
Subtalar Joint
Table of Contents
Introduction
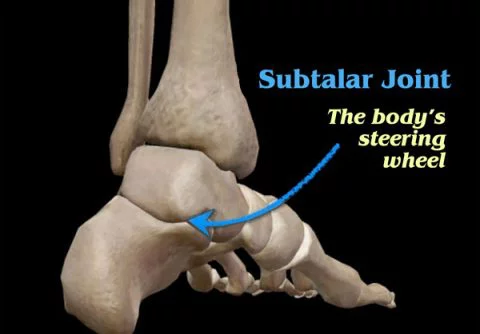
The Subtalar joint, also known as the talocalcaneal joint, is a significant joint in the foot that plays a crucial role in foot and ankle movement. It is formed by the articulation between the talus bone, located above, and the calcaneus bone, situated below. As a synovial joint, it allows for smooth gliding and controlled motion.
This joint is also known as the anatomical subtalar joint or the subtalar joint proper in the literature.
However, in clinical practice, the anatomical subtalar (posterior) and talocalcaneonavicular (anterior) joints are considered functional units. The acuminate interosseous tunnel, which is involved in the tarsal canal and tarsal sinus, is located in the center of this functional area.
The anatomical subtalar joint is a single synovial articulation created by the talus’s posterior calcaneal articular aspect and the calcaneus’s convex posterior articular surface. Capsules, ligaments, and interosseous connections connect bones.
Two principal synthesis movements happen in this joint; supination and pronation. Joints, ligaments, and tendinous tissue have significant movements.
Inversion and eversion allow:
- The foot and ankle to pivot/change directions,
- and stay balanced
- walking across uneven terrain.
- act as a shock absorber.
Pathology
The subtalar joint is mostly exposed to arthritis, especially as it has previously been affected by sprains or fractures such as those of the calcaneum or talus. Symptoms of subtalar joint arthritis involve pain in walking, loss of movement through the joint’s range of motion, and difficulty walking on rough surfaces. In flat feet, the joint is generally more horizontal.
Biomechanics
Subtalar joint movement and rotation axis are complex due to the convex posterior aspect of the calcaneus and talus. Manter described a circular movement, with a 1.5 mm talus advance for every 10° rotation. Inman’s skeleton study showed screw-like movement, translation, or rotation. The axis of subtalar joint movement has high flexibility, possibly due to the method used, including static radiographic images and in vivo studies.
Subtalar joint movement is restricted as inversion-eversion, with a range of 25°-30° in inversion and 5°-10° in eversion. High variability in range could be clarified by different techniques and ankle joint position.
Tendons balance the ankle during the gait and stance phases, with evertors and invertors involving the tibialis posterior and peroneus longus, depending on the subtalar joint position.
Anatomy
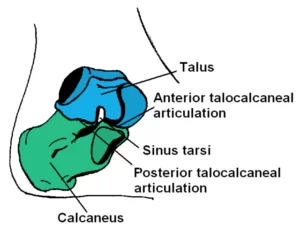
The subtalar joint includes two parts: the anterior and posterior parts. The anterior talar head is on the calcaneus anterior and middle aspect, supporting the acetabulum pedis and navicular bone. The spring ligament plays a critical role in stabilizing the talar head, which can lead to flat foot deformity. The posterior talus surface is larger and separated by the interosseous calcaneal ligament. Anatomical variations exist for the anterior and middle surface, with 42% having an oblong form, 22% a ‘bean’ form, and 36% having a complete separation.
The subtalar joint is damaged by intrinsic and extrinsic ligaments, including the cervical ligament and interosseous talocalcaneal ligament. Malfunction of the interosseous ligament can cause unnatural anterolateral rotation, main to instability. The importance of the calcaneofibular ligament for subtalar stabilization is different, but studies show increased subtalar movement and instability. The inferior extensor retinaculum also recreates a role in subtalar joint stability and movement.
Structure
The ST joint is a multi-articular joint, with three articulated aspects that provide a surface for the joint to glide. The ST joint could be divided into two parts:
On the anterior surface of the calcaneus, the talus is positioned slightly obliquely.
Between the two bones, there are three places of articulation: two anterior and one posterior. The posterior, middle, and anterior facets are the three articulations, which are together referred to as facets.
- The anterior subtalar joint: talar head articulating with the anterior and middle surface of the calcaneus. Which allows gliding forward (anterior articulation).
- The medial subtalar joint: Allows the joint to glide side-to-side.
- The posterior subtalar joint: the concave surface of the talus lies on the convex posterior aspect of the calcaneus. Which tolerates gliding backward (posterior articulation).
The anterior facet articulates with the head of the talus and lies laterally and congruently to the middle facet, with the sustain tenaculum tali forming the floor of the middle facet. Some persons only have one articulation because the middle and anterior facets are connected. The tarsal canal divides the three facet bones into their largest and greatest-sized counterparts, respectively.
Location
Each foot has seven tarsal bones, which form the heel, ankle, and hindfoot framework. The proximal tarsal bones, talus, and calcaneus are closest to the ankle. The calcaneus bone, the largest and strongest, attaches to the Achilles tendon.
The talus, the superior tarsal bone, connects the ankle to the tibia. It is stacked above the front part of the calcaneus bone, with three subtalar facets in the groove. The interosseous talocalcaneal ligament links the talus and calcaneus bone.
Stability
The subtalar joint contains a capsule, synovial membrane, fibrous layer, and three ligaments.
- Posterior talocalcaneal ligament
- Medial talocalcaneal ligament
- Lateral talocalcaneal ligament
The interosseous talocalcaneal ligament secures the talus and calcaneus, providing stability and strength in the sinus tarsi cavity.
Articular surfaces
The anatomical subtalar joint is a synovial articulation connecting the talus and calcaneus. It consists of two articular aspects lined with hyaline cartilage.
The articular surfaces that include this joint involve the concave posterior calcaneal aspect on the inferior surface of the talus and the convex posterior talar articular surface on the superior aspect of the calcaneus.
Ligaments and joint capsule
The subtalar joint has one relaxed joint capsule that covers the whole joint. Like in other synovial joints, the joint capsule is filled with a synovial membrane. The lateral, medial, and posterior freezing of the joint capsule are the main ligaments that share in the movements of this joint. The subtalar joint capsule connects to articular surfaces, the tarsal sinus floor, and the roof. The tarsal sinus is a narrow passageway located directly anterior to the subtalar joint, connecting the talus and calcaneus.
Inside the tarsal sinus, the joint capsules of the subtalar and talocalcaneonavicular joints connect and shape the talocalcaneal interosseous ligament.
The lateral talocalcaneal ligament is a flat fibrous group that length obliquely connecting the lateral talar process to the lateral calcaneal surface and the calcaneofibular ligament. It lies deep in the calcaneofibular ligament.
The medial talocalcaneal ligament length connects the medial aspects of the talar tubercle and calcaneus and the posterior aspect of sustained tenaculum tali. Some of its distal sarcophagi merge with the medial deltoid ligament of the ankle joint.
The posterior talocalcaneal ligament is fibrous tissue connecting the talus to the calcaneus. The interosseous talocalcaneal ligament is collected from two dense and thick fibrous groups located in the tarsal sinus. The deep extension of the inferior extensor retinaculum is situated joining this group of the interosseous ligament.
Occupying the central position joining the talocalcaneal and talocalcaneonavicular joints, this ligament is related to the functions of both joints. The main role of this ligament in the subtalar joint is to maintain stability both at rest and by active movements. Interosseous talocalcaneal ligament inflexible, restricting foot movement.
The cervical/anterior talocalcaneal ligament is detected lateral to the ligament and the tarsal sinus. Development from superior calcaneal surface to talar neck tubercle. This ligament is also rigid in pronation.
Innervation
The plantar surface of the subtalar joint is innervated by the medial or lateral plantar nerves, while the dorsal aspect takes its innervation from the deep fibular nerve.
Neurovascular Supply
The subtalar joint takes supply from two arteries and two nerves. Arterial supply approaches from the posterior tibial and fibular arteries.
Innervation to the plantar part of the joint is supplied by the medial or lateral plantar nerve, whereas the dorsal surface of the joint is supplied by the deep fibular nerve.
Blood supply
Arterial supply provides for the subtalar joint to enter from two arteries; the Posterior tibial artery and the fibular artery.
Function
The joint tolerates inversion and eversion of the foot but recreates a minimal role in dorsiflexion or plantarflexion of the foot. The center of rotation of the subtalar joint is thought to be in the region of the middle aspect.
It is considered a plane synovial joint, also commonly mentioned as a gliding joint. It acts as a depend connecting the talus and calcaneus. There is an extensive change in the inclination from horizontal.
The subtalar joint can also be considered a combination of the anatomic subtalar joint thought above, and further the talocalcaneal part of the talocalcaneonavicular joint. This is the more usual view of the subtalar joint as considers its movement. Joint articulations enable midfoot pronation and supination.
Movement
Subtalar joint movements involve gliding and rotation, causing pronation and supination. Primary movements are talocalcaneonavicular and calcaneocuboid joints, creating a functional part of the foot.
Supination and pronation be on a single axis from calcaneus tubercle to talus neck, with an average rotation angle of 42° upwards and anterior to the transverse plane.
Supination involves inversion, adduction, and plantarflexion at joints, while pronation develops from eversion, abduction, and dorsiflexion. Primary movements should be coincidental and never in isolation.
Inversion and eversion are primary movements in subtalar and transverse tarsal joints, with ranges different across origin, with inversion ranging from 25° to 30° and eversion from 5° to 10°.
Inversion and eversion are movements where the sole of the foot rotates towards the midline and the lateral side is directed inferiorly. Abduction and adduction be around a vertical axis in the transverse plane. The range of motion for adduction/abduction is similar to inversion/eversion but depends on the interindividual intention of the axis of rotation. An inclination less than 42° results in greater RoM for inversion/eversion and less adduction/abduction, while the opposite happens closer to the long axis of the leg.
Dorsiflexion and plantarflexion of subtalar and transverse tarsal joints are minor parallel to inversion/eversion and abduction/adduction movements, with a closed packed position and limited ROM in varus and valgus.
Muscles acting on the subtalar joint
Subtalar joint suspension involves tibialis anterior, posterior, and support from hallucis longus.
Pronation is mainly produced by fibularis longus, fibularis brevis, and fibularis tertius with help from the extrinsic muscles that extend the toes (extensor digitorim logus and extensor hallucis longus).
Clinical Significance
Problems affecting the subtalar joint can arise from injuries, such as sprains or fractures, as well as conditions like arthritis or instability. Subtalar joint disorders can lead to pain, limited mobility, and difficulties with walking or running. Treatment options may include conservative measures like rest, physical therapy, orthotics, or, in severe cases, surgical intervention.
It’s important to consult with a healthcare professional or a qualified orthopedic specialist for an accurate diagnosis and appropriate management of any subtalar joint-related issues.
Sinus tarsi syndrome is a painful condition affecting athletes, causing persistent ankle discomfort and subtalar joint synovitis. Diagnosis is determined through physical examination, with treatment involving physical therapy and anti-inflammatory medication.
Summary
The subtalar joint connects tarsal bones in the hindfoot, consisting of the talus bone and calcaneus bone, forming the heel.
The subtalar joint’s primary need is to facilitate gait movements. Because of the faithful and repeated stress placed on it, it could be prone to acute traumatic injuries, like subtalar dislocation, as do chronic conditions that progress from wear-and-tear, like osteoarthritis.
Clinical relations
FAQS
The subtalar joint, also known as talocalcaneal, is a foot joint involving the talus and calcaneus.
below the talus (= the ankle bone): the subtalar joint.
The talus and calcaneus, two of the tarsal bones in the foot, are joined together at the subtalar (ST) joint. The St joint, which allows for foot rotation, inversion, and eversion, is a synovial joint.
The subtalar joint is anatomically related to the talus and calcaneus, also known as the anatomical subtalar joint.
Sustentaculum tali form the mid-calcaneal aspect, supporting tibialis posterior, hallucis longus, and digitorum longus tendons.
Subtalar joint supplies arteries and nerves, with arteries providing anterior and fibular blood supply, and nerves innervating plantar and dorsal aspects.
Peroneus longus, brevis, and Tertius are lateral ankle stabilizers and primary investors, crucial for pronator and supinator motion.
STJoint neutral position is used by clinicians for cast representations in a biomechanical functional orthosis, but no method is accurate or reproducible.
Sustentaculum tali, middle calcaneal aspect, supports tibialis posterior, hallucis longus, and digitorum longus tendons.
Sprains: These wounds result in ligament tears or stretching. Strains: These wounds result in strained or torn muscles or tendons. Fractures: The AAOS states that pain in the subtalar joint is a symptom of a broken talus bone. Dislocation: This injury include bones popping or slipping out of sequence.
10 Comments