
Hook Of The Hamate Fracture
Table of Contents
Introduction
Hook Of The Hamate Fracture is infrequent and underreported. These types of injuries are usually misdiagnosed or sometimes mistaken for simple wrist sprains. Delayed diagnosis is common.
The hamate is a triangular-formed bone that forms a portion of the distal carpal row, communicating with the capitate (radially), triquetrum (proximally), and fifth and fourth metacarpals (distally).
hook fractures and body fractures are divided into two types of hamate fractures.
Anatomy
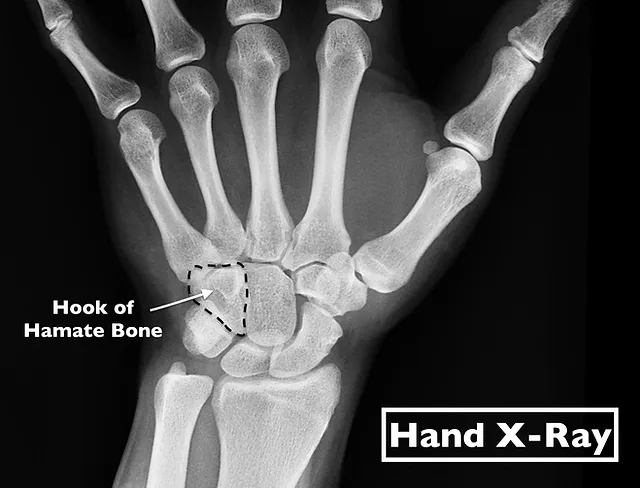
The hamate bone is one of eight carpal bones, it is a triangular-shaped bone, comprised of a body and a hook (hamulus), found on the ulnar side of the distal carpal row.
The hamate is a triangular like shaped bone that forms by the distal carpal row and connects with the capitate carpal bone (radially), triquetrum carpal bone (proximally), and fifth and fourth metacarpals (distally)
The Guyon canal (a fibro-osseous structure that comprises a groove between the pisiform and the hook of the hamate) maintains the artery and nerve of the ulna and, for this cause, hook fractures must offer a high chance of ulnar artery and nerve injury.
Cause of Hook Of The Hamate Fracture
- The hook of hamate fracture often happens during sports where a tight grip is needed, for example, tennis, baseball, and golf.
- The body of the hamate fractures is associated with high-impact injury for example a strong punch and may be related to contemporary carpal fractures and carpometacarpal dislocations. Body fractures are less expected.
Epidemiology
Hamate fractures are unusual hand trauma and account for 2 to 4 percent of carpal fractures. Hamate fractures (hook and body) tend to happen in young, active patients. They are uncommon in children age.
Mechanism of Injury
- The hook of hamate injuries is primarily because of repeated impact, usually, a sporting activity (racket, club, bat) exerting a direct force in front of the hamate.
- Avulsion-type fractures of the hook can even be possible, as the hook of the hamate plays as an attachment site for 3 tendons these tendons are followed by opponens and flexor digiti minimi, and flexor carpi ulnaris.
Symptoms of Hook Of The Hamate Fracture
Symptoms may be incomplete and unspecific, but wrist pain is expected. a patient may also have prolonged pain and swelling over the hypothenar aspect, which is located at the base of the palm on the same side as the little finger.
Weakened grip strength is ordinary. If an individual attempts to grip an object, they usually have pain along the wrist’s ulnar (outer) side. Flexing the ring finger and pinky finger may also result in pain.
Other symptoms may possess:
- swelling and tenderness
- reduced range of movement
- stiffness
- weakness
- numbness
- Muscle spasm
- pain when moving the wrist or hand
- difficulty in gripping and using the fingers
- an ulnar nerve injury, which can result in numbness in part of the hand or fingers.
Differential Diagnosis
Differential diagnosis includes:
- Flexor/extensor carpi ulnaris tendon injury
- Metacarpal/carpal bone fracture or contusion
- Triangular fibrocartilaginous complex tear
- Ulnar artery thrombosis
- Ulnar nerve neuropathy
- Carpal tunnel syndrome
Complications
- Nonunion
- Post-traumatic arthritis
- Avascular necrosis in the proximal pole (body fractures)
- Ulnar nerve compression (Guyon´s canal)
- Carpal tunnel syndrome
- Flexor digitorum profundus tendon rupture
- Ulnar artery thrombosis (hypothenar hammer syndrome)
- Ulnar artery compression
- Residual instability of fourth or fifth metacarpals
Diagnosis
Hook of Hamate fractures is diagnosed via physical assessments and x-rays. Standard X-rays for wrist traumas commonly do not display this fracture and need a special view referred to as a carpal tunnel view. A doctor may apply compression on the wrist to pinpoint the area of the injury. Due to this is usually not noticed in traditional imaging, there is frequently a delay in diagnosis (averaging four weeks).
Clinical doubt aids in the diagnosis. If a fracture is supposed with negative radiographs, advanced imaging with CT or MRI scans may be accepted.
Treatment
Hook Fractures
Acute, undisplaced fracture: There is still a point of discussion around whether the patients may benefit from early surgical treatment for this kind of fracture. Sports players will usually benefit from early surgical management, returning to sports activities in three months, and Immobilization under an ulnar gutter cast for six weeks.
Acute, displaced fracture: Excision of a bony segment is the gold standard approach. Open reduction and internal fixation (screws or Kirschner wires) is another established therapy. Both options offered similar clinical outcomes.
Chronic pain, nonunion: These symptoms need fracture pinning with bone grafting.
Body Fractures
Acute, nondisplaced: Immobilization, six-week cast.
Acute, displaced: ORIF (such as K-wires, grid plate, or headless reduction screws).
Physiotherapy Management
In conservative treatment, therapy should start straight after cast removal.
- Following any immobilization of the hand and wrist, there is usually a loss of supination and pronation strength and range, as well as a lack of intrinsic muscle strength and control.
- Distinctive physical therapy exercises are needed to manage this, and the complete upper limb may also require retraining to provide adequate proximal stability returns to the upper limb complex, especially if returning to sporting actions
Following ORIF, therapy must start after a 3-week immobilization program. Post-surgery, the physiotherapist will teach rehabilitation, and document back to the other members of the team as to the improvement or stagnation or regression of the rehabilitation strategy in coordination with the surgeon’s rehabilitation program.
Hook excisions may begin initial treatment.
The rehabilitation protocol should last 4 to 6 weeks.
- Relying on the damage passive and active exercises are demonstrated and exercised. As the function and range of movement enhance coordination exercises, exercises in front resistance and exercises to restore strength can be integrated into the exercise schedule.
- During the 1st days after trauma, edema in the hand may be evident, resulting in reduced function of the hand. Positioning the hand above the elbow can help in decreasing the swelling.
- During the rehabilitation, the physiotherapist utilizes passive mobilizations to standardize the ROM and the rolling and sliding motion of the active joint. These mobilizations may possess traction, translation, and angular mobilizations.
During rehabilitation after plaster immobilization of the wrist, there will be the presence of stiffness of the capsule in the wrist.
- Traction and translations are completed.
- The individual is also inspired to mobilize as much as possible the affected joints to improve function and return to activity as quickly as possible.
- Patients are motivated to actively move the adjacent non-involved joints to avoid stiffening other secondary complications.
- In the hand wrist and finger flexors are muscles that indicate an increased tone and have the tendency to contract. The flexors of the hand must be stretched and (as pain and swelling permit) add eccentric training.
- Progressive resistance exercises are involved when the fracture is adequately consolidated. The exercises contain concentric and eccentric muscle movements and open and closed chain exercises. Resistance exercises are essential to recovering adequate functionality of the hand.
- Low-intensity therapeutic US has been declared to be beneficial in enabling fracture recovery, it accelerates the normal fracture rehabilitation procedure.
- Therapeutic ultrasound therapy might be beneficial for nonunion fracture, it is a therapy for nonunion of the hook of the hamate and is a choice in several therapy techniques.
FAQ
Holding your elbow flexed and close to your side, to side, rotate your hand to turn the palm up, and then the palm down direction. It is useful to use a light hammer or light weighted dowel to perform this exercise Repeat 8 – 10 times, 3 – 4 times per day. Use an uninvolved hand to gently flex the problematic wrist downward.
Continuous pain following this damage is a typical indication for additional workup and following diagnosis of a hamate fracture. Complications have nonunion, post-traumatic arthritis, ulnar neuropathy, or flexor digitorum profundus tendon rupture.
Uncomplicated hook of hamate fractures commonly recoverin 6–8 weeks. After this, an individual may require several weeks to months to recover maximum strength and range of motion. People who have surgery may require 3 months or more before returning to their sport.
Therapy for a hook of hamate fracture
Early therapy commonly concerns immobilization in a plaster cast for four weeks. Regardless, if your damage is detected late, then it is likely it will fail to recover. If this occurs, the most prevalent choice is to surgically remove the hook fragment of bone entirely.
A fracture of the hook of the hamate elicits pain on the pinky finger side of the palm and a weakness of grip. Other signs may possess a decreased range of movement. swelling or inflammation.




