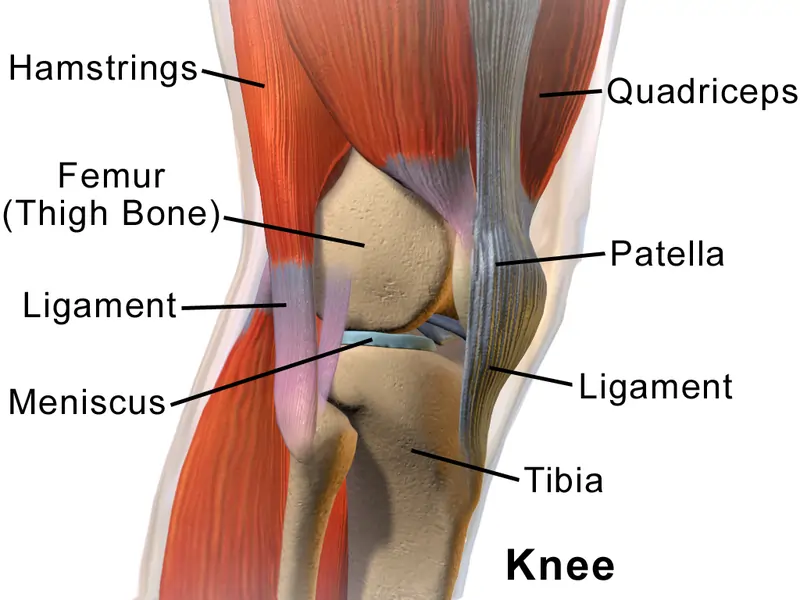
Knee joint with muscles
The knee joint with muscles plays an important role in the functioning of knee movement, such as quadriceps, Hamstring are the main muscles of knee joint which helps to perform day-to-day activity like walking, sitting to stand, running, and stair climbing.
Table of Contents
What is the knee joint?
- A knee joint is a synovial joint that connects three bones; a femur, tibia as well as patella. This is a complex hinge joint composed of two articulations; a tibiofemoral joint & patellofemoral joint. A tibiofemoral joint is an articulation between a tibia as well as the femur, while a patellofemoral joint is an articulation between the patella and the femur as well.
- The knee joint is the largest & arguably the most stressed joint in a body. An arrangement of the bones in a joint provides the fulcrum that translates the actions of the flexor & extensor muscles of the knee joint. An arrangement of the extracapsular & intracapsular & ligaments, as well as extensions of muscles that cross a joint, provide the much-needed stability that counters considerable biomechanical stress brought upon a joint.
- As the hinged joint, a knee joint mostly allows motion along one axis in terms of flexion as well as an extension of a knee in a sagittal plane.
- This also allows slight medial rotation while flexion & the last stage of extension of a knee, as well as lateral rotation when “unlocking” a knee.
Articular surfaces
- A tibiofemoral joint
A tibiofemoral joint is an articulation between lateral as well as medial condyles of a distal end of a femur & the tibial plateaus, both of which are covered by a thick layer of hyaline cartilage.
A lateral, as well as medial condyles, are two bony projections located at a distal end of a femur, which have a smooth convex surface, & are separated posteriorly by the deep groove known as an intercondylar fossa. A medial condyle is larger, more narrow as well as further projected than its lateral counterpart, which accounts for the angle between the femur and the tibia. The roughened outer surfaces of the medial & lateral condyles are defined as medial as well as lateral epicondyles, respectively. Along with a posterior aspect of the distal femur, there are paired rough elevations above the medial as well as lateral epicondyles known as a medial & lateral supracondylar ridge. - The patellofemoral joint
A patellofemoral joint is the saddle joint formed by an articulation of a patellar surface of the femur (also known as a trochlear groove of the femur) as well as a posterior surface of the patella. A patellar surface of the femur is a groove on the anterior side of the distal femur, which extends posteriorly into an intercondylar fossa.
A patella is a triangular-shaped bone, with a curved proximal base & a pointed distal apex. The articular surface is defined by medial as well as lateral facets which are concave articular surfaces covered with a thick layer of hyaline cartilage & separated by the vertical ridge. Medial to a medial facet is a third minor facet, known as an ‘odd’ facet which lacks hyaline cartilage.
Being the sesamoid bone, a patella is tightly embedded & held in place by a tendon of the quadriceps femoris muscle. On a distal part of the patella, the extension of the quadriceps femoris tendon forms the central band called a patellar ligament. This is a strong, thick ligament that extends from a patellar apex to a superior area of a tibial tuberosity.
The joint capsule, ligaments, and menisci of the knee joint
- A joint capsule of a knee joint is one of composite nature, mainly formed by muscle tendons & their expansions, forming a thick ligamentous sheath around the knee joint. A capsule is relatively weak & attached to the margins of the femoral as well as tibial articular surfaces. An anterior portion of a capsule features the opening, whose margins attach to the borders of a patella. The second gap is also present in a lateroposterior portion of a knee capsule to give passage to a tendon of the popliteus muscle.
- A capsule is formed from an outer fibrous layer (which is continuous with adjacent tendons) & an inner synovial membrane that lubricates articular surfaces, decreasing friction in addition to providing nourishment to cartilage. A joint capsule forms several fluid-filled pouches called bursae, that decrease friction within a knee joint. Notable bursa of a knee joint include the:
- Suprapatellar bursa – Located superior to a patella between a femur & the tendon of the quadriceps muscle.
- Prepatellar bursa- Lies in front of a patella between a patella & the skin.
- Infrapatellar bursa – Located under a patella between a patellar ligament as well as the tibia.Ligaments
- The ligaments of a knee joint may be divided into two groups; extracapsular ligaments as well as intracapsular ligaments. These ligaments connect a femur as well as the tibia, holding them in place, providing stability, & preventing dislocation.
Extracapsular ligaments are found outside a joint capsule & include a patellar ligament, fibular (lateral) as well as tibial (medial) collateral ligaments, and oblique and arcuate popliteal ligaments. Intracapsular ligaments are found inside a knee joint capsule, with the cruciate ligaments being the most well-known of this subgroup. - Patellar ligament
A patellar ligament is the strong, thick fibrous band that is the distal continuation of the quadriceps femoris tendon. This is found superficial/anterior to an infrapatellar bursa & extends from an apex of the patella to a tibial tuberosity. - Lateral (fibular) collateral ligament
A fibular collateral ligament is a strong ligament that originates from a lateral epicondyle of a femur, just posterior to a
the proximal attachment of a popliteus, & extends distally to attach on a lateral surface of a fibular head. - Medial (tibial) collateral ligament
A tibial collateral ligament is a strong, flat ligament of a medial aspect of a knee joint. A tibial collateral ligament, moreover to its fibular counterpart, acts to secure a knee joint & prevent an excessive sideways motion by restricting external as well as internal rotation of the extended knee. A tibial collateral ligament has sometimes divided literature into superficial as well as deep parts. - Oblique popliteal ligament
An oblique popliteal ligament (Bourgery ligament) is the expansion of a semimembranosus tendon that originates posterior to a medial tibial condyle & reflects superiorly as well laterally to attach on a lateral condyle of a femur. - Arcuate popliteal ligament
The arcuate popliteal ligament is the thick, fibrous band that arises on a posterior aspect of a fibular head & arches superiorly as well as medially to attach on a posterior side of a joint capsule of the knee. An arcuate popliteal ligament reinforces a posterolateral part of the knee joint capsule, & together with an oblique popliteal ligament, prevents overextension of a knee joint. - Anterior cruciate ligament
The anterior cruciate ligament arises from an anterior intercondylar area of a tibia just behind the attachment of a medial meniscus, & extends posterolaterally & proximally to attach on the posterior part of a medial surface of a lateral femoral condyle. As it crosses to another side of the knee joint, the ACL ligament passes underneath a transverse ligament & blends with an anterior horn of the lateral meniscus. An anterior cruciate ligament is important to prevent posterior rolling as well as displacement of a femoral condyle while flexion, as well as to prevent hyperextension of a knee joint. - Posterior cruciate ligament
The posterior cruciate ligament arises from a posterior intercondylar area of a tibia & extends anteromedially & proximally to attach to an anterior part of a lateral surface of a medial femoral condyle. The ligament is almost twice as strong & has a better blood supply than an anterior cruciate ligament. A posterior cruciate ligament has the opposite function of an anterior cruciate ligament, serving to prevent anterior rolling as well as displacement of a femoral condyle while extension, as well as to prevent hyperflexion of a knee joint as well as to prevent hyperflexion of a knee joint. - Menisci
Menisci are fibrocartilaginous crescent-shaped plates found between articular surfaces of a femur & tibia and serve to
provide their congruence as well as shock absorption. The menisci are thick as well as vascularized in their outer one-third, while their inner two-thirds are thinner & avascular. Moreover, the inner two-thirds contain radially organized collagen bundles, whilst the outer third contains larger circumferentially arranged bundles. Hence, it is believed that an inner portion is more adapted for weight-bearing & resisting compressive forces, whereas the outer portions are suited for resisting tensional forces.
Movements
- Being the hinge joint, the main motions in a knee joint are flexion as well as the extension of a knee in the sagittal plane. This also allows limited medial rotation in the flexed position & in the last stage of extensions well as lateral rotation when “unlocking” & flexing the knee. Unlike an elbow joint, a knee joint is not a true hinge since it has the rotational component, an accessory movement that accompanies flexion as well as extension, therefore it is termed a modified hinge joint.
Muscles of the knee joint
Muscles near the Knee joint mainly are Quadriceps muscles which are located at the front side of the thigh while Hamstring muscles are located at the Back of the thigh and the Calf muscles which are originated around the knee joint located at the Back of the leg.
List of Muscles near Knee Joint:
- Quadriceps muscles:
- Rectus Femoris
- Vastus Medialis
- Vastus intermedius
- Vastus Lateralis
- Hamstring Muscles
- Biceps Femoris
- Semitendinosus
- Semimembranosus
- Calf muscles
- Gastrocnemius
- Plantaris
- Popliteus Muscle
Rectus Femoris
Description
- It is part of the quadriceps group. Rectus Femoris is the bulk of muscle located in a superior, anterior middle compartment of the thigh as well as it is the only muscle in the quadriceps group that crosses a hip.
- This is the superior & overlying of a vastus intermedius muscle & superior-medial part of the Vastus lateralis & Vastus medialis.
- The word rectus is the Latin word connoting “straight”. So, a rectus femoris received its name due to it runs straight down a thigh.
- This is a two-way acting muscle as it crosses over a hip & knee joint; hence, it functions to extend a knee & also helps iliopsoas in hip flexion.
- The short rectus femoris can contribute to a higher positioned patella in relation to a contralateral side. A markedly shortened rectus femoris is suggested by the knee flexion of less than 80°or even by marked prominence of superior patellar groove.
Anatomy
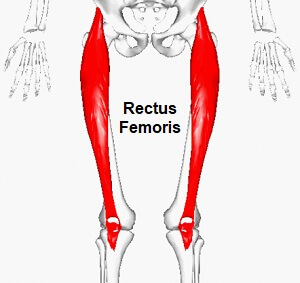
- Origin: Originates from the anterior inferior iliac spine(AIIS) as well as the part of alar of ilium superior to an acetabulum.
- Insertion: Rectus Femoris together with vastus medialis, vastus lateralis as well as vastus intermedius join the quadriceps tendon to insert at a patella & tibial tuberosity (via patellar ligament).
- Nerve supply: Rectus Femoris is innervated by a femoral nerve, originating from lumbar nerve 2, 3, & 4 nerve roots.
- Bloody supply: Blood is supplied to a Rectus Femoris via descending branch of a lateral circumflex femoral (LCF) artery.
- Function:
- Hip flexion: Rectus Femoris acts with iliopsoas to produce hip flexion especially if a knee is flexed. During gait, as the hip flexor, it acts with the iliopsoas in the “Toe off” phase.
- Knee extension: Together with other muscles that are part of the Quadriceps femoris, this facilitates knee extension. In the terminal swing phase rectus femoris acts as the extensor of a knee, as the muscle in the quadriceps group, this generates force needed for loading(foot flat phase) in the stance phase.
The Rectus femoris is more efficient in motion combining hip hyperextension as well as knee flexion or even from the position of knee extension and hip flexion as well. For instance, kicking a soccer ball.
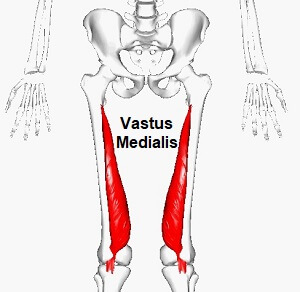
Vastus Medialis
Description
- The Vastus medialis muscle is one of the four muscles that make up the quadriceps group of muscles. This originates from the upper part of a femoral shaft & inserts as the flattened tendon into the quadriceps femoris tendon, which inserts into an upper border of a patella.
Anatomy
- Origin: The lower part of an intertrochanteric line, along with the spiral line to a medial lip of a linea aspera, a medial intermuscular septum as well as an aponeurosis of adductor Magnus.
- Insertion: Into a medial side of the quadriceps tendon, joining with rectus femoris & the other quadriceps muscles, enveloping a patella, then by a patellar ligament into a tibial tuberosity.
- Nerve supply: The branch from a posterior division of a femoral nerve is derived from L2, 3, and 4.
- Blood supply: Femoral artery as well as branches from a profunda femoris artery.
- Function: Vastus medialis, together with another muscle that makes up the quadriceps femoris, extends a knee joint & it also contributes to the correct tracking of a patella.
Clinical relevance
- Weakness of a vastus medials is associated with patellar maltracking & patellofemoral pain. The approach to treatment attempts to restore the balance between vastus medialis as well as lateralis, which requires strengthening of oblique fibers of the medialis, and assessment of the degree of dynamic supination as well as pronation of the foot.
- VMO strengthening has become a less popular approach to the treatment of anterior knee pain as the evidence supporting isolated exercises has been criticized for its poor quality.
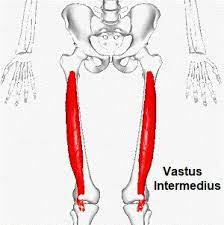
Vastus intermedius
Description
- It is located centrally, underneath the Rectus femoris in an anterior compartment of the thigh & on each side of it:
- Vastus medialis as well as Vastus Lateralis respectively. This is one of the four muscles that form the quadriceps femoris muscle. The tensor of the Vastus Intermedius is the new muscle that is part of the Quadriceps.
Anatomy
- Origin: Originating from the upper two-thirds of the anterior as well as lateral surfaces of a femur & the intermuscular septum.
- Insertion: Inserting via a Quadriceps femoris tendon to form a deep part of a tendon & then inserts into a lateral margin of a patella.
- Blood supply: A descending branch of a lateral circumference femoral artery supplies the muscle.
- Nerve supply: A Vastus Intermedius muscle is innervated by the branch of a Femoral nerve, originating from lumbar nerve 2, 3, as well as 4 nerve roots.
- Function: Together with other muscles that are part of a Quadriceps femoris, this facilitates knee extension.
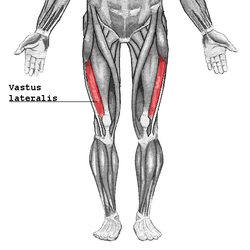
Vastus Lateralis
Description
- A vastus lateralis muscle is located on a lateral side of a thigh. The muscle is the largest of the quadriceps which includes: the rectus femoris, vastus intermedius, as well as vastus medialis. Together, the quadriceps act on a knee & hip to promote motion & strength as well as stability. They provide power for & absorb the impact of daily activities namely walking, running, as well as jumping.
Anatomy
- Origin: Upper inter-trochanteric line, the base of the greater trochanter, lateral linea aspera, lateral supracondylar ridge as well as the lateral intermuscular septum.
- Insertion: Lateral quadriceps tendon which attached to a tibial tubercle.
- Nerve Supply: The posterior division of the femoral nerve (L3,4).
- Blood Supply: A lateral circumflex femoral artery
- Function: Extension of a knee joint.
- Functional contributions: In everyday life, the quadriceps muscle group as the whole allows the individual to stand up from sitting, walk up, or even downstairs along with basic walking as well as running. These muscles are not active during standing with knees fully extending, but become active while a heel-strike as well as toe-off phases of gait.
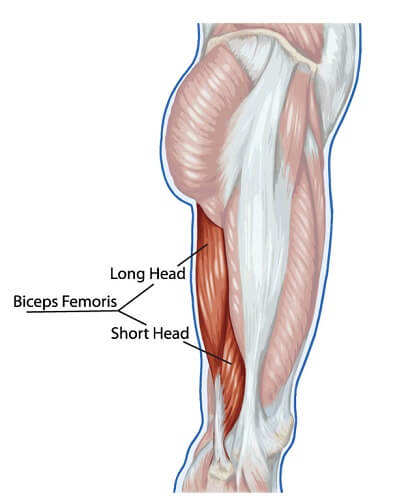
Biceps Femoris
Description
- The Biceps femoris is the muscle of a posterior compartment of a thigh, as well as lies in a posterolateral aspect. This arises proximally by two ‘heads’, termed a ‘long head’ (superficial) as well as a ‘short head’ (deep). This is part of the hamstrings.
Anatomy
- Origin: Long head: Ischial tuberosity. Short head: Linea aspera as well as a lateral supracondylar line of the femur.
- Insertion: Lateral aspect of the fibular head.
- Nerve Supply: Long head: Tibial division of a sciatic nerve (L5-S2). Short head: Common peroneal division of the sciatic nerve.
- Blood Supply: Perforating branches of the profunda femoris, inferior gluteal, as well as medial circumflex femoral arteries.
- Function:
- Action: Long head: Flexes a knee, extends the hip, laterally rotates the lower leg when the knee is slightly flexed, and helps in lateral rotation of the thigh when the hip is extended. Short head: Flexes a knee, and laterally rotates the lower leg when the knee is slightly flexed.
- Functional contributions
- Through the reversed origin insertion action, a long head gives posterior stability to a pelvis. Both heads provide rotary stability by preventing forward dislocation of a tibia on a femur while flexion. Its contributions to an arcuate ligament complex at a posterolateral corner of a knee also provide varus as well as rotatory stability to a knee.
Clinical relevance
- An individual knows that the biceps femoris muscle usually has two heads, namely the short head as well as the long head of the biceps femoris. These two heads insert on a head of the fibula, where at the site of insertion which divides into two portions by the fibular collateral ligaments.
- Any sort of subluxation or even dislocation of the biceps femoris tendon or abnormal insertion of a tendon, & any or no trauma, meniscal instability may lead to Snapping Biceps Femoris Tendon. This is an unusual condition with symptoms of pain on the lateral side of the knee, the fibular head will be prominent, painful snap on the lateral aspect of the knee while active as well as passive knee flexion at 90 degrees & difficulty in performing ADL’s or sport related activities.
- During performing sprinting there will be an abrupt rise or even alter in the speed of running because of which biceps femoris muscle, as well as semi tendinosis present at the back of the thigh, are usually hurt causing over-stretching of such muscles.
- An injury to the Long head of the biceps femoris tendon as well as semitendinosus is most common among soccer players leading to sport-related injuries.
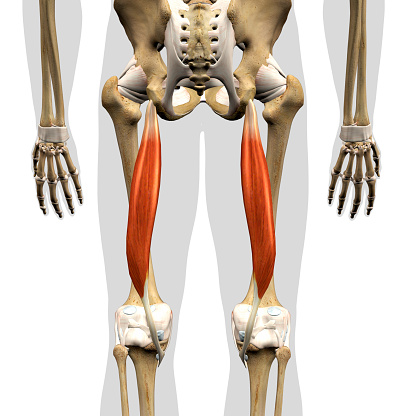
Semitendinosus
Description
- This muscle is one of the three muscles that make up the hamstrings muscle group, & it is located at the posterior as well as the medial aspect of the thigh. A semitendinosus is so named because of it has a long tendon of insertion.
- A muscle is fusiform & ends a little below the middle of the thigh in the long round tendon that lies along a medial side of a popliteal fossa; it then curves around a medial condyle of a tibia & passes over a medial collateral ligament of a knee-joint, from which it is separated by the bursa, & is inserted into an upper part of a medial surface of a body of a tibia, nearly as far forward as its anterior crest.
- A semitendinosus is more superficial than a semimembranosus (with which it shares very close insertion as well as attachment points). However, owing to the semimembranosus being wider as well as flatter than a semitendinosus, this is still possible to palpate a semimembranosus directly.
- At its insertion, it gives off from its lower border the prolongation to a deep fascia of a leg & lies behind a tendon of a sartorius, as well as below that of a gracilis, to which it is united. These three tendons form a Pes Anserinus, hence named because of the appearance resembling the webbed “goose’s foot”.
Anatomy
- Origin: This arises, from a common tendon origin with a long head of a biceps femoris, from a lower medial facet of a lateral section of an ischial tuberosity. A semitendinosus muscle mainly originates from a medial surface of a tendon of a long head of the biceps femoris, as well as also originates from an ischial tuberosity with the thin tendon & a muscular part.
- Insertion: A semitendinosus tendon inserts at an upper part of a medial surface of a tibia, behind an attachment of the sartorius & infero-anterior to internment of gracilis.
- Nerve Supply: A tibial portion of a sciatic nerve (L5, S1, 2).
- Blood supply: Branches from an internal iliac, popliteal, as well as profunda femoris arteries.
- Function: Extension of a thigh at a hip. Agonists: Gluteus maximus, semimembranosus, biceps femoris (long head), as well as adductor Magnus (posterior part). Antagonists: Psoas major as well as iliacus. A semitendinosus is also the weak medial rotator of a hip.
- Flexion of a leg at the knee. Agonists: Biceps femoris (long head), biceps femoris (short head), as well as semimembranosus. Antagonists: Vastus lateralis, vastus medialis, vastus intermedius, as well as rectus femoris. Gracilis, sartorius, popliteus, gastrocnemius, as well as plantaris assist with flexion of the knee.
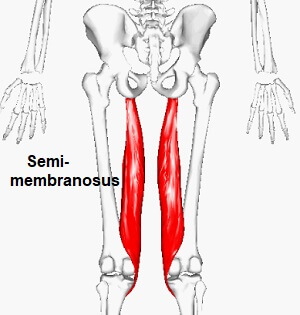
Semimembranosus
Description
- This is one of a group of muscles called the Hamstrings. This is located on a posteromedial side of the thigh deep to Semitendinosus as well as medial to the Biceps Femoris. Its origin is an ischial tuberosity on an inferior pelvis & it has the complex distal insertion connected to the Popliteus Muscle, to a Medial meniscus, to a Medial Collateral Ligament as well as to the Tibia. In the lower part of the thigh, semitendinosus as well as semimembranosus together form an upper medial boundary of a popliteal fossa.
- Its primary action is knee flexion, knee internal rotation as well as hip extension. It also plays the main role in providing knee stability. A semimembrAtal tendon is a major component of a posteromedial corner of a knee.
Anatomy
- Origin: The strong membranous tendon attaches to an upper lateral facet on a rough part of an ischial tuberosity.
- Insertion:
The anatomy of a distal insertion of a semimembranosus may be described as a distal semimembranosus complex: in fact, six different semimembranosus insertions may be identified. Anatomic dissection revealed six insertions of a distal semimembranosus tendon: direct arm, anterior arm, posterior oblique ligament extension, oblique popliteal ligament extension (capsular arm), distal tibial expansion (popliteus aponeurosis), as well as meniscal arm:
A direct arm attaches in the groove at a posteromedial aspect of a tibia;
An anterior arm courses more anteriorly & attaches to a tibia deep to a medial collateral ligament.
The broad component extends into an oblique popliteal ligament, which courses along with the posterior capsule of a knee. Some authors suggest more precise nomenclature renaming this ligament as an oblique popliteal tendon/expansion due to its function.
An insertion that is directed towards the components of a posterior oblique ligament has been described as a capsular arm. An entire posterior oblique ligament is inseparable from a capsule.
The short meniscal arm attaches to a meniscotibial ligament (coronary ligament) of a posterior horn of a medial meniscus.
The distal arm also extends over a popliteus muscle & its aponeurosis. This is a fascia-like structure extending from an inferior aspect of the direct arm over a popliteus muscle.
Additional connections to a posterior capsule as well as lateral meniscus have been reported. The tendiTheof a semimembranosus inserted into a posterior horn of a lateral meniscus was found in 43.2% of the knees.
The bursae separate a muscle from a medial head of a tibia & the medial head of a Gastrocnemius. - Nerve supply: Tibial division of a Sciatic Nerve (root value L5, S1, and 2). The nerve supply for the skin covering the muscle is L2.
- Blood supply: Branches from an internal iliac, popliteal, as well as profunda femoris arteries.
- Function: The functions of the distal semimembranosus complex may be summarized as follows:
Hamstrings generally play the role of hip extension as well as knee flexion. Otherwise, a semimembranosus alone is the hip extensor as well as a knee flexor/intrarotator. - In knee extension, a semimembranosus tendon prevents valgus, while in knee flexion it prevents external rotation.
A distal semimembranosus complex stabilizes the posterior capsule through an oblique popliteal ligament. In fact, on the knee flexion during running, cutting, and pivoting, the capsular arm of the semimembranosus actively tightens the posterior oblique ligament providing dynamic stability. In addition, an oblique popliteal ligament plays a significant role in preventing both excessive external knee rotation as well as hyperextension & in strengthening the stability of a knee. - A semimembranosus acts synergistically with a popliteus muscle through a fibrous extension towards this muscle.
- A distal semimembranosus complex actively pulls a posterior horn of a medial meniscus, protecting it from being crushed between a medial femoral condyle & a posterior medial tibial plateau while knee flexion. Moreover, it provides the element of the posterior traction over a posterior horn of a lateral meniscus, along with the structures forming a stabilizing mechanism of a posterolateral aspect of the knee.
- Hip extension
Agonists: Gluteus Maximus, semitendinosus, Biceps Femoris (long head), as well as Adductor Magnus (posterior part)
Antagonists: Psoas Major and Iliacus as well. - Knee flexion
Agonists: Biceps femoris (long head), biceps femoris (short head), as well as semitendinosus. However, a dynamic synergy of a semimembranosus complex & the biceps femoris also provides for pulling posterior horns of a medial as well as lateral menisci.
Antagonists: Vastus Lateralis, Vastus Medialis, Vastus Intermedius, as well as Rectus Femoris, Gracilis, Sartorius, Popliteus, gastrocnemius, & plantaris assist with flexion of a knee. - Knee internal rotation of a knee when it is flexed
Agonists: Popliteus and semitendinosus as well.
Antagonists: Biceps femoris (long head) as well as biceps femoris (short head).
Sartorius and Gracilis assist with the internal rotation of a knee when a knee is flexed. - Functional movements
Stand from sitting, walking upstairs, standing jump forwards, as well as standing jump upwards.
Clinical relevance
- Hamstring Syndrome
The pathology commonly affects athletes who present with localized pain near an ischial tuberosity. Pathophysiology is thought to be that of the insertional tendinopathy at an ischium but there can also be involvement of the sciatic nerve compression. A pain in hamstring syndrome radiates down a posterior thigh or even popliteal region & is exacerbated when the hamstrings are in tension. It is often seen in sprinters or even hurdlers. On examination there is exquisite tenderness over an ischial tuberosity & percussion in that region can reproduce a sciatic distribution of the pain. Treatment involves rest, anti-inflammatory agents as well as steroid injections. - Baker’s cyst
A bursa that separates a muscle from a medial head of a tibia & the medial head of a Gastrocnemius may at times become enlarged with distended fluid. The swelling is termed ‘Baker’s cyst’ (described by Morrant Baker in the 19th century as the cystic mass in a popliteal fossa of children).
Gastrocnemius muscle
Description
- A gastrocnemius muscle is a complex muscle that is fundamental for walking as well as posture. Gastrocnemius forms a major bulk at the back of the lower leg & is a very powerful muscle. This is a two-joint or biarticular muscle & has two heads & runs from the back of the knee to the heel.
- The definitive shape of a calf is a result of a medial as well as lateral heads of a gastrocnemius, which is situated at a posterior, upper half of a lower leg. With the soleus as well as plantaris, they form the composite muscle called the triceps surae. The two heads of a muscle form the lower boundaries of a popliteal fossa. A gastrocnemius muscle is superficial, may be easily seen & can be touched on the back of the lower leg.
Anatomy

- Origin: The two heads are located from the medial as well as lateral condyles of a femur.
A medial head from behind a medial supracondylar ridge & an adductor tubercle on a popliteal surface of a femur.
A lateral head from an outer aspect of a lateral condyle of a femur, just superior as well as posterior to a lateral epicondyle. A fabella is an accessory ossicle almost always found in a lateral head of the gastrocnemius.
Both heads have attachments from a knee joint capsule as well as from an oblique popliteal ligament. - Insertion: A bulk of a gastrocnemius muscle from each of the heads comes together & insert into a posterior surface of the broad membranous tendon.
It then fuses with a soleus tendon to form an upper part of the tendocalcaneus.
The broad tendon then narrows until it reaches the calcaneus where it expands again for its insertion on a middle part of a posterior surface of the calcaneus. - Nerve supply: Both heads of the gastrocnemius are supplied by a tibial nerve (S1 and 2).
Cutaneous supply is mainly provided by L4, 5, and S2 as well. - Blood supply: A lateral as well as medial sural arteries, which are direct branches of a popliteal artery.
- Function: A gastrocnemius with soleus is the main plantar flexor of the ankle joint. A muscle is also the powerful knee flexor. This is not able to exert full power at both joints simultaneously, for instance when a knee is flexed, gastrocnemius is unable to generate as much force at the ankle. The opposite is true when the ankle is flexed.
- When running, walking, or even jumping the gastrocnemius provides a significant amount of propulsive force. Considering the amount of force needed to propel the body into the air, triceps surae may generate a lot of force.
- A gastrocnemius muscle tension has many fascial connections, & this tension is transmitted not only to the foot but to the knee, hip, as well as the lumbar area. The shortened gastrocnemius muscle could cause dysfunctions to physiological motions of a hip, reducing its anteversion (inward rotation of a femur). A fascial system plays a fundamental role in a transmission of a force produced by a contraction of the contractile component of a muscle.
Plantaris
Description
- A Plantaris muscle is a small muscle with a short belly as well as a long slender tendon that is located in a posterior compartment of a leg & along with a Gastrocnemius as well as Soleus muscles, form the Triceps Surae. A long, thin tendon of the plantaris is nicknamed the freshman’s nerve, as it is often mistaken for the nerve by first-year medical students during dissection. The muscle is believed to be an accessory muscle & only vestigial in humans, & and it might be absent in 7 to 20% of people.
Anatomy
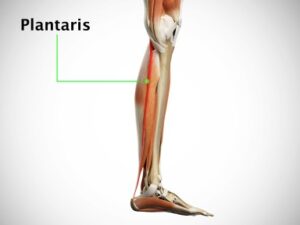
- Origin: This originates from a lower part of a lateral supracondylar line of a femur & from an oblique popliteal ligament of a knee joint as well as a muscle belly crosses a popliteal fossa inferomedially. In a proximal third of a leg, the muscle belly is situated between a popliteus muscle anteriorly as well as a lateral head of the gastrocnemius muscle posteriorly. Its long slender tendon courses distally between a medial head of a gastrocnemius muscle as well as a soleus muscle in the middle third of the leg.
- Insertion: A muscle inserts medially, in association with the Achilles tendon on a calcaneus, or even independently on a calcaneus.
- Nerve supply: Neural innervation of a plantaris muscle is provided by a tibial nerve (S1, S2).
- Blood supply: Arterial supply to a plantaris muscle is from a popliteal artery.
- Function: In terms of function, a plantaris muscle acts with a gastrocnemius but is insignificant as either the flexor of a knee or the plantar flexor of the ankle. It has been considered to be the organ of proprioceptive function for the larger, more powerful plantar flexors, as it contains a high density of muscle spindles.
- Primary Actions of a Plantaris
- A plantaris muscle is not the prime mover & does not have the primary action but helps with the actions of other muscles at the knee & ankle joints.
- Secondary Actions of the Plantaris: Give an aAssistexion of a knee, Agonists: Biceps Femoris, Semitendinosus, Semimembranosus Antagonists: Vastus Lateralis, Vastus Medialis, Vastus Intermedius, as well as Rectus Femoris.
- Helps with plantarflexion of the foot at the ankle. Agonists: Gastrocnemius, and Soleus.
Popliteus Muscle
Description
- A Popliteus is the small, thin, flat, triangular-shaped musculotendinous complex of a lower leg with a popliteus muscle & the popliteofibular ligament as well as constitutes the part of a posterolateral corner of a knee. This is the deep muscle of a knee joint, forming the ground of a popliteus fossa.
- This also makes up a lateral musculature of a knee joint, along an iliotibial band. This is the only muscle in a posterior compartment of a lower leg (which also includes tibialis posterior, flexor digitorum longus, as well as flexor hallucis longus) that is mono-articular & does not influence the ankle joint.
- This is one of the main posterolateral stabilizers of a knee joint, causing both medial as well as lateral rotation of a knee, thereby being involved in both the closed chain phase & open-chain phase of a gait cycle. This also works as the smaller stabilizer in rregardingernal rotation anterior translation & varus force.
Anatomy
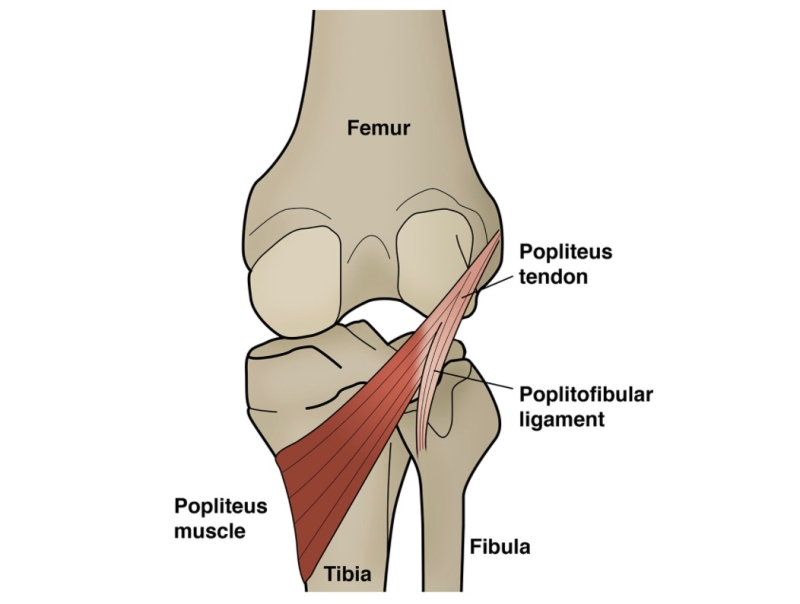
- Origin: The muscle fibers originate from a lateral condyle of a femur & a posterior horn of a lateral meniscus, via the strong tendon called a popliteus tendon. Cadaveric dissections have also shown fibers originating from a styloid portion of a fibular head, which then runs obliquely blending with the main muscular structure.
- From there it runs inferiorly as well as mediolaterally towards a Tibia. This courses diagonally across a posterior upper tibia & a portion of a joint capsule, to lie as the deepest muscle of a posterior knee region. A popliteal tendon pierces a joint capsule but does not enter the synovium. A popliteus tendon passes beneath a lateral collateral ligament (LCL) as well as a tendon of the biceps femoris.
- A popliteal bursa, which is usually the extension of a synovial membrane, separates it from a lateral femoral condyle. Even though a popliteus muscle has extra-articular areas, this is the capsular structure separating a lateral meniscus of a knee from a lateral collateral ligament. Furthermore, the head of the popliteus can arise from a sesamoid bone in a lateral head of a gastrocnemius muscle. Moreover, an inconstant muscle called a popliteus minor is seen which arises from a femur on an inner side of a plantaris muscle as well as inserts into a posterior ligament of a knee joint.
- A popliteus muscle is intra-capsular but extra-articular as well as extra-synovial.
- Insertion: The inserts on a tibia are just proximal to a soleal line but below the tibial condyles.
- Nerve supply: A popliteus muscle is supplied by a tibial nerve, from spinal nerve roots L4 through S1, with approximately 2 to 3 parallel tibial nerve branches. An entry point of a nerve is a lateral distal margin of a muscle, which is found inferior to a fibular head, as well as then splits into anterior, medial, as well as lateral distributions throughout a muscle.
- Blood supply: A popliteus muscle is supplied by two arteries two medial inferior genicular branches of a popliteal artery, and a muscular branch of a posterior tibial artery.
- Function:
- The popliteus muscle helps in knee flexion & its function is decided according to the position of the lower extremity, for instance, weight-bearing or even non-weight-bearing, as it is the primary internal rotator of a tibia in the non-weight-bearing position.
- In open chain kinematics, this rotates the tibia medially,
- In close chain kinematics, this laterally rotates the femur in the initial phase of the knee flexion.
- With extension while weight-bearing, ‘locking’ of a knee happens. In this state, a femur medially rotates on a tibia, allowing for the full extension without muscular expenditure. To ‘unlock’ the knee, a popliteus muscle requires to contract, causing flexion as well as lateral rotation of a femur on a tibia, thereby giving a muscle the term – ‘key’ to a locked knee.
- While the knee flexion, a popliteus muscle retracts a lateral meniscus posteriorly to avoid being entrapped between a femur as well as a tibia.
- In knee stability as the popliteus tendon is frequently found to be connected to the lateral capsule, it gives the muscle a possible role in the postero-lateral stability of the knee. The Popliteus is an important structure resisting excessive external tibial rotation as well as maintaining a neutral tibial rotation, even if all other postero-lateral ligaments were severed.
Clinical relevance
- It is commonly involved in the posterolateral (PCL) corner injuries of the knee, which occur secondary to a varus force applied to a flexed knee, a direct blow to the knee (from medial to lateral).
- Varus/hyperextension( both from contact and non-contact injuries).
- Dislocation of the knee.
Whatever the mechanism of injury to a posterior cruciate ligament corner (from the above), an urgent evaluation of a patient’s neurovascular status of a limb is performed. In the case of knee dislocation, vascular status is assessed followed by the closed reduction of a knee joint which is then again followed by assessing a vascular status. - Further to the trauma, poor motion patterns, as well as posture, may often weigh heavily on a popliteus muscle leaving it prone to weakness as well as injury. Iatrogenic injury to the muscle is common, which may lead to poor functional prognosis as well as thus becomes vital to be addressed – especially following the knee reconstruction surgery. Anatomical smaller knees also required extra attention as the risk of popliteal injury is increased.
- Popliteal tendinopathy may also happen as posterolateral knee pain. However, this can be difficult to single out owing to other more common knee pain etiologies in the vicinity. As the muscle inhibits excessive tibial rotation preventing significant anterior translation of a knee, this can be pathologically overcome secondary to excessive sprinting or even running downhill & thus such activities may be avoided or even modified to run on flat surfaces such as the treadmill.
- If lateral hamstrings are stronger as compared to the inner (medial) hamstrings, a popliteus muscle will be weaker. Excessive pronation or collapse of an inner foot when walking or even running will stress a popliteus in an opposite direction.
- Different EMG studies have shown that popliteus muscle activity increases with knee extension & downhill walking, thereby consolidating its role in the control of hyperextension of a knee joint.
- A referred pain pattern in the case of trigger point of popliteus muscle is the back of the knee.