
Carpal bone
Table of Contents
Introduction
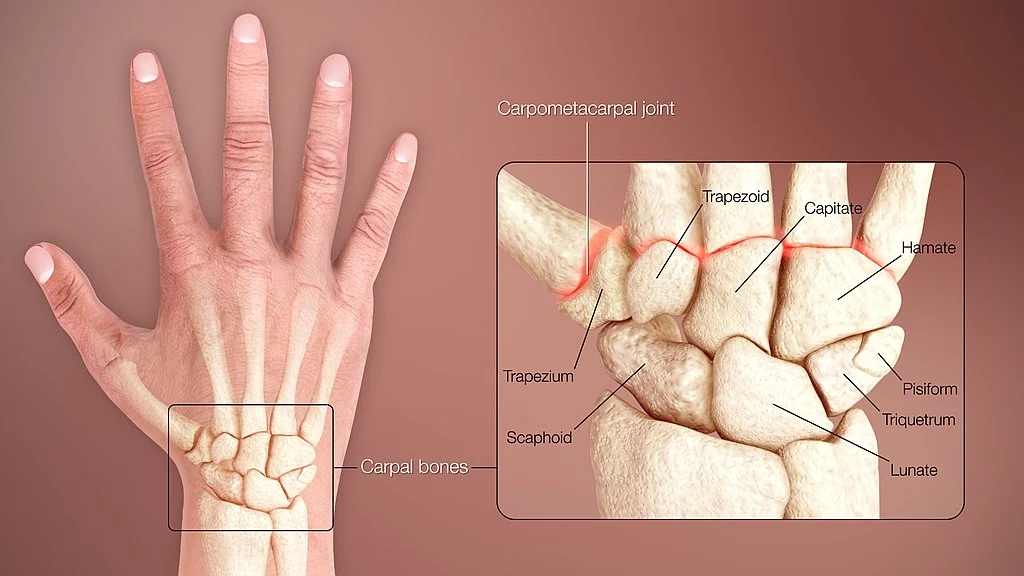
The carpal bones are a group of eight small bones located in the wrist between the radius and ulna (forearm bones) and the metacarpal bones (hand bones). These bones are arranged in two rows, with four bones in each row.
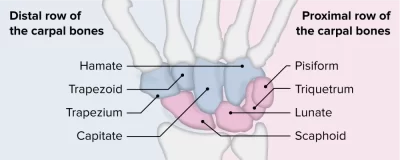
The names of the carpal bones, from lateral (thumb) to medial (pinky), in the proximal row are:
- Scaphoid (navicular) bone
- Lunate bone
- Triquetral (triangular) bone
- Pisiform bone
The names of the carpal bones, from lateral to medial, in the distal row are:
- Trapezium bone
- Trapezoid bone
- Capitate bone
- Hamate bone
These bones are connected to each other by strong ligaments, which provide stability to the wrist joint. They also have numerous articulations with other bones in the wrist and hand, allowing for a wide range of movements such as flexion, extension, abduction, adduction, and circumduction of the wrist.
Proximal row
bone are a scaphoid bone, lunate bone, triquetrum bone, pisiform bone.
Distal row
bone are a trapezium bone, trapezoid bone, capitate bone, hamate bone.
Mnemonic
- She – Scaphoid
- Likes – Lunate
- To –Triquetrum
- Play – Pisiform
- Try – Trapezium
- To – Trapezoid
- Catch – Capitate
- Her – Hamate
The carpal bones are eight irregularly-shaped bones located in the wrist area. These bones associate the distal part of the long forearm bones (radius and ulna) with the proximal parts of the metacarpal bones.
The carpal bones are classified into two columns: proximal and distal. the proximal column of carpal bones (from radial to ulnar) possesses the pisiform bone, scaphoid bone, lunate bone, and triquetrum bone. The distal column comfortable the trapezium bone, trapezoid bone, capitate bone, and hamate bones. Unique carpal bone has an amazing shape and is multifaceted, indicating that it can communicate with several wrapping bones, muscles, and ligaments of the forearm and hand. This way, the carpal bones supply flexibility and different types of movements to the soft tissues of the hand. they deliver the adultness of the skeletal framework of the wrist that supports the choice of the various neurovascular structures of the hand.
Structure
The eight carpal bones could be managed as either two transverse columns. When evaluated as paired rows, each row creates a turn that is convex proximally line and concaves distally. On the palmar side, the carpus is concave and includes the carpal tunnel, protected by the flexor retinaculum.
The proximal row (comprising scaphoid bone, lunate bone, triquetrum bone, and pisiform bone) articulates with the surfaces of the radius and distal carpal row, and therefore always adjusts to these mobile surfaces. Within the proximal row, per carpal bone has small independent mobility. for example, the scaphoid donates to middle-carpal bone strength by expressing distally with the trapezium and the trapezoid. In difference, the distal row is more difficult as its transverse arch forces with the metacarpals.
Clinically and biomechanically, the carpal bones are well conceptualized as 3 longitudinal columns:
Radial scaphoid column: scaphoid bone, trapezium bone, and trapezoid bone.
Lunate column: lunate bone and the capitate bone.
Ulnar triquetral column: triquetrum bone, and hamate bone In this context, the pisiform is followed as a sesamoid bone implanted in the tendon of the flexor carpi ulnaris.
The ulnar column has an opening between the ulna and the triquetrum; consequently, only the radial or scaphoid bone and prominent or capitate bone columns transmit with the radius. the wrist is more useful and stable in flexion than in extension because of the strength of further capsules and ligaments than the interlocking provinces of the skeleton. practically all carpals have six surfaces(except the pisiform). The palmar or anterior surfaces and the dorsal or posterior surfaces are irregular, for ligamentous attachment; the dorsal surfaces live the broader, save in the lunate.
The superior or proximal, and inferior or distal textures are articular, the superior naturally convex, and the inferior concave; the medial and lateral surfaces are again articular where they are in contact with bordering bones, otherwise they are rough and tuberculated.
The structure in all is comparable: cancellous tissue surrounded by a layer of compact bone.
Scaphoid bone
The scaphoid bone is the most prominent carpal bone of the proximal row. the scaphoid bone is a boat-shaped bone (“scaphoid” in Greek tool boat, hence its observation) that lies a little inferior to the anatomical snuffbox. It frames proximally to the radius bone, and distally with the trapezium bone and trapezoid bone. In extra, the scaphoid bone communicates with the lunate bone and capitate bones.
The scaphoid bone has a bony stature located on its palmar surface understood as the scaphoid tubercle; as it seats subcutaneously the tubercle is smoothly palpable on the palm. The scaphoid bone is the numerous continually fractured bone of the wrist. Scaphoid bone fractures mostly arise when a person slips onto the outstretched hand.
Lunate bone
The lunate bone is the next bone of the proximal row, found between the scaphoid bone and the triquetrum bone. The Lunate communicates with the head of the radius (carpal articular cover) and the articular disc of the distal radius.
Triquetrum bone
The triquetrum bone is one of eight carpal bones that includes the area of the wrist joint. It is a pyramidal-shaped bone that can be located on the medial side of the wrist. The name triquetrum bone is emanated from the Latin word triquetrous which means “three-cornered”. It conforms with the lunate bone lateral side and the hamate bone distally. In accumulation, the triquetrum takes an isolated oval-shaped element on its distal palmar surface for presentation with the pisiform bone.
Pisiform bone
The pisiform bone is a small, pea-shaped bone found on the distal palmar surface of the triquetrum bone. It has a dorsal articular part for articulation with the triquetrum bone. the pisiform is a sesamoid bone meaning that it is fully ingrained in a tendon, more specifically in the tendon of the flexor carpi ulnaris muscle. This bone also lies superficially in the palm and it is smoothly palpable.
Trapezium bone
The hand’s trapezium is a carpal bone with a strange shape. The metacarpal bone of the thumb is directly adjacent to the trapezium, which is located within the distal row of carpal bones. The trapezoid and scaphoid bones are located on their lunar surface.[1] 708 The superior surface faces medially and upward; It articulates with the scaphoid and is smooth on the medial side; It is continuous with the lateral surface and rough laterally.
For articulation with the base of the first metacarpal bone, the inferior surface is oval, concave from side to side, and convex from front to back. The thumb’s opposable motion is partially due to this saddle-shaped articulation.
Trapezoid bone
The trapezoid bone is wedge-shaped in the distal line of the wrist carpal bones. It may look extremely small in comparison to the other bones from a palmar region, however, it is much broader on its dorsal side. It creates words with the scaphoid bone proximally, laterally with the trapezium bone, and medially with the capitate bone and its distal facet passes it to articulate with the two metacarpal bones.
Capitate bone
The capitate bone is the biggest of all the carpal bones. It primarily communicates distally with the 3rd metacarpal bone. In extra, it forms articulations with the surrounding carpal bones; with the trapezoid, scaphoid, lunate, and hamate.
Hamate bone
The hamate bone is wedge-shaped and the numerous medial bone of the distal row. The hamate bone formations articulations distally with the fourth and fifth metacarpals, with the capitate laterally and triquetrum proximally.
The hamulus donates to the formation of the medial boundary of the carpal tunnel and the lateral border of the ulnar canal (i.e. Guyon’s canal). The hamulus also functions as the tenderness point for many different ligaments and muscles of the hand and forearm, including the flexor retinaculum.
They are worried about how you’re going to determine all the carpal bones. Examine no further than our interactive carpal bone examinations and labeling activities – they’ll support you in consolidating information fast and effectively.
Function
Ligaments
Four groups of ligaments in the area of the wrist. there are four groups of ligaments in the area of the wrist. the ligaments of the wrist suitably unite the ulna and radius with the carpus: the ulnar and radial collateral ligaments; the palmar and dorsal radiocarpal ligaments; and the palmar ulnocarpal ligament.
The ligaments of the intercarpal articulations unite the carpal bones with one another:
The radiate carpal ligament
The palmar ligaments
The dorsal ligaments
The interosseous intercarpal ligaments
The pisohamate ligament
The ligaments of the carpometacarpal accents unite the carpal bones with the metacarpal bones: the metacarpal ligament and the palmar and dorsal carpometacarpal ligaments. The ligaments of the intermetacarpal articulations unite the metacarpal bones: the dorsal, interosseous, and palmar metacarpal ligaments.
Blood Supply and Lymphatics
The radial artery, ulnar artery, and anastomoses supply the blood supply of the wrist. the radial artery mostly supplies the thumb and the lateral side of the index finger while the ulnar artery supplies the rest of the digits and the medial side of the index finger. In individuals, vascular supply takes location via the anastomotic network consisting of three dorsal and three palmar arcs, which arise from both the radial and ulnar arteries, that overlap the carpal bones.
The scaphoid bone, capitate bone, and a little proportion of lunate bone (20%) all include one intraosseous vessel collection. of not, the scaphoid bone has a single blood collection from the radial artery that joins from the distal part of the bone to deliver the proximal part, thus making its proximal pole most helpless to avascular necrosis. The trapezoid bone and hamate bone both have two provinces of blood collection without intraosseous anastomoses.
The trapezium bone, triquetrum bone, pisiform bone, or most lunate bones (80%) have two regions of blood collection and uniform intraosseous anastomoses. Consequently, the rest of the carpal bones, barring the scaphoid bone, capitate bone, and a small proportion of lunates, maintain a lower danger of growing avascular necrosis following a fracture.
Nerves
Innervation of the wrist joint arrives from the: anterior interosseous branch of the median nerve. posterior interosseous branch of the radial nerve. the dorsal and the profound branches of the ulnar nerve. the lateral antebrachial cutaneous nerve, the posterior interosseous nerve, the dorsal branch and the perforating departments of the ulnar nerve, and the external department of the radial nerve innervate the wrist joint from the dorsum. The palmar cutaneous component of the median nerve, the anterior interosseous nerve, and the major trunk and deep component of the ulnar nerve innervate the wrist joint from the palmar side.
Muscles attachment
Two types of muscles create the muscles of the hand: extrinsic muscles and intrinsic muscles.
Intrinsic muscles grow within the hand itself and likewise contribute to wrist strength by suspending flexor and extensor forces via their tenderness to metacarpal bases. Some carpal bones perform as regions of origin or as sites of insertion for the extrinsic and inherent muscles of the hand. the flexor carpi ulnaris is the most excellent extrinsic muscle that inserts onto carpal bones, particularly the pisiform and hook of the hamate, and the base of the fifth metacarpal bone, which permits it to flexion and adduction of the wrist joint.
All the intrinsic muscles have their origin placed on the carpal bones. the thenar muscles, which have the opponent’s pollicis muscle, abductor pollicis brevis muscle, and flexor pollicis brevis muscle, have origin sites that affect the main tubercles of the scaphoid bone and trapezium bone. The adductor pollicis muscle assumes its origin from the capitate bone and the second metacarpal bone and the third metacarpal bone. The hypothenar muscles such as the opponens digiti minimi muscle, abductor digit minimi muscle, and flexor digiti minimi brevis muscle, originate from the pisiform bone and curve of the hamate bone.
Physiologic Variants
Although unique, the digit of carpal bones may change in the actuality of accessory bones, separated bones, anatomical variants, or genetic abnormalities. Reports exist of over twenty accessory carpal bones, with numerous common variants living in the os centrale carpi, the os radiale external, the triangular bone, and the stylopodium bone.
Various cases of other carpal bones may be interesting split bones of the scaphoid bone, lunate bone, and even the hamate bone. anatomical variants induce extra carpal bones to originate due to a failure of fusion from carpal bone ossification centers. Latest, hereditary anomalies generating fewer carpal bones can seem either due to the hereditary absence of normal bone (which primarily originates with the scaphoid bone, lunate bone, or triquetrum bone) or from an alliance between two carpal bones, which most typically affects the lunate bone and triquetrum bone.
Movements
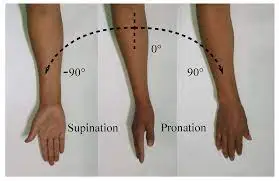
Anatomical terms of motion and Special motions of the hands and feet. the hand is communicated to be in a straightforward position when the third finger heads over the capitate bone and is in a straight line with the forearm. This should not be complicated by the mid-position of the hand which approximates an ulnar variation of 12 degrees. from the straight position two teams of actions of the hand are possible: abduction (movement towards the radius, so-called radial deviation or abduction) of 15 degrees and adduction (motion towards the ulna, so-called ulnar deviation or adduction) of 40 degrees when the arm is in tough supination and barely greater in strict pronation. Flexion and extension are achievable with a complete range of 170 degrees. Radial abduction/ulnar adduction.
Left: Ulnar adduction
Right: Radial abduction
Left: Dorsiflexion
Right: Palmar flexion
During radial abduction, the scaphoid bone is inclined towards the palmar side which permits the trapezium bone and trapezoid bone to close the radius. Because the trapezoid is strictly connected to the second metacarpal bone to which even the flexor carpi radialis muscle and extensor carpi radialis muscle are connected, radial abduction effectively pulls this combined system towards the radius. During radial abduction, the pisiform bone crosses the most significant path of all carpal bones.
Radial abduction is delivered by (in demand of importance) extensor carpi radialis longus muscle, abductor pollicis longus muscle, extensor pollicis longus muscle, flexor carpi radialis muscle, and flexor pollicis longus muscles.
Ulnar adduction forces a tilting or dorsal activity of the proximal row of carpal bones. It is created by the extensor carpi ulnaris muscle, flexor carpi ulnaris muscle, extensor digitorum muscle, and extensor digiti minimi muscle. Both radial abduction and ulnar adduction occurs around a dorsopalmar axis driving via the head of the capitate bone.
Palmar flexion/dorsiflexion
During palmar flexion, the proximal carpal bones are replaced towards the dorsal and palmar sides during dorsiflexion. While flexion and extension consist of activities about a team of transverse axes – giving through the lunate bone for the proximal row and through the capitate bone for the distal column-palmar flexion arises primarily in the radiocarpal joint and dorsiflexion in the midcarpal joint.
Dorsiflexion is produced by (in order of importance) the extensor digitorum muscle, extensor carpi radialis longus muscle, extensor carpi radialis brevis muscle, extensor indicis muscle, extensor pollicis longus muscle, and extensor digiti minimi muscle. Palmar flexion is produced by (in order of importance) flexor digitorum superficialis muscle, flexor digitorum profundus muscle, flexor carpi ulnaris muscle, flexor pollicis longus muscle, flexor carpi radialis muscle, and abductor pollicis longus muscle.
Combined movements
Combined with motions in both the elbow joint and shoulder joints, intermediate or related motions in the wrist are equal to those of a ball-and-socket joint with some required regulations, such as maximum palmar flexion blocking abduction.
Accessory movements
Anteroposterior gliding actions between framing carpal bones or along the midcarpal joint can be achieved by stabilizing particular bones while pushing another (i.e. sponging the bone between the thumb and index finger).
Ossification of the carpal bone starts with the capitate bone and ends with the pisiform bone.
At born, there is no fossilization in the carpal bones. Although there is grand individual variability, approximate ossification words are as follows:
- capitate: 1-3 months
- hamate: 2-4 months
- triquetrum: 2-3 years
- lunate: 2-4 years
- scaphoid: 4-6 years
- trapezium: 4-6 years
- trapezoid: 4-6 years
- pisiform: 8-12 years
Except for the pisiform bone, an opportunity way to remember the proclamation of ossification is to begin at the capitate bone and then drive in an anti-clockwise direction on the volar character of the right carpus bone.
Ossification commands of the distal radius and ulna bones.
Clinical importance
Scaphoid bone fracture
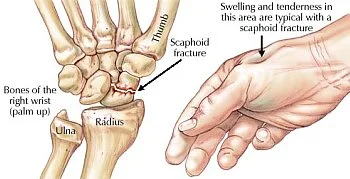
The most typical fracture of the carpus bone is the fracture of the scaphoid bone. It usually appears when someone slips on outstretched writing while trying to control the incident. The symptoms include pain and swelling in the parts understood as the anatomical snuffbox. Difficulties appear due to a lack of blood supply to the location of the palmar carpal component of the radial artery. This inadequacy of blood and attending nutrient deprivation can lead to avascular osteonecrosis.
Carpal tunnel syndrome

Carpal tunnel syndrome is the base term for a condition understood as median nerve reduction and is the numerous standard condition of compression-related neuropathy. It is mostly induced by occupational preferences, such as repeated wrist flexion and extension, directing to overuse of the anatomical structures that directly work during these movements. As a result, an addition in content group and force within the carpal tunnel push down upon the median nerve leading to sensory and motor disorders within its regions of innervation. Chronic contraction can guide to enduring nerve injury and atrophy of the thenar muscles which cracks as weakness in the thumb and index fingers. Therapy includes resting the wrist and refraining from utilizing it for some time. Bandages and splints may support and stabilize the region while anti-inflammatory drugs and painkillers may be prescribed in extreme cases.
Hook of the Hamate Fracture

These fractures are developed by natural crashes usually from “grounding” a golf club or “checking” a baseball bat. They commonly present with hypothenar pain and paresthesias in the distribution of the ulnar nerve. They are analyzed with radiographic imaging and verified with a CT scan if initial x-ray findings are negative. The everyday standard of care remains to excise the hook of the hamate component which has created successful outcomes with a return to sports in 6 weeks.
Lunate Dislocation

Due to the lunate’s proximity to the median nerve, anterior removal of the bone may cause the mechanical reduction of the median nerve within the carpal tunnel and produce signs and symptoms even with median nerve neuropathy such as paresthesias of the foremost three digits and radial half of the fourth digit and deficiency and atrophy of the thenar eminence. Again, the anatomic connection of the carpal bones can also get aggravated by ligament injuries, thereby making two classifications of instabilities, dorsal intercalated segmental instability (DISI) and volar intercalated segmental instability (VISI).
FAQs
The carpal bones are bones in the wrist that connect the bases of the five metacarpal bones in the hand to the distal segments of the radial and ulnar bones in the forearm. Two rows of eight carpal bones are formed: two rows, one proximal and one distal.
Capitate
The Capitate is the biggest carpal bone in the middle of the wrist working as a keystone of the carpal turn. Many wrist ligaments attach to it. It communicates with every other carpal bone excluding the triquetrum. The head of the capitate frames with the deep concave surfaces of the scaphoid bone and lunate bone.
In a helpful wrist, there is a balanced relationship between the proximal rows and distal rows of the carpal bones. The carpal bones can locomote in the flexion/extension plane and the ulnar/radial plane. Comparable actions are complex and are not managed in this module.
The carpal bone is any one of several small, irregular bones that make up the wrist (carpus) in humans and the “knee” of the foreleg in horses, cows, and other quadrupeds. They fit the lower limb’s tarsal bones in the rear.
The ligaments that secure the carpal bones to the radius, ulna, and metacarpals are known as extrinsic wrist ligaments. The carpal bones’ dorsal and palmar surfaces both contain these ligaments. The periosteum, which is the rough outer layer of the bones, is where they attach.
14 Comments