
Hand Bones
Table of Contents
Introduction
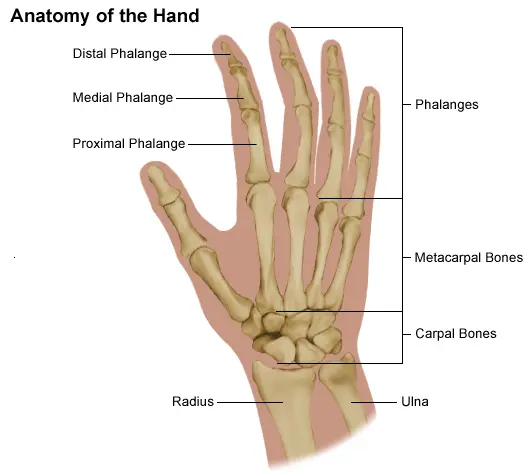
The hand is made up of a lot of different bones, muscles, and ligaments, which give it a lot of flexibility and movement. There are three significant arrangements of bones in the actual hand, including:
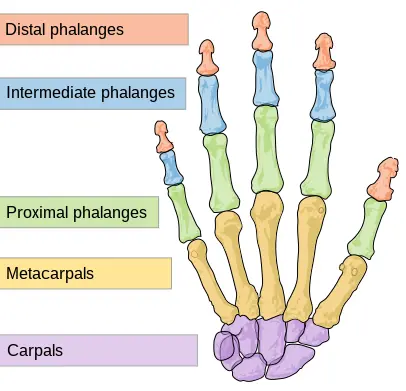
Phalanges. The 14 bones are situated in the fingers of a singular hand and the toes of per foot. Independently finger holds 3 phalanges (the distal, center, and proximal); Only two are on the thumb.
Metacarpal bones. The 5 bones that organize the middle part of the hand.
Carpal bones. The 8 bones that form the wrist. The two rows of carpal bones are attached to 2 bones of the arm-the ulna bone and the radius bone.
The hand can contain several muscles, ligaments, tendons, and sheaths. The structures that can charter and enable the hand’s bones to move are the muscles. The pointer’s joints are held together by ligaments, which are fibrous tissues. The sheaths are cylindrical designs that cover a district of the fingers. The ligaments associate muscles in the part or hand deep down to permit development. In addition, the hand contains arteries, veins, and nerves that supply the hand and fingers with blood flow and sensation.
Structure and Function
The carpus (proximal and distal rows), metacarpal bones, phalanges, and different sesamoid bones contain the skeletal hand. There are 5 metacarpals, 14 phalanges, and four always-present sesamoid bones in the hand.
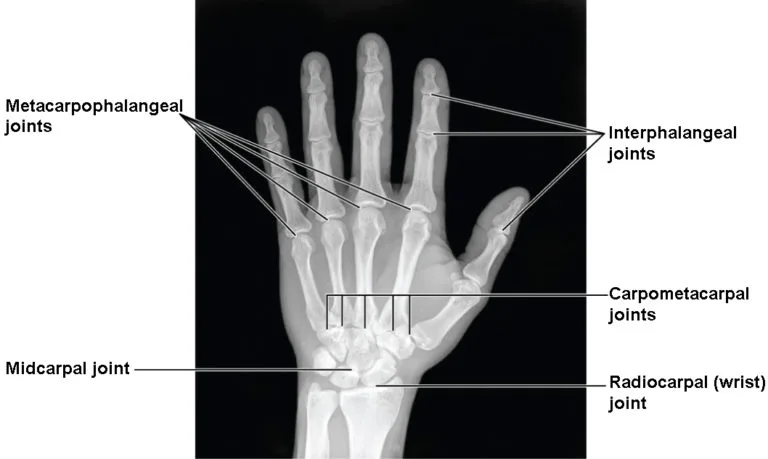
The wrist attaches to the hand at the carpometacarpal (CMC) joints. The first CMC structures form the expression between the trapezium and the base of the first metacarpal. The base of the second metacarpal connected with trapezium, trapezoid, and capitate. The base of the third metacarpal communicates with the capitate. The base of the fourth metacarpal communicates with the capitate and hamate. The fifth metacarpal’s base communicates with the hamate.
The first metacarpal bone resembles the thumb, the second to the index finger, the third to the long finger, the fourth to the ring finger, and the fifth to the little finger. The thumb has 2 phalanges, named proximal and distal phalanges. The proximal phalanx base contains the metacarpophalangeal (MCP) joint with the first metacarpal head. The head of the proximal phalanx frames with the base of the distal phalanx to form the interphalangeal (IP) joint. The index, long, ring, and small fingers individually have proximal, middle, and distal phalanges. The proximal phalanges include MCP joints with separate metacarpal bones. The head of an individually proximal phalanx articulates with the base of each middle phalanx to include proximal interphalangeal (PIP) joints. The head of each middle phalanx articulates with the base of each distal phalanx to comprise distal interphalangeal (DIP) joints. two sesamoid bones are current at the first MCP joint. These are forever present and have important functional implications for the movement of the thumb. Single sesamoids occur over the second and fifth MCP joints in 60.8% and 59.1% of people, respectively.
Embryology
The limb bud first occurs in the proximal fetus around the fifth week of development. From this point, different HOX genes control the growth of the limb. The stylopod, zeugopod, and autopod stand as the three development zones of the limb bud conforming to the humerus, ulna, radius, and hand, respectively. Ectoderm differentiates into the apical ectodermal ridge, nonridge ectoderm, and location of polarizing action. These zones carry essential roles in differentiation. For example, the reduction of the apical ectodermal ridge early in limb growth will result in the actuality of only stylopod development. Reduction of the apical ectodermal mound later in development will result in the development of the stylopod and zeugopod, but no autopod, leading to the fetus not growing a hand.
In humans, the hand embryologic result is the result of the HOXA and HOXD genes. Anteroposterior development is governed by HOXA, while proximodistal growth is governed by HOXD. Analyses have shown that the length of the metacarpal bone can help figure out how the fetus will develop before birth, which could help find any anomalies. A more complete picture can be obtained by combining this with foot lengths and other commonly used growth estimates. During development, a wide range of morphologic abnormalities may occur because of the involved structure of the hand.
Blood Supply and Lymphatics
Blood supply to the hand comes from the ulnar and radial arteries, which are branches of the brachial artery. Dorsal hand vascular collection comes from the dorsal carpal angle. This arch forms from anastomosis of the dorsal carpal branches of radial and ulnar arteries. Metacarpal departments subsequently appear from the dorsal carpal arch. The first metacarpal department systems along the radial border of the second metacarpal, supplying the first web area and second metacarpal. The second via fifth branches route along the ulnar boundaries of the second via fifth metacarpals and provide branches to the interosseous muscles as well as the periosteum.
The superficial palmar arterial angle is primarily created by the ulnar artery, while the radial artery primarily supplies the deep palmar arterial arch. Metacarpal components generally arise from the deep arch, while digital arteries arise from the superficial arch. Metacarpal branches form anastomosis with digital arteries. Physiologic take of arterial flow in the hand is aching with a group of anastomoses and variations in flow dominance.
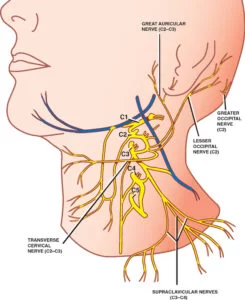
Nerves
Innervation to the hand is from the median, ulnar, or radial nerves. Separately number/ray has two palmar and two dorsal digital nerves. The cutaneous volar component of the first three and a half digits is innervated by the median nerve.
The ulnar nerve completely innervates the dorsal and volar ulnar half of the fourth and fifth numbers. The radial nerve innervates the remainder of the dorsal hand. Due to the complicated function of the hand, it is vital that clinicians reliably report and understand proprioception and gripping strength. A multiple innervation distribution is supplied to the MCPs, PIPs, and DIPs to facilitate this knowledge.
Muscles
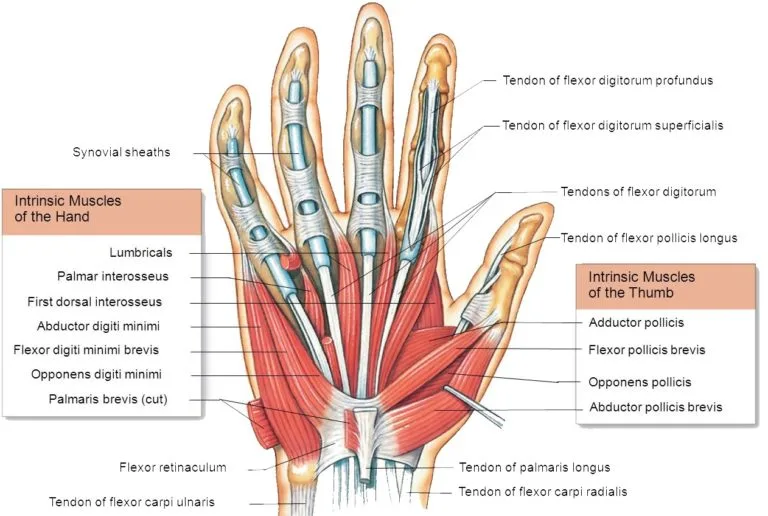
Three volar Interossei adduct the two, fourth, and fifth digits around an axis created by the third digit. These muscles originate on the metacarpal of the number living adducted and insert into their proximal phalangeal floor and extensor hood. Adduction occurring along this third number axis suggests that the volar interosseous muscle of the second digit is found on its ulnar border, while the interossei of the fourth and fifth digits live on their radial boundaries.
Four dorsal interossei function to pinch the second, third, and fourth digits while helping with the flexion of the MCPs, the affection of the PIPs, and the branch of the Drops. The first dorsal interosseous muscle arises from the first and second metacarpals, inserting into the radial ground of the proximal phalanx of the second digit as well as its extensor hood. The second dorsal interosseous muscle originates from the second and third metacarpals, inserting into the radial base of the proximal phalanx of the third number as well as its extensor hood. The third dorsal interosseous muscle derives from the third and fourth metacarpals, inserting into the ulnar base of the proximal phalanx of the third digit as well as its extensor hood. The fourth dorsal interosseous muscle arises from the fourth and fifth metacarpals, inserting into the ulnar base of the proximal phalanx of the fourth number as well as its extensor hood.
Abductor pollicis longus (APL) structures in the lower arm, at the midshaft of the spiral limit of the ulna, and the ulnar boundary of the sweep, as pleasantly as the interosseous layer. It supplements the outspread side of the foundation of the principal metacarpal in supplement to the trapezium and opponens pollicis belt. This strength acts to snatch the principal digit.
Abductor pollicis brevis (APB) creates at the trapezium and scaphoid and inserted into the lateral base of the proximal phalanx of the first digit. This force acts in first-digit abduction in addition to MCP flexion.
Distal to the origin of APL, the extensor pollicis longus (EPL) develops at the radial border of the ulna and the interosseous membrane. EPL supplements the ground of the distal phalanx and acts to broaden the interphalangeal joint.
Extensor pollicis brevis (EPB) originates at the ulnar boundary of the radius and interosseous membrane at the level of EPL. It inserts to the floor of the proximal phalanx of the first number and aids in the first digit extension at the MCP.
Opponens pollicis parts to pronate the first metacarpal. It starts at the trapezium and inserts into the anterolateral aspect of the first metacarpal.
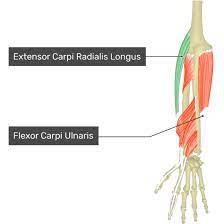
The flexor carpi radialis (FCR) inserts into the trapezium, two metacarpals, and the third metacarpal at the medial humeral epicondyle. The wrist is flexed and radially countered by FCR.
Flexor pollicis brevis (FPB) has a profound and superficial head. The deep head begins at the second metacarpal, while the superficial head creates at the transverse carpal ligament and trapezium. These insert into the lateral side of the proximal phalanx of the first digit and function to flex the MCP.
Flexor pollicis longus (FPL) is the immediate flexor of the first digit, originating from the volar interosseous membrane and radius. It inserts into the floor of the distal phalanx.
The Adductor pollicis has 2 heads, an oblique and second transverse. The oblique head originates at the capitate, and the second, and third metacarpals. The transverse head creates at the distal half of the third metacarpal shaft. These both insert into the medial floor of the thumb proximal phalanx and act to adduct the first digit.
Abductor digiti minimi (ADM) acts to abduct the fifth digit and has existed located to originate at the pisiform, piso-hamate ligament, and flexor carpi ulnaris. It inserts into the ulnar factor of the proximal phalangeal base and extensor apparatus of the fifth digit.
Flexor digiti minimi (FDM) develops from the hamate, pisiform, and flexor retinaculum. Distally, it connects with ADM to insert into the proximal phalangeal base of the fifth digit, directing to its action of MCP flexion.
Extensor carpi ulnaris originates at the lateral humeral epicondyle and inserts into the dorsal base of the fifth metacarpal, acting in wrist extension and ulnar deviation.
Flexor digitorum superficialis (FDS) has an expansive origination from the medial epicondyle of the humerus and coronoid process of the ulna to the volar part of the radial shaft. It then inserts into the middle phalangeal bases of the second via fifth digits. This acts primarily in PIP flexion.
Flexor digitorum profundus (FDP) originates from the volar-medial aspect of the ulna and interosseous membrane and inserts at the distal phalangeal bases of the second through fifth digits. This performs DIP flexion.
The central label and terminal tendons of the humerus, known as the extensor digitorum communis, originate at the lateral epicondyle and insert at the dorsal portion of the distal phalangeal base of the second via fifth numbers. The accessory slips and insertions of this muscle vary significantly anatomically, but the standard instruction states that in addition to the always-present terminal insertion, there is also an insertion into the middle phalanx and MCP.
Physiologic Variants
There is a fantastic deal of physiologic divergence between people in the morphology of the hand bones. One of the tools used to differentiate the variance in hand anatomy is the digit length ratio of the two to the fourth digit, otherwise referred to as the 2D to 4D ratio. This number has been indicated to be 0.98 among the general people but shows variability between ethnicities, ethnicities, and sexes, as well as the handedness of the patient. The third digit is always the longest of the digits. The most significant source of friction in the hand bones is the impact of contrasts in size.
Surgical Considerations
Metacarpal fractures should experience fixation if there is any segment of malrotation to ensure that patients can create a closed fist and hold it properly.
Surgery is indicated in the treatment of these fractures when the fracture pattern falls outside of proper angulation patience, and therefore the patient’s functional outcome would profit from surgical fixation by lag pin fixation and/or plating processes, or via percutaneous pinning of the fractures. Patience for fractures of the shaft and neck of each metacarpal varies with the index tolerating the minor angulation and the little finger tolerating the most. Fractures of the fifth metacarpal neck, otherwise understood as boxer’s fractures highlight the good outcomes of nonoperative treatment of the maturity of these fractures.
include MCP or IP dislocations that are basic and will also need to experience surgical fixation to facilitate the rehabilitation of function. Phalanx fractures with removal, nonunion, malunion, ipsilateral extremity fractures, pathologic fractures, or multiple inconsistent ipsilateral hand fractures may demand surgical intervention. Dorsal intraarticular fractures of the distal phalanx, otherwise comprehended as mallet finger, rarely need to experience surgical fixation, but intervention is indicated with greater than 30 percent involvement of the articular character or for volar subluxation of the distal phalanx. Volar interarticular avulsion fractures of the distal phalanx, also understood as jersey finger, by in large require surgical fixation for the rehabilitation of flexor digitorum profundus function.
Clinical importance
Polydactyly occurs onetime in every 700 to 1000 live births, creating a relatively standard anatomical variant. There is a type of types of polydactyly, and they can broadly classify as syndromic or non-syndromic. Subtypes of polydactyly live based on the point of origination of the extra digit. Though the exactness of the exact inborn links is always a work in improvement, patients who present with polydactyly should have a mindful workup to head out underlying conditions.
Small joint osteoarthritis characteristically suggests Heberden and Bouchard nodes of the DIP and PIP, respectively. These nodes determine the cutaneous indications of joint space narrowing and osteophyte appearance resulting from osteoarthritis. Analysis shows a positive correlation between the formation of these nodes and underlying osteoarthritis.
Rheumatoid arthritis (RA) is another format of arthritis that often suggests prominent hand manifestations. Swan channel and boutonniere deformations are classically defined, in complement to the ulnar deviation of the numerals. The swan neck deformation is characterized by DIP flexion with PIP extension, while the inverse is right of the boutonniere deformity. Nowadays, disease-modifying antirheumatic drugs (DMARDs) have been able to decrease the rigor of hand disease seen in RA, but early intervention should be started to control disability and progressive joint deterioration seen in the natural course of the disease.
FAQs
Our hands do so much for us. They are capable of a wide multiplicity of functions: touching, grasping, feeling, holding, manipulating, caressing, and more They are a vitally important component of who we are and how we see ourselves.
27 joints
The hand’s anatomy has 27 bones, 27 joints, 34 muscles, over 100 ligaments and tendons, numerous blood vessels, nerves, and related soft tissue. It is significant to understand the standard anatomy of the hand to understand diseases and conditions that can impact our hands.
Each of the fingers has three joints:
metacarpophalangeal joint (MCP) – the joint at the floor of the finger.
proximal interphalangeal joint (PIP) – the joint in the middle part of the finger.
distal interphalangeal joint (DIP) – the joint nearest to the fingertip.
Definition
index finger, pointer finger, or forefinger.
the middle finger or long finger,
ring finger.
little finger, pinky finger, or small finger.
The short, thick first number of the human hand and the lower-primate hand and foot, also known as the pollex. It has only two phalanges, which are the tubular bones of the fingers and toes, unlike other digits. The thumb even contrasts in having a lot of opportunity for movement and standing opposable to the tips of different digits.
One Comment