

Hamate Bone
Table of Contents
Introduction
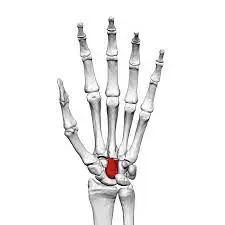
The Hamate bone, also known as os hamatum, is one of the eight carpal bones located in the wrist. It is situated on the ulnar side of the wrist, which is the side closer to the pinky finger. The bone is named after its hook-like process called the hamulus, which protrudes from the palm side of the bone.
The hamate bone has several important anatomical features. It has a body, which is the main portion of the bone, and a hook-like process that extends toward the palm. The body of the hamate bone forms part of the carpal tunnel, a narrow passageway in the wrist through which several tendons and the median nerve pass. The hook of the hamate bone serves as an attachment site for various ligaments and muscles.
Anatomy of the Hamate Bone
The hamate bone is one of the eight carpal bones present in the wrist. It is a wedge-shaped bone that sits on the ulnar side of the wrist, towards the pinky finger. The hamate bone consists of a body and a hook.
The body of the hamate bone is the larger part and forms the majority of its structure. It has a curved shape with a smooth surface, which contributes to the articulation and movement of adjacent bones. The body of the hamate bone also has several prominent features, including a ridge called the crest, which serves as an attachment site for ligaments and muscles.
The hook of the hamate bone is a bony projection that extends from the body towards the palm side of the hand. It is located on the medial side of the bone and is easily palpable. The hook is curved and has a sharp tip, resembling a hook or a beak. This hook serves as an attachment site for various ligaments and muscles, including the flexor retinaculum, flexor carpi ulnaris tendon, and abductor digiti minimi muscle.
The hamate bone is connected to other carpal bones through ligaments, forming a stable and flexible wrist joint. It articulates with the capitate bone proximally, the fourth and fifth metacarpal bones distally, and the triquetrum bone medially.
Functions of the Hamate Bone
The hamate bone serves several important functions in the wrist and hand.
- Support and stability: The hamate bone, along with the other carpal bones, provides support and stability to the wrist joint. It helps maintain the alignment of the wrist and allows for smooth movements of the hand and fingers.
- Attachment site for ligaments and muscles: The hook of the hamate bone serves as an attachment site for various ligaments and muscles. Ligaments are tough bands of connective tissue that connect bones to other bones, while muscles are responsible for movement. The attachment of ligaments and muscles to the hamate bone helps provide strength and control during gripping and wrist movements.
- Carpal tunnel formation: The body of the hamate bone contributes to the formation of the carpal tunnel, a narrow passageway in the wrist. The carpal tunnel houses several tendons that control finger motion and the median nerve, which give sensation to the palm and fingers. The hamate bone helps form the floor of the carpal tunnel, providing protection and support to these structures.
- Transfer of forces: The hamate bone plays a role in transferring forces from the forearm to the hand. When we grip or perform activities that involve the use of our hands, forces generated by the muscles in the forearm are transmitted through the wrist and ultimately to the hand. The hamate bone helps distribute these forces evenly, allowing for efficient and controlled hand movements.
Overall, the hamate bone is an integral part of the wrist and hand complex, contributing to its stability, strength, and functionality.
Articulation of the Hamate Bone
The articulation of the hamate bone involves its connection with several other bones and structures in the hand and wrist. These articulations allow for various movements and provide stability to the hand.
- Ulna: The hamate bone articulates with the ulna at the distal radioulnar joint. This joint provides for forearm rotation, which is necessary for actions such as twisting a doorknob or using a screwdriver.
- Capitate: The hamate bone articulates with the capitate bone at the carpometacarpal joint of the little finger. This joint allows for flexion (bending), extension (straightening), abduction (moving away from the midline), and adduction (moving towards the midline) movements of the little finger. These movements are important for activities such as typing, playing musical instruments, or gripping small objects.
- Triquetrum: The hamate bone also articulates with the triquetrum bone at the pisohamate joint. This small synovial joint allows for slight gliding movements between the two bones. Although the range of motion at this joint is limited, it contributes to the overall flexibility and mobility of the wrist.
- Metacarpals: The hamate bone has a hook-like projection called the hamulus, which articulates with the fourth and fifth metacarpal bones at the carpometacarpal joint of the ring and little fingers. This joint allows for flexion, extension, abduction, and adduction movements of these fingers. These movements are crucial for tasks that require a strong grip, such as holding a pen or lifting weights.
Overall, the articulation of the hamate bone plays a vital role in hand and wrist movements. It allows for rotation of the forearm, flexion and extension of the little finger, slight gliding movements between the hamate and triquetrum bones, and flexion, extension, abduction, and adduction movements of the ring and little fingers. These movements are essential for various daily activities and tasks that involve the use of the hand and wrist. Additionally, the articulation of the hamate bone provides stability and support to the hand, helping to transmit forces from the forearm to the hand.
Muscle attachment
The hamate bone serves as an attachment site for several muscles in the hand and wrist. These muscle attachments play a crucial role in the movement and stability of the hand.
- Flexor Digiti Minimi: The flexor digiti minimi muscle originates from the hamate bone. It is responsible for the flexion (bending) of the little finger at the metacarpophalangeal joint and assists in the flexion of the proximal and distal interphalangeal joints. This muscle provides strength and control to the little finger during gripping and fine motor activities.
- Opponens Digiti Minimi: The opponens digiti minimi muscle also originates from the hamate bone. It is responsible for the opposition of the little finger, which is the movement that brings the little finger toward the thumb. This muscle allows for precision grip and manipulation of objects between the thumb and little finger.
- Flexor Carpi Ulnaris: The flexor carpi ulnaris muscle has a tendon that passes over the hook of the hamate bone. This muscle originates from the medial epicondyle of the humerus and inserts into the pisiform bone and base of the fifth metacarpal bone. It is responsible for flexion and adduction of the wrist, as well as assisting in ulnar deviation (moving the hand towards the little finger side). The attachment of this muscle to the hamate bone helps stabilize the wrist joint during these movements.
- Abductor Digiti Minimi: The abductor digiti minimi muscle also has a tendon that passes over the hook of the hamate bone. This muscle arises from the pisiform bone and inserts into the bottom of the proximal phalanx of the little finger. It is responsible for the abduction (moving away from the midline) of the little finger. This muscle contributes to the spreading and separation of the fingers.
- Flexor Retinaculum: The hamate bone is also involved in the attachment of the flexor retinaculum, a thick band of connective tissue that forms the roof of the carpal tunnel. The flexor retinaculum helps hold the tendons of the flexor muscles in place and prevents them from bowstringing during finger and wrist movements.
In conclusion, the muscle attachments of the hamate bone are essential for the movement and stability of the hand and wrist. These muscles allow for flexion, opposition, abduction, and adduction of the little finger, as well as flexion, adduction, and ulnar deviation of the wrist. The attachment of these muscles to the hamate bone provides strength, control, and support to the hand during various activities and tasks.
Blood and lymph supply
The hamate bone receives its blood supply from several arteries, including the dorsal carpal branch of the ulnar artery, the palmar carpal branch of the ulnar artery, and the anterior interosseous artery.
The dorsal carpal branch of the ulnar artery is a major source of blood supply to the hamate bone. It arises from the ulnar artery and runs along the dorsal surface of the hand, supplying blood to the dorsal aspect of the hamate bone.
The palmar carpal branch of the ulnar artery also contributes to the blood supply of the hamate bone. It arises from the ulnar artery and passes through the palm of the hand, giving off branches that supply the palmar aspect of the hamate bone.
The anterior interosseous artery, a branch of the ulnar artery, provides additional blood supply to the hamate bone. It travels along the anterior surface of the interosseous membrane between the radius and ulna and sends branches to the volar (palm) aspect of the hamate bone.
In addition to arterial supply, the hamate bone also receives lymphatic drainage. Lymphatic vessels drain excess fluid and waste products from tissues and return them to the bloodstream. The lymphatic vessels in the hand and wrist region drain into lymph nodes located in the axilla (armpit) and cubital fossa (elbow pit). From there, lymphatic vessels continue to larger lymphatic trunks and eventually join the venous system.
Overall, the hamate bone receives a rich blood supply from various arteries, ensuring adequate oxygen and nutrient delivery to maintain its function and health. Lymphatic drainage helps remove waste products and maintain tissue fluid balance in the hand and wrist region.
Conditions that affect Hamate Bone
There are several associated conditions that can affect the hamate bone. These conditions can range from fractures and dislocations to specific injuries related to the hook of the hamate bone.
Hamate Fracture: A fracture of the hamate bone can occur due to direct trauma, such as a fall or a sports-related injury. Fractures can also be caused by repetitive stress on the bone, commonly seen in athletes who use tools with handles, such as golfers or baseball players. Symptoms of a hamate fracture include pain, swelling, tenderness, and difficulty gripping or grasping objects. Treatment typically involves immobilization with a cast or splint, and in some cases, surgical intervention may be necessary to realign and stabilize the bone.
Hamate Dislocation: Dislocation of the hamate bone can occur when there is a forceful twisting or bending of the wrist. This might occur as a result of activities such as sports or accidents. Symptoms of a dislocated hamate bone include severe pain, visible deformity, swelling, and limited range of motion in the wrist and hand. Immediate medical attention is required to relocate the bone and stabilize it with a splint or cast. In some cases, surgery may be necessary to repair any ligament damage or realign the bone.

Hamate Hook Fracture: The hook of the hamate bone is particularly susceptible to injury due to its prominent location and its exposure to external forces. Fractures of the hamate hook can occur from direct impact or repetitive stress on the bone. Symptoms include localized pain, tenderness, swelling, and difficulty gripping or grasping objects. Treatment options may include immobilization with a cast or splint, and in some cases, surgical removal of the fractured hook may be necessary.
Hamate Avulsion Fracture: An avulsion fracture occurs when a ligament or tendon attached to a bone pulls away a small piece of the bone. In the case of the hamate bone, an avulsion fracture can happen when the flexor carpi ulnaris tendon or other adjacent ligaments forcefully contract or tear away from the bone. Symptoms include pain, swelling, and limited wrist and hand function. Treatment may involve immobilization, physical therapy, and in severe cases, surgical intervention to reattach the fractured fragment.
Hamate Bone Contusion: A contusion, or bruise, of the hamate bone, can occur from direct trauma to the wrist or hand. This can cause swelling, pain, and tenderness in the affected area. Treatment typically involves rest, ice, compression, and elevation (RICE), along with over-the-counter pain medications to manage symptoms.
It is necessary to notice that these associated conditions can vary in severity and treatment options. Proper diagnosis by a medical professional is crucial for determining the appropriate course of treatment for each individual case.
Rehabilitation
Rehabilitation of a hamate bone injury typically involves a multi-step process that focuses on reducing pain, restoring range of motion, improving strength, and gradually returning to normal activities. The specific rehabilitation program may vary depending on the severity and type of injury, as well as individual factors such as age, overall health, and activity level. It is essential to consult with a healthcare professional or physical therapist for personalized guidance and supervision throughout the rehabilitation process.
- Immobilization: In cases of fractures or dislocations, immobilization is often the initial step in the rehabilitation process. This typically involves wearing a cast, splint, or brace to stabilize the injured area and promote proper healing. The duration of immobilization may vary depending on the extent of the injury but can range from a few weeks to several months.
- Pain management: Pain and inflammation are common after a hamate bone injury. Pain management techniques may include the use of over-the-counter or prescribed pain medications, cold therapy (applying ice packs to the affected area), and elevation to reduce swelling. Your healthcare provider may also recommend non-pharmacological pain management techniques such as transcutaneous electrical nerve stimulation (TENS) or ultrasound therapy.
- Range of motion exercises: Once the initial pain and swelling have subsided, gentle range of motion exercises can be initiated to restore flexibility and mobility in the wrist and hand. These exercises may include wrist flexion and extension, wrist circumduction (rotating the wrist in a circular motion), finger flexion and extension, and thumb movements. It is important to start with gentle movements and gradually increase the intensity and range of motion as tolerated.
- Strengthening exercises: As the range of motion improves, strengthening exercises can be introduced to rebuild muscle strength and stability in the wrist and hand. These exercises may include grip strengthening exercises using hand grippers or therapy putty, wrist curls and extensions with light dumbbells or resistance bands, and finger and thumb strengthening exercises. The intensity and resistance of these exercises should be gradually increased over time.
- Functional activities and sports-specific training: Once pain is minimal, range of motion is restored, and adequate strength is achieved, functional activities and sports-specific training can be incorporated into the rehabilitation program. This may involve practicing specific movements and techniques related to the individual’s sport or daily activities. It is important to progress gradually and listen to the body’s response to avoid re-injury.
- Gradual return to activity: Before returning to full activity or sports participation, it is crucial to ensure that the hamate bone has fully healed, and the surrounding structures are adequately strengthened. Your healthcare provider or physical therapist will guide you through a gradual return-to-activity plan, which may include modified training, protective equipment, and monitoring for any signs of pain or discomfort.
Throughout the rehabilitation process, it is essential to follow the guidance of medical professionals and adhere to any prescribed treatment plans or protocols. It is also important to maintain open communication with your healthcare team, reporting any changes in symptoms or concerns during the rehabilitation process.
FAQs
The hamate bone can be injured through trauma, such as a direct blow to the hand or a fall onto an outstretched hand. It can also be injured from repetitive motions, such as swinging a golf club or racket.
Symptoms of a hamate bone injury may include pain and tenderness in the wrist or hand, difficulty gripping or grasping objects, swelling, and a decreased range of motion.
A hamate bone injury is typically diagnosed through a physical examination by a healthcare professional. X-rays or other imaging tests may also be advised in order to confirm the diagnosis.
The healing time for a hamate bone injury can vary depending on the severity of the injury and the individual’s healing abilities. It may take several weeks to several months for complete healing to occur.
In some cases, a hamate bone injury may lead to long-term complications, such as chronic pain, stiffness, or weakness in the hand or wrist. However, with proper treatment and rehabilitation, most individuals can recover fully without long-term complications.
While it may not be possible to prevent all hamate bone injuries, taking precautions such as using proper technique and protective equipment during sports or activities that involve repetitive motions can help reduce the risk of injury. Strengthening the muscles of the hand and wrist through targeted exercises may also provide some protection.

2 Comments