
Scheuermann’s Disease
Table of Contents
What is Scheuermann’s disease?
A radiologist from danish first discovered Scheuermann’s in the early nineties, & the condition is named after him. Scheuermann kyphosis, also known as Scheuermann disease, juvenile kyphosis, or juvenile discogenic disease, is a disease involving an abnormal, excessive curvature of the spine. It affects bodies & discs of the vertebra of the spine & is turned into anterior wedging of more than or equal to 5 degrees in 3 or more adjacent vertebral bodies.
Scheuermann’s disease is a childhood self-limiting skeletal disease. In which the vertebral body grows unevenly that is, the posterior angle is frequently more than the front.
Mostly, evaluation is made at the age of 12 to 17 years when parents observe the hunch back or change in posture.
Pain in the involved hyperkyphotic region can also be the finding of the initial evaluation. Scheuermann’s disease is the most usual cause of kyphotic deformity in adolescents.
Scheuermann disease is categorized into two types, Type 1 only includes the thoracic spine, whereas type 2 involves both the lumbar spine & thoracic spine. Scheuermann disease typically presents with postural deformity & subacute thoracic pain in adolescents.
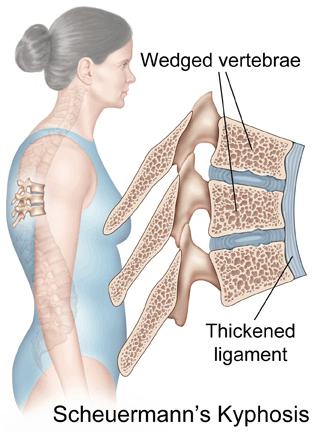
Scheuermann’s kyphosis develops over time during phases of bone growth (such as puberty). It occurs when the front part of the body of the spine doesn’t grow as rapidly as the back of the spine & causes healthy, rectangular-shaped vertebrae to become triangular-shaped & wedged together. This causes the thoracic spine to curve greater than normal. Patients become forward stooped with a bent-over posture.
The Normal Spine
To better understand kyphosis first, we need to know basic anatomy lessons. The spinal column (also called the vertebral column) starts at the skull & extends into the pelvis. The column has thirty-three vertebrae with discs in between each vertebra which helps to absorb shock & distribute load and keep the vertebrae from grinding each other during movement. Healthy vertebrae are shaped rectangular & stacked one on top of another.
anatomy lateral (side) spine
the spine is normally curved from front to back. For some patients, nevertheless, the thoracic spine curves too much (more than 40-45 degrees), giving them a hump appearance on their backs. Sometimes their heads seem like they are sloped forward as though resting on their chests. This is called kyphosis.
Diagnosis can be made with an x-ray of the standard & hyperextension lateral side of the thoracic spine.
non-steroidal anti-inflammatories, stretching exercises, and lifestyle modification can include in management. However, a brace is prescribed for more extensive conditions, & surgical treatment option is for patients with a greater degree of kyphosis, neurologic deficits, or severe refractory pain. This activity outlines the diagnosis & management of kyphosis and defines the role of the individual in the healthcare professional team for improving care for patients with this disease.
What are the causes of Scheuermann’s disease?
The definitive and universally accepted causes of Scheuermann kyphosis remain undetermined. As previously mentioned, a hereditary component is understood to contribute to this disease’s development, although the mode of transmission is still unclear. Height & weight might also be contributing factors.
The small bones- vertebrae that make up the spine are generally rectangular. They bundle like bricks with flexible cartilage in between. When a child has kyphosis, the posterior part of some of the vertebrae grows rapidly compared to the anterior part. These vertebrae become wedge-shaped, so when the vertebrae bundle up, the spine curves, making the back round out.
One growing theory, supported by histologic evaluations, advocates discordant vertebral endplate mineralization & ossification during growth which causes disproportional vertebral body growth & resultant classic wedge-shaped vertebral bodies that lead to kyphosis.
Pathoanatomy
- the exact pathophysiology is unknown but several theories
- osteonecrosis of the anterior apophyseal ring
- herniation of disc content leading to loss of anterior disc height
- relative osteoporosis leading to compression deformity
- altered biomechanics leading to anterior wedging & subsequent growth arrest
- most widely accepted theory suggests that kyphosis & vertebral wedging are caused by a developmental error in collagen aggregation which outcomes in an abnormal end plate
Genetics
- the autosomal dominant inheritance pattern is now accepted
Other theories proposed include mechanical, metabolic, & endocrinologic causes, but the real cause is still unclear.
What are the symptoms of Scheuermann’s disease?
Scheuermann’s disease is considered to be a type of juvenile osteochondrosis of the spine. It’s found mostly in teenagers & presents a typically worse deformity than postural kyphosis. Patients suffering from Scheuermann’s kyphosis consciously can not correct their posture. The apex of their curve, situated in the thoracic vertebrae, is quite rigid.
Scheuermann’s condition is ignominious for causing mid & lower back & neck pain, which can be severe and disabling. The inpatient might feel pain at the apex of the wind, which is exacerbated by physical exertion & by ages of standing or sitting; this can have a significantly mischievous effect on their lives as their position of exertion is checked by their disability. The case might feel isolated or uncomfortable amongst their peers if they’re children, depending on the position of disfigurement.
In addition to the pain associated with Scheuermann’s complaint, numerous cases with the complaint have a loss of vertebral height & depending on where the apex of the wind is, might have a visual hunchback’ or’ round back’. It has been reported that angles in the lower thoracic area beget more pain, whereas angles in the upper area present further visual disfigurement. nonetheless, it’s general pain or ornamental reasons that prompt cases to seek help for their condition. In studies, kyphosis is better characterized for the thoracic chine compared to the lumbar chine
The seventh & tenth thoracic vertebrae are most commonly involved. It causes backache & spinal curvature. In very serious cases it might cause internal problems and spinal cord damage, but these cases are extremely rare. The curve of the reverse reduces height, therefore putting pressure on internal organs, wearing them out more snappily than the natural aging process; surgical ways are nearly always recommended in this case.
Pain Scheuermann’s cases had an advanced threat for reverse pain & disabilities during conditioning of diurnal living than controls. however, the degree of thoracic kyphosis among patients wasn’t related to reverse pain, general health, or quality of life.
- Possible Subacute thoracic pain, generally no identifiable inciting event. The pain is worse during activity & improved with rest.
- The disfigurement is generally appreciated in the early to mid-teenage times by the child, parents, or on an academy webbing test.
- The physical test shows a rigid hyperkyphotic wind, accentuated with forward bending and condescending.
- Hyperkyphosis doesn’t resolve with an extension or lying prone or supine, further supporting the “ rigid ” nature of this disfigurement.
- Other associated findings on an examination might include cervical or lumbar hyperlordosis, scoliosis, & tight hamstrings.
- Although neurologic deficits aren’t common, a thorough neurologic exam must be taken.
- Muscle tightness & fatigue, especially at the end of the day.
- Reduced flexibility of the torso
- In severe cases, heart & lung function can be impaired, or severe neurological symptoms can occur. These symptoms are extremely rare.
Patients with Scheuermann’s disease are unable to participate in physical exercise, work, & activities of diurnal living secondary to pain or the presence of their deformity negatively affecting their ornamental appearance. Possible to see cutaneous skin saturation at the region of the topmost curve due to skin disunion on president tails. The history of kyphosis is not clear, with controversial reports as to the inflexibility of pain & physical disability.
What are the associated conditions of Scheuermann’s disease?
Numerous with Scheuermann’s complaint constantly have an extreme lordotic wind in the lumbar chine; this is the body’s natural way to compensate for the kyphotic wind over. numerous with Scheuermann’s complaint have veritably large lung capacities & males frequently have broad, barrel cases. Most patients have forced vital capacity( FVC) values above average. It has been proposed that this is the mortal body’s natural way to compensate for a loss of breathing depth.
frequently cases have tight hamstrings, which, again, is associated with the body compensating for an inordinate spinal curve, though this is also batted ( for illustration, some suggest the miserliness of ligament is the starting cause of the growth abnormality). In addition to the usual lordosis, it has been suggested that between 20 – 30 of cases with Scheuermann’s Disease also have scoliosis, though utmost cases are negligible. In more serious cases, nonetheless, the combination is classified as a separate condition known as kyphoscoliosis.
Patients with Scheurmann’s disease are likely to have a lower-than-average bone density. They’re hence at a statistically lesser long-term risk for osteopenia & osteoporosis, the reason for this is unknown.
- spondylolysis in the lumbar region
- dural cysts
- compensatory tightness of the anterior shoulder, hamstrings, & iliopsoas muscle
- non-orthopedic manifestations
- pulmonary issues in curves exceeding 100 degrees
What is the epidemiology of Scheuermann’s disease?
- Prevalence: 1% to 8% in the United States
- Gender: Male to female ratio is at least 2:1
- Age: Most usually diagnosed in adolescents 12-17 years
- Rarely diagnosed in children lower than 10 years.
- Classification: Type I (Classic) – Thoracic spine inclusion only, with the apex of curve T7-T9 Type II – Thoracic & lumbar involvement, with the apex of curve T10-T12
What are the complications of Scheuermann’s disease?
Potential complications:
- Progressive cosmetic deformity
- Chronic back pain
- Neurologic deficits or spinal cord compression
- Postoperative complications
- Pseudoarthrosis (most common complication)
- Persistent pain
What is the Differential Diagnosis of Scheuermann’s disease?
- Postural kyphosis (flexible postural deformity)
- Hyperkyphosis attributable to another known disease state
- Postsurgical kyphosis
- Ankylosing spondylitis
- Scoliosis
What is the diagnostic procedure for Scheuermann’s disease?
The adolescent will present with cosmetic/postural deformity & subacute thoracic pain. The deformity is significantly acknowledged in the early to mid-teenage years by the parents, child, or on a school screening examination. With respect to subacute thoracic pain, there is generally no identifiable inciting event. The pain is worse during activity & improved with rest.
Physical exam shows a rigid hyperkyphotic curve, emphasized with forward bending. The scheurmann’s hyperkyphosis does not fade away with an extension or lying prone or supine, further supporting the rigid nature of this condition. Other associated findings on an examination might include cervical or lumbar hyperlordosis, scoliosis, & tight hamstrings. Although neurologic deficits are not common, a thorough neurologic exam must be completed.
At each visit, the patient’s spinal range of motion should be assessed in all planes of motion: flexion/extension, right/left lateral bending, and right/left rotation. The degree of hyperkyphosis should also be followed over time by serial imaging to assess the degree of progression. Tracking the patient’s functional range of motion as well as the degree of deformity will assist guide the appropriate intervention and prognosis.
History & physical along with anterioposterior or lateral radiographs contain the important components for diagnosing Scheuermann kyphosis. Lateral radiographs are needed for diagnosis and diagnostic criteria include the following:
Rigid hyperkyphosis, greater than 40 degrees
Anterior wedging, more than or equal to 5 degrees in three or more adjoining bodies of the vertebra
Procedure for Determining the Degree of Kyphosis on Lateral Imaging
- The line is drawn initiating from the superior endplate of the most tilted vertebrae on the cephalad area of the kyphotic curve
- The line is drawn initiating from the inferior endplate of the most tilted vertebrae on the caudal part of the kyphotic curve
- The angle we get by the intersection of lines perpendicular to the above-explained lines is the measured Cobb angle
- Hyperkyphosis is explained as measured Cobb angle greater than 40 degrees
Procedure for Determining the Degree of Anterior Wedging with Lateral Imaging
- The line is drawn starting from posterior to anterior along the superior endplate
- The line is drawn initiating from posterior to anterior along the inferior endplate
- The angle we get by the intersection of these lines anteriorly is the measured Wedge angle
- Anterior wedging of greater than or equal to 5 degrees in 3 or more adjacent vertebral bodies, with an associated rigid hyperkyphosis greater than 40 degrees, is diagnostic for Scheuermann disease
Other Associated Findings Noted on AP/Lateral Radiographs
- Irregular vertebral endplates
- Schmorl nodes
- Loss of disc space height
- Scoliosis
- Spondylolysis/spondylolisthesis
- Disc herniation
Neurological screening: rarely the spinal cord can be stretched over the posterior region of the vertebral bodies at the apex of the curvature which might cause neurological features of impending paraplegia with clonus & hyperreflexia.
Adam’s forward-bend test: Scheuermann’s kyphosis can be accompanied by scoliosis.
Muscle length testing: the condition can be accompanied by tightness of the M. Pectoralis, M. Hamstrings, M. sub occipitalis, and the hip flexors with possible contractures of the anterior shoulder and hip
Range of motion: Flexibility of the extremities & spine can determine impairments and track changes over time.
Muscle strength testing: strength of the abdominals, core, trunk extensors, & gluteal muscles must be assessed.
Although typically not a necessity, MRI can be helpful to further diagnose anatomic changes or for pre-operative planning. CT imaging is usually not required. There are also no specific laboratory tests or histologic findings needed for the diagnosis of Scheuermann kyphosis.
What is the treatment plan for Scheuermann’s disease?
Conservative treatment for Scheuermann’s disease:
Scheuermann’s complaint is tone-limiting later growth is finished, intending that it generally runs its course & noway hand over further complications. generally, still, once the case is fully grown, the bones will maintain the disfigurement. For that reason, there are multitudinous operation procedures & options available that target correct kyphosis while the spine is still growing, and especially aim to help it from worsening.
Because the disease is frequently benign, & because back surgery includes numerous risks, surgery is usually considered the last option for patients. In severe or extreme cases, cases might be managed through an extensive surgical procedure in an effort to prevent the disease from worsening or harming the patient’s body.
In Germany, a quality treatment of specialized physical therapy for both Scheuermann’s condition & lumbar kyphosis is the Schroth technique, it is a system for scoliosis and other related spinal deformities. This method has been manifested to decrease pain & decrease kyphotic angle significantly during an inpatient treatment program.
Bracing can be employed to help avert progression & in some cases reduce the hyperkyphosis Cobb angle. Conservative treatment of Scheuermann’s hyperkyphosis in foreign research is naturally regarded as a productive treatment option. Physiotherapy & bracing are the first-line approaches for this condition.
Braces analogous to the Scolibrace & Kyphologic brace systems have been exposed to be productive in the treatment of Scheuermann’s case.
Stretching, lifestyle modification, NSAIDs, physical therapy
- Indication:
- Kyphosis less than 60 degrees and asymptomatic
- The majority of patients come into this category
- Patients typically do better without significant long-term sequelae
Extension bracing plus “A”
- Indication:
- Kyphosis 60 to 80 degrees plus/minus symptomatic
- Course
- Bracing is typically needed for 12 to 24 months
- Most effective in skeletally immature patients
Typically, doesn’t improve the curve but rather impedes progression
Braces
Milwaukee brace
Kyphologic brace
Thoracolumbosacral orthosis-style Boston brace
Surgical treatment for Scheuermann’s disease:
Spinal fusion, typically a combination of anterior release + fusion as well as posterior instrumentation + fusion
Indications
- Kyphosis greater than 75 degrees causes unacceptable deformity
- Kyphosis more than 75 degrees with associated pain
- Neurologic deficit/spinal cord compression
- Severe refractory pain
Scheuermann’s complaint can be successfully done right with surgical methods, almost a total of which involve spinal fusion & hardware instrumentation, e.g., screws, rods, pedicles, etc. While many patients are typically interested in catching surgery for their posture correction, it is important to know that the surgery aims to decrease pain & not a cosmetic defect. As always, the surgical technique should be utilized as a last resort once conservative treatment backslides or the patient’s health is in imminent danger as any surgical procedure is not without risk. Nevertheless, the chances of complications are relatively low, and the surgeries are frequently successful.
There are 2 primary surgical techniques to redress kyphosis one posterior-only fusion and the other anterior/posterior fusion. While debate lingers over which surgical approach is best, several studies published since 2018 advocate treatment trends favoring posterior-only fusion.
The traditional surgical technique requires placing 2 rods of titanium, which are roughly one and a half feet long (it depends on the size of the kyphosis) into the back on each of the 2 sides of the spine. Eight titanium screws & hardware are drilled through the bone to fasten the rods onto either side of the spine. On the internal side of the spine, ligaments (which can be too small, and retain the spine back into its abnormal shape) must be surgically released or cut, not only stooping part of the cause of the kyphosis but also allowing the titanium rods to stretch the spine into a more natural position. The damaged discs between the wedged vertebrae are normally removed & replaced with bone grafting from the hip or other parts of the vertebrae, which once healed or “fused” will solidify. The titanium instrumentation holds everything in its space during healing. The patient can expect to remain in the hospital for a least a week, & possibly longer. They might then be required to wear a brace for several months more to make sure the spine heals appropriately. The titanium instrumentation might remain in the body permanently, or be removed years later. Patients who have undergone such surgery might need physical therapy to manage pain & mobility. Recovery can be elongated: typically patients are not allowed to lift weight anything above 5–10 pounds (2.3–4.5 kg) for 6 months to 1 year, & many patients are out of work for at least 6 months. Nevertheless, once the fusion is solidified, most patients can go back to their routine life within 1–2 years.
Physiotherapy treatment for Scheuermann’s disease:
Non Surgical Treatment
Children with little kyphosis might simply need observation for changes in the thoracic curve and also educate them on their posture & activities by the physiotherapist.
Unless the curve or pain becomes worse, no other treatment might be required.
Some children eventually get better without having a noticeable abnormal kyphosis & have no long-term problems.
few patients with mildly exaggerated thoracic kyphosis are able to function normally without any pain or other complications.
The doctor might suggest bracing along with exercise.
A brace is most effective when utilized before the skeleton matures at about age 14.
Ideally, bracing should begin at the start of puberty, be worn for approximately 2 years, & removed at the end of skeletal maturity.
Doctors usually chose a Milwaukee brace, which contains molded plastic that conforms to the waist &gradually straightens the thoracic curve, and is designed to hold the shoulders posteriorly. The brace has 2 upright bars, and padded bars line up along the sides of the spine. The force from the upright bars straightens the spine but is not helpful for rigid curves that angle more than 75 degrees.
Bracing
Younger patients generally carry the brace for whole the time including at night, although they commonly remove the brace to shower.
The doctor adjusts the brace in routine as the curve improves.
When the thoracic curve has regained its normal curve, the brace is removed for a few hours until the bones are completely mature, which is typically around age 14 or 15.
In adult Scheunemann patients we can gain half correction of the kyphosis & pain relief with the help of bracing even after they have gained full bone maturity. Bracing for pain relief in adults is also given when surgery is not an option.
Physiotherapy is recommended in combination with bracing.
Exercises seem to enhance the effect of the brace by strengthening muscles that assist align the spine
The therapist can advise posture & activity modification which can be very useful in the management of kyphosis.
Even without a brace, physiotherapy is recommended to assist with any pain that might be present and to teach proper posture correction to treat any muscular imbalances present in the spine.
Doctors might prescribe anti-inflammatory medication for pain. Younger patients usually utilize medicine on a short-term basis, in combination with other treatments. Adults who have ongoing pain sometimes need long-term usage of anti-inflammatory medication.
According to Lowe, treatment with the use of a brace is almost always fruitful in patients with kyphosis in the range of 55 degrees to 80 degrees if the evaluation is done before skeletal maturity.
Bracing therapy has a few shortcomings: as the bracing time is elevated the chances of getting low back pain increases
In adolescents, compliance is commonly low.
Other bracing types can also be attempted such as the usage of a soft brace but this however has not shown to be successful. With a soft brace, zero correction can be achieved in rigid curvatures.
Other aspects of Physiotherapy Treatment
- Patient education includes:
Extension-based stretching/strengthening program
Hamstring stretching exercise program
Proper postural & body mechanic techniques for ADLs
Appropriate use & handling of braces
- Postural improvement:
Targets on hamstring & pectoralis stretching and trunk extensor strengthening as well as improving function.
These exercises can be useful when the thoracic spine has not started a relevant stiffness & when the sagittal curve is not too high: Cobb angles from 44° to 55°.
Practice normal posture standing and sitting
- Exercises:
Flexibility exercises to release lower extremity contractures eg. Hamstrings
Strengthen core musculature and back extensors.
- Sports:
Extension sports are suggested: such as swimming, gymnastics, aerobics, basketball, cycling, & hyperextension exercises.
Some sports should be alarm: like sports associated with jumping, marked stress, & functional overuse of the back.
- Postoperative physical therapy:
Necessary and must contain breathing exercises, mobilizations, & strengthening exercises.
Scheuermann’s disease in adults
Regarded differently from that of the younger because the main manifestation is pain & not aesthetic quality.
Functional rehabilitation on an OPD basis is the advocated management & referrals for surgery or dorso-lumbar braces are infrequent.
The kyphotic posture can be managed with the Schroth method
Examples of Schroth exercises are described in R
Another treatment regime is outlined here, using a different method There are five Principles of Correction:
- Trunk elongation & Expansion
- Symmetrical sagittal straightening: identical exercises must be done for both sides of the trunk (right & left): Bilateral thoracic expansion in a posterior to anterior (PA) direction to decrease the thoracic hyperkyphosis. Bilateral lumbar expansion in an anterior to posterior (AP) direction to decrease the hyperlordotic low back
- Shoulder traction: the traction improves the expansion of the thorax & corrects the spine
- Correction of breathing: it allows the patient to feel an increased expansion in his or her initially collapsed regions. The goal is to expand the thorax in a back-to-front & a lateral direction.
- Muscle activation by increasing tension: to target the best possible correction, muscle balance, and stabilization & to increase the proprioceptive input. It assists to integrate the ‘corrected body schema’ in the brain.
- To manage adult Scheunemann patients intense physical therapy incorporated with bracing is utilized.
More clinical trials are needed to find the effectiveness of conservative interventions, especially different exercises & manual therapies. This should also be combined or compared with braces.
What is the prognosis of Scheuermann’s disease?
The majority of patients are successfully managed with conservative measures, as previously discussed. Pain in the involved part typically gets better after it is reached skeletal maturity, although patients with kyphosis are at elevated risk of chronic back pain as compared to the other population. Long-term follow-up studies typically advocate a lower health-related quality of life & increased back pain in adulthood.
Patients with kyphosis lower than 60 degrees at skeletal maturity significantly have no long-term sequelae.
Back pain in adults that so rarely limits daily activities (mild curves with a mean of 71 degrees)
Curves >75 degrees are prone to cause severe thoracic pain
Studies suggest at least some improvement in 80% of patients but not frequent to severe deformity
Long-standing compensatory lumbar hyperlordosis might lead to lumbar spondylolysis
Spinal fusion for kyphosis & scoliosis is an exceedingly invasive surgery. The risk of complications is estimated to be about 10 percent. Possible complications might be inflammation of the soft tissue or deep inflammatory processes, breathing impairments, bleeding, nerve injuries, or infection. As early as five years after surgery around 5% need reoperation & long-term issues remain unclear. Taking into consideration that some of the symptoms of spinal deformity cannot be influenced by spinal surgery, it stays a cosmetic indication, though the cosmetic effects of surgery are not necessarily stable.
FAQ (frequently asked questions)
Scheuermann’s disease is characterized by vertebral body wedging, diminished anterior vertebral growth, vertebral endplate irregularity, Schmorl’s nodes, narrowing of the intervertebral disc spaces, & premature disc degeneration.
Scheuermann’s disease affects children aged 13 to 16 years, & the diagnosis is rarely made in patients younger than 10 years.
Scheuermann’s disease, or Scheuermann’s kyphosis, is a disease in which a child has too much curvature (or kyphosis) in the middle of the back. Kyphosis typically happens during periods of accelerated growth. If the front of the spine does not grow as quickly as the back of the spine, the vertebrae become wedge-shaped.


One Comment