is important to note that the anatomy and pathophysiology of ulnar impingement syndrome can be complex and vary from person to person.
- A full evaluation by a physician, such as an orthopedist, is necessary to ensure an accurate diagnosis of the condition and appropriate treatment.
Causes of ulnar impaction syndrome
The etiology of elbow impression syndrome (UIS) is multifactorial, meaning that it can be caused by a combination of different factors. The condition is primarily caused by excessive contact and pressure between the structures surrounding the ulna (ulna) and carpal bone. Too many factors may contribute to the development of elbow impingement syndrome:
Positive ulnar variance:
- One of the most important anatomic factors associated with UIS is ulnar positive variance.
- This occurs when the ulna is longer than the radius, resulting in increased contact between the ulnar head and tibia.
- This excessive exposure can wear down the joint cartilage and surrounding soft tissues, causing pain and inflammation.
Repetitive wrist strain:
- Participating in activities that involve repetitive wrist movements and strain can contribute to UIS.
- Athletes involved in sports such as gymnastics, weightlifting, and racquet sports, as well as those in certain occupations (such as manual workers), may be at increased risk due to repetitive stress on the wrist joint.
Traumatic injuries:
- Past injuries to the wrist, such as fractures or sprains, can alter the normal anatomy of the wrist and contribute to ulnar impingement syndrome.
- These injuries can cause changes in the alignment of the joint, increasing the probability of striking between the ulna and other structures.
Anatomic variations:
- Anatomic variations of the ulna, radius, or carpus can also affect UIS. For example, changes in the shape or size of the ulnar styloid process can affect the degree of impingement.
Trigeminal Cartilage Complex (TFCC) Instability:
- The TFCC is an important structure that stabilizes the ulnar aspect of the wrist joint.
- When the TFCC is damaged or unstable, it can cause changes in joint mechanics and increased impact forces between the ulna and other bones.
Inflammatory conditions:
Chronic inflammatory conditions such as rheumatoid arthritis can affect the wrist joint and contribute to ulnar syndrome.
- It is important to note that not everyone who has a positive ulnar variance or engages in repetitive wrist stress will develop ulnar syndrome.
- The condition can occur in people with a combination of risk factors or anatomical predispositions.
- Diagnosing the specific cause of elbow impingement syndrome requires a thorough evaluation by a physician, usually an orthopedist.
- Treatment depends on the severity of the condition and underlying factors and may include conservative measures (eg, rest, splints, physical therapy) or, in some cases, surgical procedures to treat anatomical problems.
Signs and symptoms
Ulnar impingement syndrome (UIS) can cause a variety of signs and symptoms, usually caused by excessive contact and pressure between the structures surrounding the ulna (ulna) and carpal bone. Symptoms may range from mild discomfort to too much pain and dysfunction. Common signs and symptoms of elbow impingement syndrome include:
Wrist pain:
Pain in the ulnar part of the wrist is one of the symptoms of UIS. The pain can be localized to the affected area or radiate to the ulna of the forearm.
Swelling:
Inflammation and irritation of the carpal structures can cause swelling around and next to the ulnar styloid.
Clicking or clicking:
Some people with UIS may experience clicking or clicking when moving the wrist, especially when turning or bending the wrist.
Limited wrist range of motion:
UIS can impair wrist mobility, especially on the ulnar side of the wrist. This limitation can prevent various activities and tasks that require wrist movement.
Weakness and grip problems:
In advanced cases, pain and changes in joint mechanics can cause weakness and reduced grip strength in the affected arm.
Tenderness to touch:
The ulnar side of the wrist may be tender to touch, especially over the ulnar styloid process and adjacent structures.
Pain from specific activities:
Pain and discomfort may worsen with activities that involve repetitive wrist movements, heavy lifting, or strong grip.
Worsening of symptoms over time:
Untreated, ulnar impingement syndrome can cause a gradual increase in symptoms, affecting daily activities and impairing overall wrist function.
- It is important to note that these symptoms can also occur with other wrist conditions, such as carpal tunnel syndrome, triangular fibrocartilage complex (TFCC) injuries, or other ligament problems.
- Therefore, an accurate diagnosis by a healthcare professional, usually an orthopedic specialist, is critical to distinguishing ulnar impingement syndrome from other wrist conditions and creating an appropriate treatment plan.
- If you suspect you have elbow impingement syndrome or have persistent wrist pain or related symptoms, see your doctor for a proper evaluation and personalized treatment recommendations.
- Early diagnosis and treatment can help prevent the condition from progressing and improve overall wrist function.
Differential diagnosis
When diagnosing elbow impingement syndrome (UIS), health professionals must consider several other conditions that affect the wrist with similar symptoms. Differential diagnosis of UIS includes:
Tears of the Triangular Cartilage Complex (TFCC):
TFCC injuries, like UIS, can cause pain, swelling, and limited wrist motion. TFCC tears are often caused by trauma or repetitive strain on the wrist.
Ulnar styloid fracture:
Fractures of the ulnar styloid process can cause localized pain on the ulnar side of the wrist and can be confused with UIS.
Ulnar ligament injury:
Injuries to the ulnar ligament of the wrist can cause pain in the ulnar part of the wrist, making it a possible differential diagnosis. Junction syndrome: This condition involves inflammation at the junction of the extensor and abductor tendons on the back of the wrist, but can cause pain that radiates to the ulna.
ECU Tendinitis:
Inflammation of the Extensor Carpi ulnaris (ECU) Tendon can cause pain and limited wrist movement, mimicking the symptoms of UIS.
Pisotriquetral Joint Dysfunction:
Dysfunction or inflammation of the ulnar joint near the ulna can cause pain in the ulnar region of the wrist.
Ulnar neuropathy:
Compression or entrapment of the ulnar nerve can cause symptoms similar to UIS. This condition can cause tingling, numbness, and weakness on the ulnar side of the arm.
Rheumatoid arthritis:
Inflammatory joint diseases such as rheumatoid arthritis can affect several joints, including the wrist, and cause symptoms similar to UIS.
Kienböck disease:
This condition involves avascular necrosis of the ulna, causing pain and limited wrist motion that can be mistaken for UIS.
Carpal tunnel syndrome:
Although carpal tunnel syndrome primarily affects the median nerve, it can also cause symptoms that radiate to the ulna in the wrist.
De Quervain’s tenosynovitis:
This condition involves inflammation of the tendons in the thumb and wrist area, causing pain on the radial side of the wrist.
- An accurate diagnosis of impingement elbow syndrome requires a thorough evaluation by a healthcare professional, such as an orthopedist, who takes the patient’s medical history, performs a physical exam, and may order imaging tests such as X-rays, MRIs, or ultrasounds to confirm the diagnosis and rule out other possible conditions.
- Once the diagnosis is confirmed, an appropriate treatment plan can be developed to treat the specific condition and relieve symptoms.
Diagnosis
A diagnosis of elbow impingement syndrome (UIS) requires a thorough evaluation by a healthcare professional, usually an orthopedist. The process may include the following steps:
Examination
- A full wrist examination should be performed to diagnose impingement elbow syndrome.
- Diagnostic imaging should be performed to support the results of the clinical examination.
- A physiotherapist should pay particular attention to the following:
Palpation
- Dorsal tenderness distal to the end of the ulna
- Tenderness involving only the ulnar styloid process
- Positive ulnar dispersion, while static or dynamic
Range of motion
- Painful passive deviation and severe pronation of the ulna
- Decreased flexion, extension, radial and ulnar deviation
Strength
- The reduced grip on the dynamometer
Ulnocarpal stress test
- Place the wrist at the greatest deviation of the ulna
- Place an axial load on the wrist
- Passively rotate the forearm through supination and pronation
- Test = increase in patient pain NOTE. The test is sensitive for UIS but may be positive for other conditions such as LTIL injury, TFCC injury, or isolated arthritis.
Grip Rotation Impact Test (GRIT)
- Place your hand’s side by side with your elbow bent at 90 degrees
- Use a grip dynamometer to measure grip in three positions: neutral, full supination, full pronation
- GRIT ratio = (supinated grip strength) / (pronated grip strength)
- A GRIT ratio more eminent than 1.0 indicates UIS
Examination of the integrity of the TFCC may be necessary, especially in patients suspected of having long-term ulnar impingement syndrome due to the commonly observed degeneration of this structure.
Physician:
- The physician begins by taking a detailed medical history, including questions about past wrist injuries, repetitive wrist-bearing activities, and the onset and duration of symptoms.
- They also ask about illnesses or past problems with the wrist.
Physical Examination:
- A physical examination of the affected wrist is performed.
- The doctor evaluates the range of motion of the wrist, and checks sensitivity, swelling, and possible deformations.
- They may also perform special tests to assess the stability and integrity of the wrist structures.
Imaging studies:
- X-rays are often the first imaging study done to evaluate the bony structures of the wrist.
- X-rays can help detect ulnar positive variance, fractures, or other bone-related abnormalities.
- In some cases, an MRI (magnetic resonance imaging) or ultrasound may be recommended to visualize soft tissues such as the trigeminal cartilage complex (TFCC) and evaluate for possible ligament damage or tears.
Diagnostic injections:
- In some cases, the doctor may give diagnostic injections, such as a local anesthetic injection, to confirm the source of the wrist pain.
- If the pain improves significantly after the injection, this indicates that the cause of the symptoms is probably an impact or irritation of the structures in the ulna.
Electromyography (EMG) and nerve conduction studies:
- If a doctor suspects ulnar neuropathy (compression of the ulnar nerve), EMG and nerve conduction studies may be ordered to evaluate nerve function and rule out other possible causes of symptoms.
- Once the ulnar infarction syndrome is diagnosed, a treatment plan can be determined.
- Treatment may include conservative measures such as rest, wrist weights, physical therapy, and anti-inflammatory medications to reduce pain and inflammation.
- In cases where conservative therapy does not provide relief, a surgical procedure may be considered to address the anatomical problems underlying UIS.
- For an accurate diagnosis and appropriate treatment, it is very important to see a doctor in time for persistent wrist pain or related symptoms, because early intervention can help prevent the condition from progressing and improve the overall function of the wrist.
Medical treatment
Medical treatment for elbow impingement syndrome (UIS) aims to relieve symptoms, reduce inflammation and improve wrist function. The specific treatment method may vary depending on the severity of the condition and individual patient factors. Here are some commonly used treatment options at UIS:
Rest and activity modification:
Reducing or avoiding activities that worsen symptoms can promote healing and reduce inflammation. Rest time may be recommended to give the wrist time to heal.
Immobilization:
- A wrist cast or brace may be prescribed to support and limit wrist movement, allowing the damaged structures to heal.
- These devices are usually worn for a period of time and can be removed during a specific activity or physical therapy session.
Nonsteroidal anti-inflammatory drugs (NSAIDs):
- Drugs such as ibuprofen or naproxen can help reduce the pain and inflammation associated with UIS.
- However, long-term or excessive use of anti-inflammatory drugs should be discussed with a doctor due to possible side effects.
Corticosteroid injections:
- In some cases, a doctor may inject corticosteroids directly into the affected area to reduce inflammation and provide short-term pain relief.
- However, these injections are used with caution because they can weaken tissue with repeated use.
Physical therapy:
- A physical therapist can design specific exercises to strengthen the wrist, improve range of motion, and improve wrist stability.
- Physiotherapy can be useful both during conservative treatment and after surgical procedures.
Occupational therapy:
An occupational therapist can provide guidance on ergonomics and adaptive methods in daily life to reduce stress on the wrist.
Shock wave therapy:
Extracorporeal shock wave therapy (ESWT) is a non-invasive therapy that uses elevated-energy shock waves to stimulate recovery in the affected area. It has been investigated as a potential treatment for UIS.
Plasma (PRP) Therapy:
- PRP therapy involves the use of the patient’s own blood components that are rich in growth factors to promote healing and tissue repair.
- It is being studied as a potential treatment for UIS, although further research is needed.
Ultrasound-guided hydrosilation:
This procedure involves injecting fluid into the wrist joint to separate the bones and reduce shock. Some UIS have this promise.
- If conservative treatment does not provide sufficient relief and the condition significantly affects daily activities and quality of life, surgical treatment may be considered. Surgical procedures for UIS may include addressing anatomic factors contributing to numbness, such as ulnar shortening osteotomy, ulnar cap resection, or TFCC repair.
- It is important to consult with a qualified healthcare professional or orthopedist to determine the most appropriate treatment plan based on a person’s specific condition and needs.
- Early intervention and appropriate treatment can lead to better outcomes and wrist function in people with ulnar impingement syndrome.
Physiotherapy treatment
Physiotherapy plays a vital role in the treatment of ulnar impaction syndrome (UIS). A skilled physiotherapist can design a comprehensive rehabilitation program to address pain, inflammation, and functional limitations associated with UIS. The goals of physiotherapy for UIS are to reduce symptoms, improve wrist mobility and strength, enhance wrist stability, and promote a safe return to functional activities. Here are some common physiotherapy treatments for ulnar impaction syndrome:
Range of Motion Exercises:
Range of motion: Gentle, controlled exercises may be prescribed to maintain or improve wrist range of motion. These movements help prevent stiffness and improve flexibility. Wrist exercises may help enhance flexibility, relieve stiffness, and maintain wrist health. Below given are some simple exercises to promote a full range of motion in your wrist:
Wrist flexor stretch:
- Keep the palm of the hand facing forward.
- With the other hand, gently pull the fingers back until you feel a stretch in the wrist and forearm.
- Hold the stretch for 10-20 seconds, then switch and repeat with the opposite arm.
- Do 2-3 repetitions for each arm.
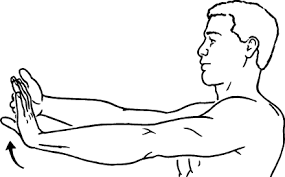
Wrist Stretch:

- Begin by extending your arms in front of you, palms facing down.
- Then gently pull your other hand back until you feel a stretch in the back of your wrist and forearm.
- Hold the stretch for 10-20 seconds, then switch to the other arm and repeat.
- Do 2-3 repetitions for each arm.
Wrist pronation and supination:
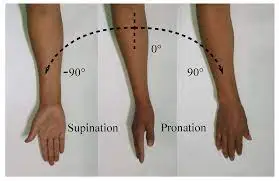
- Sit or stand with the arms at the sides and elbows at a 90-degree angle.
- Keep the palms facing the ground and then slowly rotate your arms outward so that your palms are facing up (supination).
- Then turn your hands inward so your palms are facing down (lying down).
- Do 10-15 repetitions in both directions.
Wrist circles:
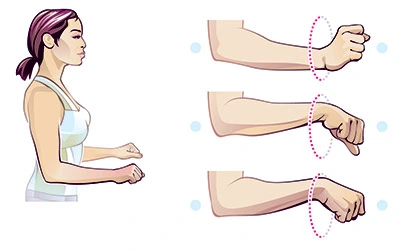
- Reach out and place your hands in front of you, fingers up.
- Start by making small circular motions with your wrist and gradually expand the circles as you go.
- Reverse the direction of movement after 5-10 seconds.
- Do 2-3 sets in both directions.
Wrist flexion and extension:
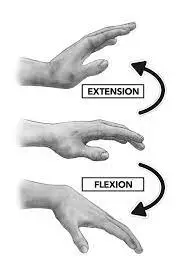
- Sit or stand with the arms at the sides and elbows at a 90-degree angle.
- Bend the wrists up (flexion) and then down (extension), moving your arms toward the ceiling and floor.
- Do 10-15 repetitions of wrist flexion and extension.
- Acknowledge the performance of these movements gradually and carefully, without movements.
- If you experience pain or discomfort while exercising, stop exercising and consult a doctor or qualified physical therapist before continuing.
- Traditional wrist exercises can help maintain wrist flexibility, reduce the risk of stiffness, and improve overall wrist function. If you have a wrist condition or injury, you should consult a doctor or physical therapist before starting an exercise program to make sure the exercises are appropriate for your needs.
Strengthening exercises:
Strengthening the muscles near the wrist joint may provide adequate support and stability. Physical therapists can use resistance training or progressive resistance exercise to target exact muscles in the forearm and hand. Wrist-strengthening exercises may help improve wrist stability, grip strength, and overall function. It is necessary to do these exercises correctly and begin with light resistance, gradually it as strength improves. Here are some effective wrist-strengthening exercises:
Wrist curls (flexion and extension):

- Find a chair to sit on or stand with one hand on a flat surface, such as a table.
- Make sure your palm is facing up.
- Take a light dumbbell or a common household object such as a soup can and hold it in your hand.
- Slowly bend the wrist upwards, bringing the weight into the body (flexion).
- Lower the weight back to the starting position. Do 10-15 repetitions in 2-3 sets.
- Repeat with the other hand.
Wrist deviation (radial and ulnar):
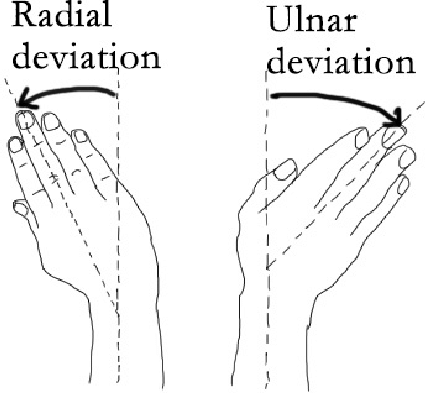
- Sit in a chair or stand straight, forearms on a flat surface, palms down.
- Keep a light bulb or household items.
- Gently bend the wrist to the thumb (radial deviation) and then to the pinky (elbow deviation). Do 10-15 repetitions for 2-3 sets.
- Repeat with the other hand.
Grip Strengthening – Hand Exercise:

- Hold your palm up.
- Squeeze the handle, engaging your hands and forearm muscles.
- Hold the handle for a few seconds and then release it slowly.
- Do 10-15 repetitions in 2-3 sets.
- Repeat with the other hand.
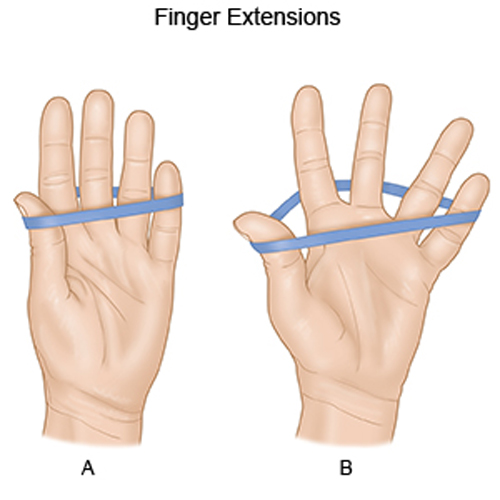
Finger flexion exercise:

- Place your forearm on a flat surface with the palm facing down and the fingers extended.
- Put a rubber band around the fingers.
- While squeezing the rubber band, gradually bend the fingers.
- Return the fingers to the starting position.
- Do 10-15 repetitions in 2-3 sets.
Wrist Roll Exercise:

- Attach a light stake to the end of a pin or stick and tie it with string or thread.
- Hold the stick with both hands, palms down.
- Rotate the weight by turning the needle with your wrists and bring the weight towards you.
- Calculate the weight by inverting the needle.
- Do 5-10 repetitions in 2-3 sets.
Make sure you do these strengthening exercises under control and try to avoid overloading the wrist joints. If the person experiences pain or discomfort, reduce resistance or stop the movement and consult a doctor or qualified physical therapist. Additionally, if a person has a wrist condition or injury, it is necessary to obtain permission from a health practitioner before beginning strength training.
Finger squeezes:
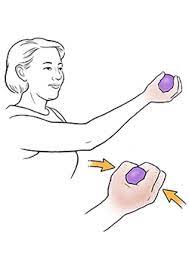
- Put a soft foam or rubber ball in the palm of the hand.
- Squeeze the ball as hard as a person can with all the fingers.
- Keep the pressure for a few seconds and then release.
- 10-15 times with each hand.
Finger extensions:
- Extend your fingers as far as possible.
- Hold the movement for a few seconds and then relax.
- Repeat 10-15 times with each hand.
Thumb opposition:

- Do this exercise by forming an O shape with your thumb and touching the tip of each finger separately with the tip of your thumb.
- Repeat this movement with each finger.
- Repeat this sequence 10-15 times with each arm.
Hand grip exercise:
- Keep the grip in the hand with the palm facing up.
- Squeeze the handle while using your hand and forearm muscles.
- Hold the handle for a few seconds and then release it slowly.
- Do 10-15 repetitions for each arm.
Wrist extension with resistance band:
- Place your arm, palm down, on your thigh while sitting on a chair.
- Tie the resistance band around your fingers and thumb.
- Extend your wrist back, pulling the resistance against the strap.
- Return to the starting position with control.
- Do 10-15 repetitions for each arm.
Finger pinch:

- Place a small object (such as a coin or a small ball) between the tips of your thumb and forefinger.
- Press your thumb and finger together to hold the target.
- Maintain for a few seconds, then relax.
- Repeat 10-15 times with each hand.
Tapping the table:
- Raise your arms flat on a table or platform.
- Raise each finger individually by tapping it against the table while keeping the others down.
- Repeat tapping with each finger one at a time.
- Perform 10-15 repetitions for every finger with both hands.
Elbow strengthening exercises may help enhance the stability, function, and overall strength of the muscles surrounding the joint. Below given are some effective exercises to strengthen your elbows:
Bicep curls:

- Hold a dumbbell or resistance band with your palms facing forward.
- Keeping your upper arm still, slowly bend your elbow by bending the weight or pulling the strap toward your shoulder.
- Hold the contraction for a second, then gradually lower the weight or release the tension on the band. Repeat 10 to 15 times.
- Start with a weight or resistance level that challenges the individual but allows for proper form.
Triceps extensions:
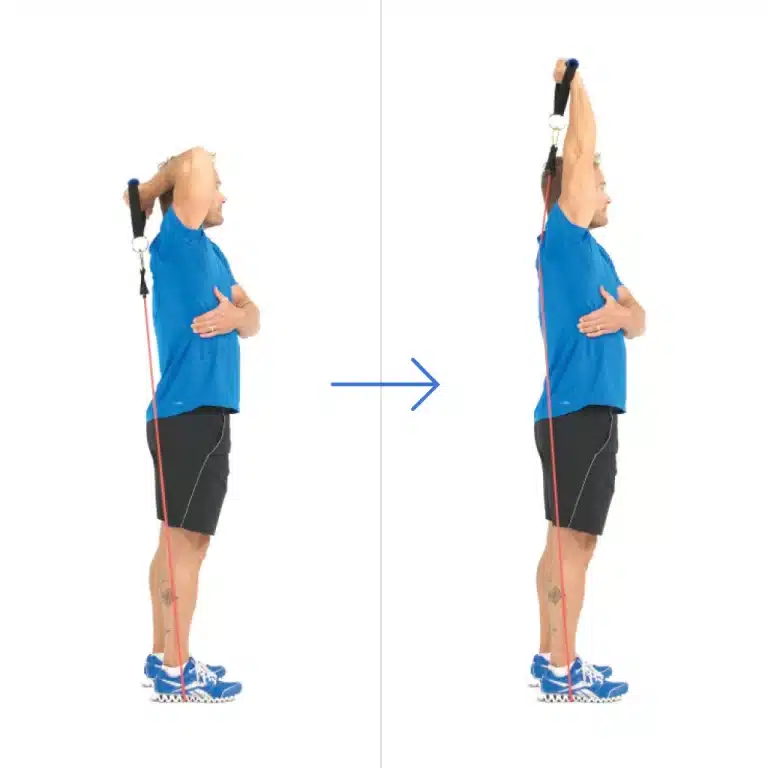
- Hold the dumbell in your hand, palm down.
- Extend the arm fully above the head, keeping the upper arm still.
- Slowly bend your elbows, lowering the weight behind your head or onto your shoulders.
- Keep the contraction for a second and then extend the arms back to the initial position.
- Repeat as many times as you want.
- Adjust the weight as needed.
Push-ups:
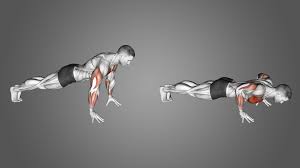
- Begin in a plank position with the hands slightly shoulder-width apart.
- Lower your body to the ground by bending your elbows, keeping them close to your sides.
- Press your hands back to the starting position.
- Repeat as many times as you want.
- Change the intensity by doing push-ups on the knees or against the wall as needed.
Reverse Wrist Curls:

- Sit in a chair with your hands on your thighs, palms down.
- Hold a rune or weighted object.
- Slowly bend your wrists down and bring your body weight to the floor.
- Hold the contraction for a second and then gradually raise the weight back up.
- Repeat as many times as you want. Adjust the weight as needed.
It’s essential, to begin with a weight or resistance level that allows a person to maintain proper form while still challenging her muscles. Do these exercises with controlled movements and focus on muscle contractions.
If you feel pain or discomfort, reduce your weight or resistance or seek advice from a doctor or qualified physiotherapist. Don’t forget to warm up before doing strength exercises, and take adequate rest and recovery between exercises. Slowly increase the weight, resistance, or intensity over time as the strength improves.
Proprioception and Balance Training:
Proprioceptive exercises improve joint position sense and stability. Balance training can be added to improve wrist stability during various functional movements.
Modalities:
A physical therapist may use therapeutic methods such as ultrasound, heat, or cold therapy to reduce wrist pain and inflammation.
Manual therapy:
Practical techniques such as soft tissue mobilization and joint mobilization can be used to improve tissue flexibility and joint function.
Activity Modification and Ergonomic Advice:
physical therapist can guide you in modifying daily activities and tasks to reduce stress on the wrist and improve ergonomics.
Taping and Bracing:
Taping techniques or custom splints may be used to provide support and stability to the wrist during activities.
Progressive Rehabilitation:
The physical therapist will gradually progress the exercises and activities as the wrist heals and modify the treatment plan based on the individual’s response.
It is important to note that physical therapy for elbow impingement syndrome must be individualized based on the patient’s specific condition, level of pain, functional limitations, and general health. In addition, physical therapy may be more effective when combined with other medical treatments, such as rest, anti-inflammatory medications, or corticosteroid injections, as recommended by a physician.
Adherence to the prescribed exercises and adherence to the physical therapy program is essential for positive results in the treatment of ulnar impingement syndrome. If symptoms persist or worsen despite physical therapy interventions, further evaluation by a physician may be necessary to explore other treatment options.
Post-surgery physiotherapy exercise protocol
| Timeframe | Goals | Bracing/splinting | Therapeutic exercise | Control pain & swelling Protect surgical site Maintain ROM in unaffected jets | |
| 0-2 weeks | Control pain & swelling Protect surgical site Maintain ROM in unaffected joints | Sugar-tong splint Long-arm cast | NWB Elevation for edema | – | |
| 2-6 weeks | -Protect surgical site -Maintain ROM in unaffected jts -Increase elbow & wrist ROM -Scar management | -Removable elbow-hinged splint or wrist cock-up brace – | -Limited wrist & forearm ROM -outside splint Stretching of elbow & wrist -Avoid loaded pronation & supination -Continue shoulder & digit ROM | -soft tissue mobilization | |
| 6-8weeks | Increase elbow & wrist ROM Increase UE strength Scar management | Removable splint worn at night – See above – as needed | Full AROM of elbow & wrist Stretching of elbow & wrist Isometric elbow flex/ext & supination/pronation | -Soft tissue | |
| 8-12 weeks | Address remaining ROM & strength impairments | -Splint may still be worn at night | Full AROM of elbow & wrist UE strength training | -Soft tissue massage Mobilization of elbow forearm & wrist |
FAQ
However, the signal changes in Kienböck’s disease are more diffuse or severe on the six radial sides. In addition, ulnar impingement syndrome affects the ulnar head and triquetrum, which are intact in Kienböck’s patients.
Stage 3: In stage 3, your hardened madness begins to crack. This can cause other bones in the wrist to move. You feel more pain, you have difficulty grasping things with the same force, and your range of motion is limited. Stage 4: In stage 4, the outer surfaces of the bones near your moon also weaken.
An abstract. Ulnar abutment (ulnar carpal impact) syndrome can be a source of ulnar wrist pain in athletes. This condition is caused by excessive load transfer between the triangular fibrocartilage complex and the ulnocarpal joints and is characterized by degenerative changes.
It is recommended that you do NOT use your hand for any work or self-care tasks for about 6-8 weeks, depending on what type of work you are returning to. Doing it too soon can change the placement of the hardware or cause misalignment of the ulna.
The success rate of ulnar nerve graft surgery is remarkable, with over 85% of patients making a full recovery. Assume a seated or standing position with your arms resting at your sides and your elbows forming a 90-degree angle. Proceed to bend your wrists upwards (flexion) and then downwards (extension), gradually moving your arms towards the ceiling and floor.

4 Comments