

Phantom limb pain
Table of Contents
What is phantom limb pain?
Phantom limb pain is defined as pain in the limb after an amputation. Some people experience pain in the part of the limb that is no longer present. This type of sensation is phantom limb pain. The pain is real. It is most common in arms and legs, but some people will feel it when they have other body parts removed, such as a breast. The phantom part directs to the location of the pain: the missing limb or part of the limb such as fingers or toes.
Phantom limb pain can happen after a surgical procedure that amputates the limb. The amputation may have been required for some unrelated reason, such as a traumatic injury or disease. The phantom limb pain is due to the effect of the surgery.
Phantom pains are often described as crushing, toes twisting, hot iron, burning, tingling, cramping, shocking, shooting, and “pins & needles”
Tends to localize to more distal phantom structures for e.g. fingers and toes
Prevalence in the early stages is 60-80 percent.
Liberated of age in adults, gender, level, or side of amputation.
For some people, the pain will go away on its own in some days. For others, it can be long-lasting and get severe.
Phantom limb pain varies from mild to severe and can last for seconds, hours, days, or longer. It may occur after a surgical method including amputation (removing part of a limb with surgery). It can also happen after accidental amputation when you lose a finger, toe, or other body parts. Phantom pain can be controlled.
Difference between phantom limb pain, phantom sensation, and residual limb pain
With phantom pain, a person senses pain where the missing body part should be. Other problems associated with losing part of the body involved:
Phantom sensations: Phantom sensation occurs the missing limb or extremity still feels like it’s part of the body. There is no pain. A person may experience phantom sensations may forget that part of a lower limb is missing and try to walk on both legs.
Residual limb pain: Residual limb pain affects the remaining part of the limb (stump) where the amputation occurred. Residual limb pain usually has a medical reason, such as nerve damage or entrapment (pressure on the nerve). It impacts approximately 7 in 10 people with limb loss.
Causes of Phantom limb pain:
Phantom pain typically occurs soon after limb loss. It can take 3 – 6 months for a wound to heal after amputation. Infrequently, the pain comes on months or years later.
Phantom pain results from a mix-up in signals from the nervous system, specifically between the spinal cord and the brain. When a body part is removed, the nerve connections from the periphery to the brain stay in place. The brain can misunderstand or misinterpret the information it’s receiving or process the signals as the sensation of pain, even if the amputated portion has since been removed.
There are considerable theories about the causes of phantom limb pain including peripheral, central, and spinal theories:
Peripheral Theories
The remaining nerves in the stump grow to develop neuromas, which provoke impulses. These impulses are sensed as pain in the limb that has been removed.
After transitions in the severity of phantom limb pain were noted in different temperatures, another theory says that cooling of the nerve endings raises the rate of firing of the nerve impulses, which are sensed by the patient as phantom limb pain
Central Theories
Melzack proposed that the body is described in the brain by a matrix of neurons. Sensory experiences make a unique neuromatrix, which is impressed on the brain. When the limb is removed, the neuromatrix tries to reorganize it, but the neuro signature remains due to the chronic pain experienced previous to the amputation. This causes pain which is phantom limb pain after amputation.
Spinal Theories
When peripheral nerves are excised during amputation surgery, there is a loss of sensory input from the area below the level of limb amputation. This decrease in neurochemicals alters the pain pathway in the dorsal horn
Risk factors:
Factors associated with a higher risk of developing phantom limb pain include:
- Pain may occur prior to amputation.
- Pain prior to amputation may be of higher intensity and longer duration.
- Upper-limb amputation
- More in the Female gender
- Higher chance in Older age
- Residual pain in the non-amputated part of the extremity
These factors may trigger phantom limb pain:
- Angina (pain in the chest due to low oxygen to the heart)
- Changes in temperature or barometric pressure
- Constipation
- Shingles (herpes zoster) condition
- Sex or physical touch
- Smoking habit
- Stress
Symptoms of Phantom limb pain:
Phantom pain symptoms may be fleeting or last for some days. During the first six months after a limb loss, the intensity of pain and frequency usually decrease. Still, as many as 8 out of 10 people continue to have phantom pain two years after amputation
The phantom pain in a patient may feel like:
- Burning or aching-like.
- Clamping, pinching, or vise-like.
- Itching or tingling-like.
- Shooting or stabbing-like.
- Throbbing pain.
- Twisting pain.
Phantom pain affects the sensation of pain in a part of the body that has been removed.
The onset of phantom pain can happen within the first some days of amputation. The sensation may occur and go but it may be continuous. While the sensation often, affects the part of the limb most distant from the body, such as the foot of an amputated leg, other body parts nearest to the brain such as the arm or hand, can still experience parallel sensations. Sensations can be characterized as shooting, stabbing, boring, squeezing, throbbing, or burning. Sensations on smaller limbs and digits such as toes or fingers feel to be less painful. Sometimes the sensation feels as if the phantom limb is forced into an awkward position. All around, the sensations may be triggered by pressure on the remaining part of the limb or emotional stress.
Types:
There are various types of sensations that may be felt in phantom limbs:
- Sensations connected to the phantom limb’s posture, length, and volume. For example., feeling that the phantom limb is acting just like a normal limb like sitting with the knee bent or feeling that the phantom limb is as heavy as the other limb. Sometimes, an amputee person may experience a sensation called telescoping, the feeling that the phantom limb is gradually shortening over time.
- Sensations of movement in the foot (for example, feeling that the phantom limb is moving).
- Sensations of touch, temperature, pressure, and itchiness in the foot. Many amputees report feeling heat, tingling, itchiness, and pain sensation.
- In less extreme cases where small digits are amputated, the sensation can be described as a tingling feeling as opposed to a painful sensation.
Diagnosis:
The diagnosis of Phantom Limb Pain is primarily a diagnosis of exclusion and is heavily dependent on the patient’s history. Because of this, lab tests are often not required. A complete blood count (CBC) can help rule out any infection. A doctor may order tests to rule out causes of residual limb pain, like infections An ultrasound can be ordered to look for neuromas as a possible pain generator. A psychological evaluation may be indicated if the patient is having a considerable amount of external triggers that may be donating to his or her pain.
Treatment of Phantom limb pain:
Treatment for phantom limb pain focuses on relieving symptoms. They include:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) or prescription pain relievers: the effectiveness of certain opioids such as tapentadol for Neuropathic pain and Phantom Limb Pain, they should be used in conjunction with antidepressants or neural modulating agents (i.e., gabapentin, pregabalin). Furthermore, their use in a condition of benign pain should be done with caution in order to avoid potential effects from patience and dependence.
- Antidepressants: Commonly used for addressing PLP. Amitryptiline, in particular, tends to be the tricyclic antidepressant (TCA) of choice as it has shown the best overall results
- Anticonvulsants are thought to work by quieting damaged nerves so the pain signals are either slowed down or blocked.
- Antiseizure medications
- Beta-blockers
- Muscle relaxant
- Injections: Botulinum toxin type B injections have been used to treat hyperhidrosis (excessive sweating) in the post-amputation patient. Hyperhidrosis can not only restrict the use of a prosthetic but can adversely affect the course of both the phantom limb and RLP(Residual limb pain). Treatment of hyperhidrosis with botulinum toxin type B injections has been shown in several small studies to reduce RLP, PLP, and sweating. Botulinum toxin type A is also being studied, but so far has not been shown to reduce pain intensity compared to lidocaine/methylprednisolone.
Physical Therapy in Phantom limb pain
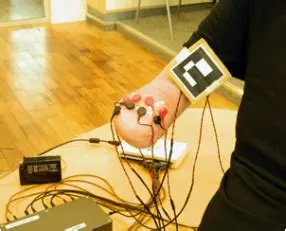
Treatments that send electrical impulses to the nerves, brain, or spinal cord may help reduce the pain. These treatments include:
- Neurostimulation.
- Spinal cord stimulation.
- Transcutaneous electrical nerve stimulation (TENS): Low-frequency and high-intensity are thought to be the most effective for PLP. It may also be used to help relieve Residual Limb Pain.
These complementary therapies may also reduce phantom pain:
- Acupuncture: In acupuncture, there is the release of endorphins that react with neurotransmitters in the brain to reduce pain. Acupuncture and dry needling can also help start and relax the muscles of the residual limb.
- Biofeedback.
- Massage: Massage to the limb will increase blood in the limb and reduce pain.
- Meditation
- Mindfulness or relaxing exercises.

It is effective for numerous individuals with one amputation and involves placing a mirror to reflect the image of the sound limb. Moving the lower limb or hand of the sound limb while looking at the reflection in the mirror makes the brain think it is moving both the sound limb and the phantom limb, helping to reduce uncomfortable feelings and pain from the amputated limb.
Mirror box therapy allows for illusions of movement and touches in a phantom limb by generating somatosensory and motor pathway coupling between the phantom and real limb. Many patients feel pain as a result of a clenched phantom limb, and because phantom limbs are not under voluntary control, unclenching becomes not possible. This theory suggests that the phantom limb feels paralyzed because there is no feedback from the phantom limb to return to the brain to inform it otherwise. If the brain received visual feedback that the limb has a movement, then the phantom limb would become not paralyzed.
A course of treatment of four weeks of mirror therapy may reduce chronic pain. Contraindications and side effects are few. The mechanism of action of mirror therapy remains undecided, with the reintegration of motor and sensory systems, restored body image, and control over fear avoidance likely to influence the result. The evidence for the clinical efficacy of mirror therapy is hopeful, but not yet final. Nevertheless, mirror therapy is affordable, safe, and easy for the patient to self-administer.
Visualization works similarly to mirror therapy. Envision the limb and fire the muscles in that limb. Stretch fingers or toes and imagine the extremity responding.
Deep-brain stimulation: Deep-brain stimulation is a surgical procedure used to relieve patients from phantom limb pain. Prior to surgery, patients undergo functional brain imaging techniques such as PET scans and functional MRI to decide an appropriate trajectory of where the pain is originating. Surgery is then assumed out under local anesthetic because patient feedback during the operation is required. A radiofrequency electrode with four contact points was put on the brain. Once the electrode was in place, the contact locations were changed slightly according to where the patient sensed the greatest relief from pain. Once the location of maximal relief was selected, the electrode was implanted and secured to the skull. After the primary surgery, a secondary surgery beneath general anesthesia was conducted. A subcutaneous pulse generator was implanted into a pectoral pocket down the clavicle to stimulate the electrode. The pain had not been entirely eliminated, but the intensity had been decreased by over 50% and the burning component had completely disappeared.
Heat, cold and manual manipulation:
- Cover the residual limb in a warm, soft towel.
- Cover the residual limb with a heating pad.
- Cover the remaining limb in a cold pack or apply a cooling cream or gel:
- Massage the residual limb with a textured material such as a towel or different clothes.
- Apply an elastic bandage to the limb.
- Change the limb position.
- Soak the limb in a warm bath.
- Tighten the muscles in the residual limb and slowly free them.
Summary:
Phantom limb pain/sensation is expected for most people after amputation surgery. Symptoms generally improve over a long time. The phantom limb pain/sensation can be managed so that it does not overwhelm the person’s life. The goal of pain management is to reduce pain levels and to allow a person to get back to living and enjoying life again. Work closely with the healthcare team to create and maintain the pain management plan that works for the person.
FAQs:
What do phantom pains feel like?
The symptoms which often characterize phantom pain: Pain expressed as burning, shooting, twisting, and crushing, like an electric shock or like “pins and needles.” Symptoms affect the part of the limb farthest from the body. Incessant pain or at times may experience pain that comes and goes.
Can phantom limbs be cured?
Presently, there is no efficacious treatment for chronic phantom limb pain, despite its devastating effects on the quality of life of most people following an amputation. Although this patient population is small, a novel and non-opioid treatment can’t come fast enough for HEAL researchers and providers.
What can trigger phantom pain?
Factors that may trigger phantom limb pain are Angina (chest pain due to low oxygen to the heart). Modifications in temperature or barometric pressure, Constipation.
Does phantom pain ever stop?
Phantom pain in the limb does go away with time. Many people find their pain has reduced by about 75 percent or more within the two years after amputation surgery. If the pain not decreases, talk to a doctor. An underlying problem may be activating the sensation, such as a neuroma (nerve overgrowth).
How long does the phantom limb last?
This is different for everyone. For most people the sensations diminish over the course of a few weeks or a few months – they become weaker and happen less. The character of the phantom feelings may change too



One Comment