Bone Of The Hand
Table of Contents
Overview
The hand is a remarkable and intricate structure composed of numerous bones that work in harmony to facilitate a wide range of movements and functions. These bones, collectively known as the bones of the hand, form the foundation of our dexterity and fine motor skills.
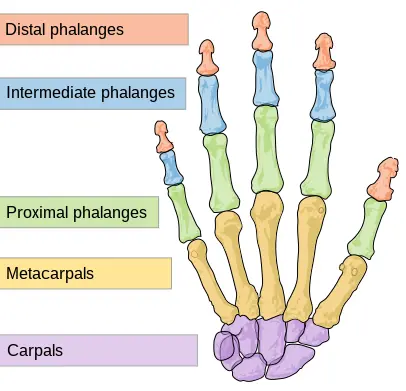
The soft tissues are supported and flexible by the hand bones. They are classified into three types:
Carpal bones (proximal): A group of eight bones with irregular shapes. These are placed near the wrist.
Metacarpals – There are five metacarpals, each of which corresponds to a digit.
Phalanges (Distal) – The finger bones. Except for the thumb, which has two, each finger has three phalanges.
The hand contains several muscles, ligaments, tendons, and sheaths. Muscles are the structures that may contract, allowing the bones of the hand to move. Ligaments are fibrous structures that serve to hold the hand’s joints together. Sheaths are tubular structures that cover a portion of the fingers. Tendons are structures that connect the muscles of the arm or hand to the bone, providing movement.
Furthermore, the hand has arteries, veins, and nerves that supply blood flow and feeling to the hand and fingers.
Anatomy
Wrist
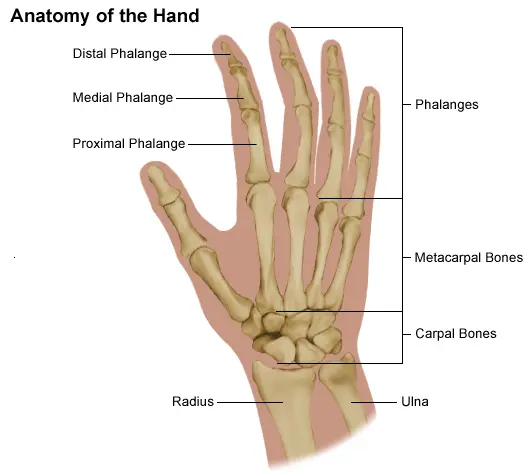
The wrist joint is a complicated joint formed by the Radius and Ulna (two forearm bones) and the carpal bones at their distal ends (furthest from the body). It connects the forearm to the hand and provides a comfortable range of motion. However, repetitive use frequently results in injury.
Bones and Articulation
The Ulna is the largest of the two forearm bones, yet it tapers to become smaller than the Radius at the wrist end. The Radius is located on the thumb side of the wrist, while the Ulna is located on the little finger side. They, along with the carpal bones, constitute the wrist joint. There are eight carpal bones in total, which are placed in two rows, proximal and distal.
- Scaphoid
- Lunate
- Triquetrum
- Pisiform
- Capitate
- Trapezium
- Trapezoid
- Hamate
Because it is the largest carpal bone, the scaphoid bone traverses both rows. The two bones that articulate with the radius and ulna to form the wrist joint are the scaphoid and lunate.
Hand
The human hand is made up of a large palm (metacarpus) with five digits that connect to the forearm via a joint called the wrist (carpus).
Digits
The four fingers on the hand are employed for the most extreme performance; these four digits can be folded over the palm, allowing object grabbing. Each finger, beginning with the one closest to the thumb, has a nickname to differentiate it from the others.
- Index finger, pointer finger, or forefinger
- Middle finger
- Ring finger
- Little finger or ‘pinky’
- Thumb
Bones
The human hand is made up of 27 bones, including eight carpals (wrist bones), five metacarpals (palm bones), and fourteen digital bones (fingers and thumb).
There are five metacarpal bones in the palm, one for each of the five digits. These metacarpals have three parts: a head, a shaft, and a base.
Human hands have fourteen digital bones, also known as phalanges or phalanx bones: two in the thumb (no middle phalanx in the thumb) and three in each of the four fingers. The distal phalanx, which carries the nail, the middle phalanx, and the proximal phalanx are the three.
Sesamoid bones are tiny ossified nodes buried in tendons that give additional leverage and relieve pressure on the underlying tissue. Many exist around the palm at the bases of the digits; the exact number varies depending on the individual.
Articulation
The human hand’s articulation is more sophisticated and delicate than that of analogous organs in any other species. We couldn’t operate a large range of equipment and devices or perform a wide range of hand gestures without this increased articulation.
The articulations are
- Interphalangeal articulations of the hand (the hinge joints between the finger bones)
- Metacarpophalangeal (where the fingers touch the palm) joints
- Intercarpal articulations
- Wrist (sometimes considered to be part of the forearm)
Bones Structure
Carpal Bones
Scaphoid
The scaphoid (“boat-shaped”) bone articulates proximally with the radius to form the carpal tunnel’s radial boundary.
The scaphoid is the largest and most usually fractured bone in the proximal row of carpal bones. It is frequently caused by a fall on an outstretched hand. Fractures can heal slowly as a result of the scaphoid’s inadequate blood supply, and avascular necrosis of the proximal fragment of the scaphoid can ensue.
Lunate
The lunate (“moon-shaped”) bone is a crescent-shaped bone that articulates with the radius proximally. The lunate is located in the middle of the carpal bones, between the scaphoid and the triquetrum. The lunate bone is the most commonly misaligned carpal bone.
Triquetrum
The triquetrum (“three-cornered”) bone is a pyramidal bone. The triquetrum is positioned between the lunate and pisiform bones on the medial side of the proximal row of carpal bones. Triquetrum fractures frequently develop as a result of forceful dorsiflexion of the hand, resulting in an avulsion fracture on the dorsal aspect of the bone.
Pisiform
Pisiform (“pea-shaped”) is a tiny spherical sesamoid bone found in the flexor carpi ulnaris tendon. The pisiform articulates with the anterior surface of the triquetrum bone, causing the bump at the medial base of the hand to extend anteriorly. The ulnar border of the carpal tunnel is formed by the pisiform bone. The pisiform, unlike the other carpal bones, is not engaged in wrist movements.
Trapezium
A trapezium (“table”) bone has four sides. It connects to four bones: the first and second metacarpals, the scaphoid, and the trapezoid. On the palmar surface of the trapezium, there is a prominent tubercle that projects anteriorly.
Trapezoid
The trapezoid (“resembles a table”) bone is a wedge-shaped bone. It got its name from its resemblance to the trapezium. The trapezoid is the smallest of the carpal bones in the distal row. The trapezoid articulates with four bones: the second metacarpal, the trapezium, the capitate, and the scaphoid. The trapezoid is the least usually fractured carpal bone.
Capitate
Capitate (“head-shaped”) is a head-shaped bone. The capitate is the largest carpal bone and articulates with five other bones: the third metacarpal, trapezoid, scaphoid, lunate, and hamate.
Hamate
Hamate (“hooked bone”) is a wedge-shaped bone. It connects to five carpal bones: the fourth and fifth metacarpals, the capitate, and the triquetrum. The hamate is easily distinguished by its form and a hook-like process that extends towards
When a golfer hits the surface forcefully with a golf club on the downswing, the hamate bone is the most commonly fractured. Clinically, this can manifest as pain and symptoms of ulnar nerve injury, as well as numbness and weakness of flexion in the fourth and fifth fingers. The hook of the hamate, like the scaphoid, is subject to avascular necrosis due to its low blood supply.
The Carpal Tunnel
The carpal bones form a U-shaped configuration that faces forward. The flexor retinaculum spans this U-shaped region to keep the carpal bones aligned.
The pisiform and hook of the hamate constitute the medial side of the arch’s base. The scaphoid and trapezium constitute the lateral side of the arch’s base.
The flexor retinaculum connects to the trapezium and scaphoid bones laterally and the hamate and pisiform bones medially. The carpal tunnel is formed by the carpal bones and the flexor retinaculum, with the bones creating the wall and floor and the tendon forming the roof.
Carpal tunnel syndrome is caused by flexor retinaculum thickening, which causes discomfort due to median nerve compression.
Metacarpal bones
Each palm has five metacarpal bones that articulate with one of the distal carpal bones to produce a carpometacarpal joint. The metacarpals’ distal ends engage with the phalanges to produce the metacarpophalangeal joint.
Each metacarpal is associated with a finger and is numbered 1-5, starting with the thumb. Each metacarpal contains three parts: a head, a body, and a base.
The first metacarpal bone is distinct from the other metacarpal bones that comprise the hand’s base. This allows the first metacarpal bone to move freely, irrespective of the other metacarpal bones.
Because metacarpals 2-5 are articulated closely together, metacarpal fractures tend to be stable; nevertheless, instability can arise if numerous metacarpal fractures occur (e.g., in a severe crush trauma). A boxer’s fracture is most commonly found in the neck of the fourth and fifth metacarpals, which occurs when a person strikes an item with a closed hand.
Phalanges
The bones of the fingers and thumbs are made up of 14 phalanges. The Pollux (thumb), like the hallux, has only two phalanges (proximal and distal), but the remaining fingers have three (proximal, middle, and distal).
Each phalanx, like the metacarpals, has a base, body, and distal head. Each phalanx’s base articulates with the metacarpal’s head.
Crushing injuries to the phalanges are the most prevalent type of injury, such as closing a door on the digit.
Clinical Relevance
Scaphoid Fracture
The most usually fractured carpal bone is the scaphoid bone of the hand, which is caused by falling on an outstretched hand (FOOSH).
Pain and tenderness in the anatomical snuffbox are the hallmark clinical features of a scaphoid fracture.
Because of the retrograde blood supply’ that arrives at its distal end, the scaphoid is especially vulnerable to avascular necrosis after fracture. This means that a fracture to the scaphoid’s midpoint (or ‘waist’) may cut off blood supply to the proximal part of the bone, rendering it avascular.
Patients who have a missed scaphoid fracture are more prone to develop wrist osteoarthritis later in life.
Fractures of the Metacarpals
The metacarpals are commonly fractured in two ways:
Boxer’s fracture is a 5th metacarpal neck fracture. It is typically produced by a clinched fist colliding with a hard object. The distal component of the fracture is moved anteriorly, causing the affected finger to shorten.
Bennett’s fracture is a fracture of the first metacarpal base induced by forced thumb hyperabduction. This fracture spreads into the first carpometacarpal joint, causing instability and joint subluxation. As a result, it frequently necessitates surgical repair.
Small Joint Osteoarthritis
This condition shows Heberden and Bouchard nodes of the DIP and PIP, respectively (mnemonic: B comes before H). These nodes are the cutaneous symptoms of osteoarthritic joint space narrowing and osteophyte development. According to research, there is a link between the appearance of these nodes and the underlying osteoarthritis.
The disease’s structural progression.
Rheumatoid Arthritis (RA)
Rheumatoid Arthritis (RA) is a kind of arthritis that frequently manifests as noticeable hand symptoms. Swan neck and boutonniere abnormalities, as well as ulnar deviation of the digits, are typically characterized. The swan neck deformity is defined by DIP flexion with PIP extension, whereas the boutonniere deformity is the inverse. illness-modifying antirheumatic medications (DMARDs) have lowered the severity of RA hand illness, but early intervention should be initiated to prevent disability and progressive joint degradation found in the disease’s natural course.
Ape Hand
Ape Hand is distinguished by thenar eminence wasting. This is due to a loss of the median nerve, as in carpal tunnel syndrome, or a rather superficial cut on the medial aspect of the thenar eminence halfway point. The abductor pollicis brevis, superficial head of the flexor pollicis brevis, and opponens pollicis are all denervated by a lesion of the recurrent branch of the median nerve.
If the median nerve in the hand is completely denervated, the first and second lumbrical will be damaged as well. Because of the action of the lengthy extensors on the hand, the hand appears to lack an opposable thumb (as in apes). The patient cannot oppose the thumb. Although thumb flexion is decreased, the flexor pollicis longus is intact and far more powerful than the flexor pollicis brevis. The deep branch of the ulnar nerve also innervates the deep head of the flexor pollicis brevis. Abduction occurs because the abductor pollicis longus (posterior interosseous nerve from the radial nerve) is intact.
Bishop Hand (Hand of Benediction or Preacher Hand)
Bishop Hand (Hand of Benediction or Preacher Hand) is a condition caused by a median nerve palsy. The ring and little fingers flex as the patient tries to make a first, but the index and fingers remain extended. This is because all of the flexor digitorum superficialis and flexor digitorum profundus muscle slips for the index and ring fingers have been denervated.
The loss of the first and second lumbricals also contributes to the index and middle fingers straightening (extension). Flexion of the ring and little fingers is weaker due to the loss of the flexor digitorum superficialis to these fingers, but the muscle slips from the flexor digitorum profundus to these fingers, as well as the third and fourth lumbrical, are still intact. It should be emphasized that the patient must make a fist for the index and middle finger extensions to remain extended.
Boutonniere Deformity
Boutonniere Deformity affects the MCP (metacarpophalangeal) and DIP (distal interphalangeal) joints. Damage to the central section of the extensor hood causes flexion of the proximal interphalangeal joints. Rheumatoid arthritis is the most common cause of the boutonnière deformity. The phrase boutonnière refers to a flower placed in a buttonhole during a ceremony such as a wedding.
Nail Disorders
Beau lines are transverse ridges or lines created by a halt in nail development induced by nutritional deficient situations. Beau lines can be caused by a variety of reasons. Clubbed nails can be caused by respiratory conditions like obstructive pulmonary disease or severe emphysema, as well as cardiac diseases such as congenital cardiac abnormalities and cor pulmonale. Mees lines appear as white transverse lines. Arsenic and thallium poisoning, as well as high fevers, can cause them. Spoon-shaped nails feature a scooped depression that can be caused by a variety of factors such as anemia (particularly iron deficiency anemia), fungal infection, long-term diabetes, psoriasis, and genetic anomalies.
Palmar Arch Arterial Bleeding
Palmar Arch Arterial Bleeding: Palmar arterial arches lesions can cause uncontrollable bleeding. Compressing the brachial artery onto the humerus is the best approach to stop the bleeding.
Polydactyly
Polydactyly is a very common anatomical abnormality that occurs once per 700 to 1000 live births. There are several kinds of polydactyly, which can be classified as syndromic or non-syndromic. Polydactyly is classified into subtypes based on the origin of the additional digit. Though the specific genetic relationships are yet unknown, patients who come with polydactyly should undergo a thorough workup to rule out any underlying disorders.
Trigger Finger
Trigger Finger is caused by thickening of the finger tendon sheath. When the finger is flexed, the thickness causes it to stick. The thickening is caused by sheath inflammation. When the finger is flexed, it sticks and eventually snaps free. Females are more likely than males to get this illness. Rheumatoid arthritis is the most common cause of this malformation.
Ulnar Drift of the Hand
Ulnar Drift of the Hand: This is particularly frequent in rheumatoid arthritis. The hand deviates to the ulnar side at the metacarpophalangeal (MCP) joints due to the bowing of the extensor digitorum ligaments.
Ulnar Claw Hand (Claw Hand)
Ulnar Claw Hand (Claw Hand): This is caused by an ulnar nerve lesion. The MCP joints for the ring and little fingers are hyperextended due to the loss of the third and fourth lumbrical muscles due to a lesion of the ulnar nerve’s deep branch. The dorsal and ventral interossei are missing, but the ring and middle fingers are not clawed because the first and second lumbrical, which are innervated by the median nerve, are intact.
The capacity to oppose the little finger and adduct the thumb will be lost as a result of the ulnar nerve deep branch damage. If the lesion occurs higher in the forearm (medial epicondylar fracture), the radial deviation will ensue due to flexor carpi ulnaris loss. Because of the loss of the flexor digitorum profundus to these digits, the flexion strength of the ring and little fingers is reduced. Sensory function loss will develop in the medial half of the ring finger and all of the little fingers.
Due to a lesion of the dorsal cutaneous branch of the ulnar nerve, sensation to the medial side of the dorsum of the hand will be lost. Because the medial cutaneous nerve of the forearm is generated from the medial chord of the brachial plexus, the medial forearm will not be affected.
Wrist Drop Deformity
Wrist Drop Deformity: This is caused by a radial nerve lesion. Because the wrist and finger extensors are denervated, the digits are unable to be extended. The examiner holds the forearm in a steady horizontal posture during the wrist drop test. The therapist holds the patient’s hand. The patient tries to extend his or her hand but is met with resistance. The outcomes are compared to the other hand.
Wrist drop is caused by some differences in the lesion. The lesion in the first case is a mid-humeral or supracondylar radial fracture. The branches to the brachioradialis and extensor carpi radialis longus are the first to emerge and are significantly smaller in size than the radial nerve itself. As a result, they may be saved, even if the rest of the nerve is lost. The extensor carpi radialis longus causes feeble extension and radial deviation of the hand when the hand is flexed (“dropped”).
Wrist drop is also evident in lesions of the posterior interosseous nerve, which develops from the deep branch of the radial nerve as it emerges from behind the Frohse arcade. When a patient with posterior interosseus neuropathy is examined for “drop hand,” the extensor carpi radialis brevis and extensor carpi radialis longus are intact, resulting in weak extension of The radial aspect of the hand with radial deviation.
Sensory changes of the radial neuropathy
The following are the sensory changes associated with radial neuropathy. The posterior cutaneous nerve of the forearm is derived from the proximal radial nerve and is only involved in proximal radial neuropathies. The superficial (sensory) radial nerve emerges on the radial side of the hand, while the deep (motor) branch divides the radial nerve in the antecubital fossa. The dorsum of the hand on the radial side is supplied by the superficial (sensory) branch. The dorsum of the thenar web can be evaluated for sensation. Branches provide the digits to varying degrees. The index and middle fingers may be affected by phalangeal base involvement. The median nerve (index, ring, and lateral half of the fingers) is the only nerve that supplies the tips of the fingers.
Zigzag Thumb Deformity
The thumb is flexed at the carpometacarpal joint (CMJ) and extended at the metacarpophalangeal joint (CMJ) in a zigzag pattern. This deformity is typical of rheumatoid arthritis. Other occurrences could be the result of hereditary hypermobility.
Summary
The bones of the hand are divided into three groups: carpal bones, metacarpal bones, and phalanges bones.
- Carpal bones: The carpal bones are the eight bones that make up the wrist. They are arranged in two rows, with four bones in each row. The carpal bones are connected by ligaments, and they also articulate with the radius and ulna bones of the forearm.
- Metacarpal bones: The metacarpal bones are the five bones that form the palm. They are numbered from 1 to 5, with the thumb having metacarpal bone 1. The metacarpal bones articulate with the carpal bones proximally and the phalanges bones distally.
- Phalanges bones: The phalanges bones are the 14 bones that form the fingers and thumb. Each finger has three phalanges bones, while the thumb has two. The phalanges bones are numbered from 1 to 3, with the distal phalanx being the closest to the fingertip.
The bones of the hand work together to allow for a wide range of movements, including grasping, pinching, and manipulating objects. They also provide support and stability for the hand and wrist.
Here are some functions of the bones of the hand:
- Support and stability: The bones of the hand provide support and stability for the hand and wrist. This allows us to perform a variety of tasks, such as carrying objects and gripping tools.
- Movement: The bones of the hand also allow us to move our fingers and thumb. This is essential for many activities of daily living, such as writing, eating, and dressing.
- Protection: The bones of the hand help to protect the soft tissues of the hand and wrist from injury. This is important because the hand is a vulnerable area that is often exposed to harm.
FAQs
What are the functions of the bones in the hand?
The bones in the hand provide support and stability for the hand and wrist.
They also allow us to move our fingers and thumb, which is essential for many activities of daily living.
The bones in the hand also help to protect the soft tissues of the hand and wrist from injury.
What are the most common injuries to the bones in the hand?
The most common injuries to the bones in the hand are fractures and dislocations.
Fractures can occur in any of the bones in the hand, but they are most common in the metacarpal and phalanges bones.
Dislocations are most common in the fingers and thumb.
How are injuries of the bones in the hand treated?
The treatment for injuries to the bones in the hand will vary depending on the type and severity of the injury.
Minor injuries, such as sprains and strains, may be treated with rest, ice, compression, and elevation (RICE).
More serious injuries, such as fractures and dislocations, may require surgery
What are the risk factors for developing bone diseases in the hand?
The risk factors for developing bone diseases in the hand include: Age
Family history of bone disease
Certain medical conditions, such as Osteoarthritis
Certain medications, such as corticosteroids
Smoking
Excessive alcohol consumption
How can I maintain my bones strong and healthy?
To keep your bones healthy and strong, you should: Eat a healthy diet that is rich in calcium and vitamin D
Exercise regularly
Maintain a healthy weight
Avoid smoking and excessive alcohol consumption
References
- Arias, D. G. (2023, July 30). Anatomy, Shoulder and Upper Limb, Hand Bones. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK547684/#:~:text=The%20carpus%20(proximal%20and%20distal,four%20consistently%20present%20sesamoid%20bones.
- Bones of the Hand – Carpals – Metacarpals – Phalanges – TeachMeAnatomy. (2020, August 16). TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/bones/bones-of-the-hand-carpals-metacarpals-and-phalanges/
- Tang, A. (2022, November 28). Anatomy, Shoulder and Upper Limb, Hand Carpal Bones. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK535382/
- Anatomy: Hand and Wrist – BID Needham. (n.d.). https://www.bidneedham.org/departments/orthopaedics/hand-program/anatomy-hand-and-wrist
- Ross, C. (2022, February 22). Bones of the Hand | Carpal Bones – Metacarpal bones | Geeky Medics. Geeky Medics. https://geekymedics.com/bones-of-the-hand/