
Capitate Bone
Table of Contents
Introduction
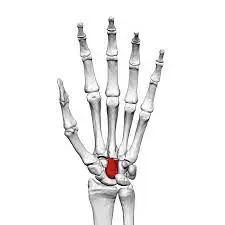
The Capitate bone is one of the eight carpal bones located in the wrist. It is the largest of the carpal bones and is situated in the middle of the second row, between the trapezoid bone and the hamate bone. The capitate bone is roughly cuboidal in shape, with a rounded head on its proximal end and a slightly tapered body that extends to its distal end.
The capitate bone has several important features that contribute to its function and stability in the wrist joint. The palmar surface of the capitate bone is smooth and convex, allowing for articulation with the trapezium bone. This articulation forms a plane joint, which permits gliding and sliding movements between the two bones.
Anatomy of Capitate Bone
The capitate bone is one of the eight carpal bones in the wrist and is the largest of the carpal bones. It is located in the middle of the second row of carpal bones, between the trapezoid bone and the hamate bone.
The capitate bone has a roughly cuboidal shape, with a rounded head on its proximal end and a slightly tapered body that extends to its distal end. The head of the capitate bone is covered in articular cartilage, which helps reduce friction and provides a smooth surface for joint movement.
The palmar surface of the capitate bone is smooth and convex, allowing for articulation with the trapezium bone. This articulation forms a plane joint, which permits gliding and sliding movements between the two bones. The palmar tubercle, a roughened area on the palmar surface, serves as an attachment site for ligaments and tendons.
On the dorsal side of the capitate bone, there is a ridge called the dorsum. The dorsum serves as an attachment site for ligaments and tendons that help stabilize the wrist joint. It also provides a bony prominence that can be palpated on the back of the hand.
The capitate bone has several important ligamentous attachments. The dorsal ligaments attach to the dorsum of the capitate bone, helping to stabilize the wrist joint. The palmar ligaments attach to the palmar tubercle, providing additional stability.
The capitate bone plays a crucial role in wrist movement and stability. It acts as a central pillar within the wrist joint, transmitting forces from the hand to the forearm. It helps distribute weight-bearing forces during activities such as gripping, grasping, and lifting. Additionally, the capitate bone assists in maintaining proper alignment and positioning of the other carpal bones, contributing to overall wrist stability.
The capitate bone is a large carpal bone located in the wrist. Its anatomy includes a rounded head, a slightly tapered body, and important ligamentous attachments. It articulates with the trapezium bone to form a plane joint, allowing for gliding and sliding movements. The capitate bone provides stability and function to the wrist by acting as a central pillar, distributing forces, and maintaining proper alignment of the carpal bones.
Articulation of Capitate Bone
The articulation of the capitate bone involves its connection with neighboring bones in the wrist, specifically the trapezoid bone and the hamate bone.
The capitate bone forms a joint with the trapezoid bone, known as the capitate-trapezoid joint. This joint is located on the palmar side of the wrist and is classified as a plane joint. A plane joint is a type of synovial joint in which the articulating surfaces are flat or slightly curved, allowing for gliding and sliding movements between the bones.
The head of the capitate bone, which is covered in articular cartilage, articulates with the corresponding surface of the trapezoid bone. The articular cartilage provides a smooth surface for joint movement and helps reduce friction during motion.
The capitate bone also articulates with the hamate bone, forming the capitate-hamate joint. This joint is located on the palmar side of the wrist, slightly distal to the capitate-trapezoid joint. The articulation between the capitate and hamate bones is a saddle joint.
A saddle joint is a type of synovial joint in which the articulating surfaces have both convex and concave regions, resembling the shape of a saddle. This allows for a greater range of motion compared to a plane joint. The saddle-shaped surface of the hamate bone fits into the corresponding surface of the capitate bone, creating a stable but mobile joint.
The articulations of the capitate bone with the trapezoid and hamate bones allow for various movements of the wrist. These movements include flexion and extension (bending and straightening), radial and ulnar deviation (movement towards and away from the thumb), as well as circumduction (circular motion).
Muscle attachment
The capitate bone may be a central bone within the wrist that serves as a connection site for a few muscles. These muscle connections play a vital part in the development and solidness of the wrist joint.
On the dorsal (back) side of the capitate bone, there are a few muscle connections. The extensor carpi radialis longus muscle connects to the dorsal surface of the capitate bone by means of a ligament. This muscle is capable of amplifying and snatching the wrist joint, permitting developments such as lifting the hand upwards and moving it towards the thumb side.
The extensor carpi radialis brevis muscle moreover incorporates a ligament that joins to the dorsal surface of the capitate bone. This muscle helps in amplifying and stealing the wrist, but it is primarily involved in flexion (bowing) and snatching (moving absent from the midline) of the thumb.
Furthermore, the extensor carpi ulnaris muscle encompasses a ligament that joins to the dorsal surface of the capitate bone. This muscle is mindful of expanding and adducting the wrist, permitting for developments such as moving the hand downwards and towards the small finger side.
On the palmar (front) side of the capitate bone, there are moreover muscle connections. The flexor carpi radialis muscle incorporates a ligament that joins to the palmar surface of the capitate bone. This muscle is included in flexion and kidnapping of the wrist, permitting for developments such as bowing the hand downwards and moving it towards the thumb side.
The flexor carpi ulnaris muscle moreover features a ligament that joins to the palmar surface of the capitate bone. This muscle helps in flexion and adduction (moving towards the midline) of the wrist, permitting for developments such as bowing the hand downwards and towards the small finger side.
In expansion to these specific muscle connections, other muscles within the lower arm contribute to the development and soundness of the capitate bone. These muscles incorporate the flexor digitorum superficialis, flexor digitorum profundus, and interosseous muscles.
Generally, the muscle connections of the capitate bone play a significant part in the facilitated development and solidness of the wrist joint. They permit different activities such as flexion, expansion, kidnapping, and adduction of the wrist, as well as developments of the thumb and fingers.
Blood and lymph supply
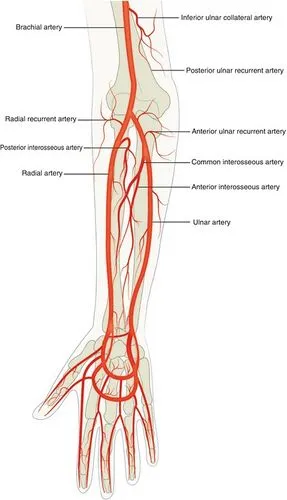
The capitate bone, found within the wrist, gets its blood supply from numerous sources. The essential blood supply to the capitate bone comes from branches of the spiral supply route, particularly the dorsal carpal department and the back interosseous supply route. These courses enter the capitate bone through little supplement foramina, which are openings within the bone that permit blood vessels to enter and supply supplements.
In expansion to the outspread supply route, the capitate bone too gets blood supply from the ulnar supply route through a little department known as the front interosseous course. This course contributes to the blood flow to the capitate bone, in spite of the fact that it isn’t as critical as the outspread course.
The lymphatic supply of the capitate bone is the portion of the lymphatic framework, which makes a difference drain excess liquid and squander items from tissues. The lymphatic vessels within the wrist locale deplete into lymph hubs found within the axilla (armpit) and the cubital fossa (the zone on the front of the elbow). From there, lymphatic vessels proceed to deplete into bigger lymphatic vessels and inevitably into the lymphatic channels, which return lymph liquid back into the circulatory system.
It is vital to note that while the blood and lymphatic supply are pivotal for keeping up the well-being and work of the capitate bone, they don’t straightforwardly take part in the recovery preparation of hamate bone harm. Recovery essentially centers on reestablishing the extent of movement, quality, and work through works out and slow movement of exercises.
Functions of the Capitate Bone
The capitate bone, located in the wrist, serves several important functions in the human body.
- Support and Stability: The capitate bone is one of the largest bones in the wrist and plays a crucial role in providing support and stability to the wrist joint. It acts as a central pillar, connecting the bones of the wrist and hand, and helps maintain the overall structure and alignment of the wrist.
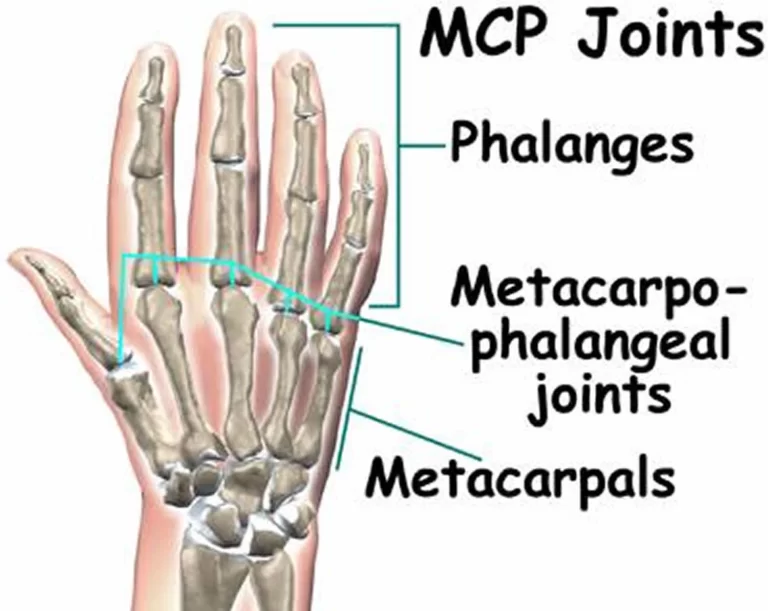
- Articulation: The capitate bone forms important articulations with adjacent bones, including the scaphoid bone proximally and the metacarpal bones distally. These joints allow for smooth and coordinated movements of the wrist and hand.
- Load Transmission: As a weight-bearing bone, the capitate bone helps transmit forces from the forearm to the hand during activities such as gripping, lifting, and pushing. It helps distribute these forces evenly across the wrist joint, reducing the risk of injury and ensuring efficient movement.
- Range of Motion: The capitate bone, along with other wrist bones, contributes to the overall range of motion of the wrist joint. It allows for flexion, extension, abduction, adduction, and circumduction movements of the wrist, enabling various functional activities of the hand.
- Muscle Attachment: Several muscles in the forearm and hand attach to the capitate bone via tendons. These muscles play a vital role in controlling movement and providing strength to the wrist and hand. The attachment of these muscles to the capitate bone allows for coordinated muscle contractions and precise control of finger and wrist movements.
- Proprioception: The capitate bone contains numerous sensory receptors that provide feedback to the brain about the position and movement of the wrist joint. This proprioceptive feedback helps in maintaining balance, coordination, and precision during fine motor tasks.
Overall, the capitate bone is essential for maintaining the stability, range of motion, and strength of the wrist joint. Its proper functioning is crucial for performing daily activities, such as writing, typing, grasping objects, and participating in sports or recreational activities.
Conditions that affect Capitate Bone
Associated conditions of the capitate bone can include fractures, dislocations, and degenerative conditions such as osteoarthritis.
Fractures: Fractures of the capitate bone can occur due to traumatic injuries, such as falls or direct impact on the wrist. These fractures can vary in severity, ranging from hairline fractures to complete breaks. Symptoms of a capitate fracture may include pain, swelling, tenderness, and difficulty moving the wrist. Treatment typically includes immobilization with a cast or splint, and in some conditions, surgical treatment may be needed to realign and stabilize the bone.
Dislocations: Dislocation of the capitate bone can happen when it is forcefully pushed out of its normal position within the wrist joint. This can occur due to high-impact injuries or excessive force applied to the wrist. Dislocation of the capitate bone can cause severe pain, swelling, deformity, and limited range of motion in the wrist. Treatment usually involves immediate medical attention to relocate the bone back into its proper position, followed by immobilization and rehabilitation.
Osteoarthritis: Osteoarthritis is a degenerative condition that can affect any joint in the body, including the wrist joint where the capitate bone is located. Over time, the cartilage that cushions the joint surfaces may wear away, leading to pain, stiffness, swelling, and reduced range of motion. Osteoarthritis of the capitate bone can be caused by age-related wear and tear, previous injuries, or repetitive stress on the joint. Treatment options for osteoarthritis may include pain management, physical therapy, splinting or bracing, and in severe cases, surgery.
It is very necessary to take in mind that any condition affecting the capitate bone should be evaluated and treated by a medical professional specializing in orthopedics or hand surgery. They can provide a proper diagnosis, recommend appropriate treatment options, and guide rehabilitation to ensure optimal recovery and function of the wrist joint.
Rehabilitation
Rehabilitation of the capitate bone involves a comprehensive treatment plan aimed at restoring function, reducing pain, and promoting healing. The specific rehabilitation program will depend on the underlying condition or injury affecting the capitate bone, as well as the individual’s overall health and goals.
Fractures: In cases of capitate bone fractures, rehabilitation typically begins after the initial immobilization period with a cast or splint. The rehabilitation program may include:

- Pain management: Medications or modalities such as ice or heat therapy may be used to manage pain and reduce inflammation.
- Range of motion exercises: Gentle exercises and movements are gradually introduced to restore flexibility and mobility in the wrist joint. These may include wrist rotations, finger stretches, and gentle flexion and extension exercises.
- Strengthening exercises: As healing progresses, strengthening exercises are incorporated to improve muscle strength and stability around the wrist joint. This may involve using resistance bands or hand weights to perform wrist curls, grip exercises, and forearm exercises.
- Functional activities: As strength and mobility improve, functional activities specific to the individual’s daily tasks or work requirements may be incorporated into the rehabilitation program. This could include activities such as gripping objects, writing, or using tools.
- Gradual return to activities: The rehabilitation program will gradually progress to include more challenging activities and tasks, with the goal of returning to normal or near-normal function.
Dislocations: Rehabilitation following a capitate bone dislocation focuses on restoring stability, range of motion, and strength in the wrist joint. The rehabilitation program may include:
- Reduction and immobilization: Immediate medical attention is required to relocate the dislocated bone back into its proper position. Following reduction, the wrist may be immobilized with a splint or cast for a period of time to allow for healing.
- Pain management: Similar to fractures, pain management techniques may be used to alleviate discomfort during the rehabilitation process.
- Range of motion exercises: Gentle range of motion exercises are gradually introduced to restore flexibility and mobility in the wrist joint. These exercises may include wrist rotations, finger stretches, and gentle flexion and extension exercises.
- Strengthening exercises: As healing progresses, strengthening exercises are incorporated to improve muscle strength and stability around the wrist joint. This may involve using resistance bands or hand weights to perform wrist curls, grip exercises, and forearm exercises.
- Functional activities: Functional activities specific to the individual’s daily tasks or work requirements are gradually introduced to simulate real-life movements and tasks.
- Gradual return to activities: The rehabilitation program will progress to include more challenging activities and tasks, with the goal of returning to normal or near-normal function.
Osteoarthritis: Rehabilitation for osteoarthritis of the capitate bone focuses on pain management, improving joint mobility, and preserving function. The rehabilitation program may include:
- Pain management: Various techniques such as heat or cold therapy, medication, or injections may be used to manage pain and reduce inflammation.
- Range of motion exercises: Gentle range of motion exercises are performed to maintain or improve joint mobility. These exercises may include wrist rotations, finger stretches, and gentle flexion and extension exercises.
- Strengthening exercises: Strengthening exercises are incorporated to improve muscle strength and stability around the wrist joint. This may involve using resistance bands or hand weights to perform wrist curls, grip exercises, and forearm exercises.
- Splinting or bracing: In some cases, splints or braces may be recommended to provide support and reduce stress on the affected joint.
- Assistive devices: Depending on the individual’s needs, assistive devices such as adaptive utensils or tools may be recommended to aid in daily activities.
- Pain management techniques: Modalities such as heat or cold therapy, ultrasound, or transcutaneous electrical nerve stimulation (TENS) may be used to manage pain and reduce inflammation.
- Education and lifestyle modifications: Individuals may be provided with education on joint protection techniques, ergonomic modifications, and lifestyle changes to minimize stress on the wrist joint and improve overall joint health.
It is necessary to consult with a medical professional specializing in orthopedics or hand surgery for a personalized rehabilitation program tailored to your specific condition and needs. They can provide guidance, monitor progress, and make necessary adjustments to ensure optimal recovery and function of the capitate bone and wrist joint.
FAQs
The duration of rehabilitation for the capitate bone will vary depending on the severity of the condition or injury, as well as individual factors such as overall health and adherence to the rehabilitation program. Rehabilitation can take time from some weeks to several months.
Rehabilitation alone cannot heal a fractured capitate bone. Fractures typically require medical intervention such as casting, splinting, or surgery to realign and stabilize the bone. Rehabilitation is then used to restore function, reduce pain, and promote healing after the initial immobilization period.
Rehabilitation can help improve muscle strength, joint stability, and overall function, which may reduce the risk of future fractures or dislocations of the capitate bone. However, it cannot guarantee prevention as there are other factors that can contribute to these injuries, such as trauma or underlying conditions.

One Comment