
Colle’s Fracture
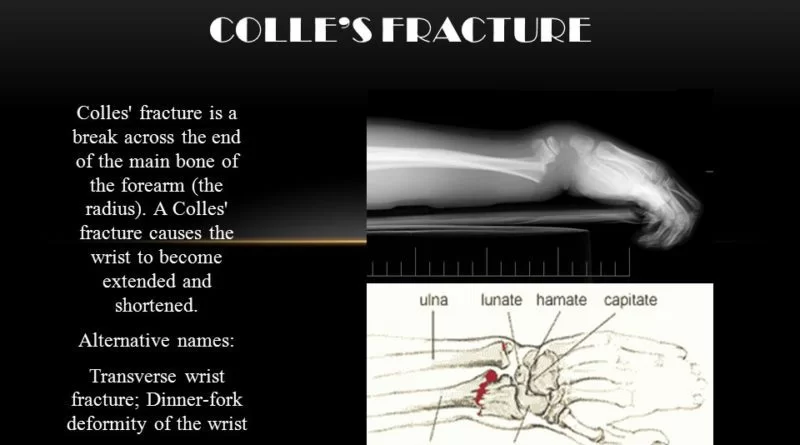
A Colle’s fracture is a type of fracture of the distal forearm in which the broken end of the radius is bent backwards. Symptoms may include pain, swelling, deformity, and bruising. Complications may include damage to the median nerve. It typically occurs as a result of a fall on an outstretched hand.
Other names: Colle’s fracture, Pouteau fracture.
A Colles Fracture is a complete fracture of the radius bone of the forearm close to the wrist resulting in an upward (posterior) displacement of the radius and obvious deformity. It is commonly called a “broken wrist” in spite of the fact that the distal radius is the location of the fracture, not the carpal bones of the wrist.
The Colle’s fracture is named after Abraham Colle’s, an Irish surgeon, who first described it in 1814 by simply looking at the classical deformity before the advent of X-rays.
The fracture originates from a fall on the outstretched hand and is usually associated with dorsal and radial displacement of the distal fragment, and disturbance of the radial-ulnar articulation. Possibly the ulnar styliod may be fractured. Communication of the distal fragment and fractures into the joint surface are present in some of these fractures. The colles fracture is one of the most common and challenging of the outpatient fractures. Colles’ fracture is defined as a linear transverse fracture of the distal radius approximately 20-35 mm proximal to the articular surface with dorsal angulation of the distal fragment.
Table of Contents
Related anatomy
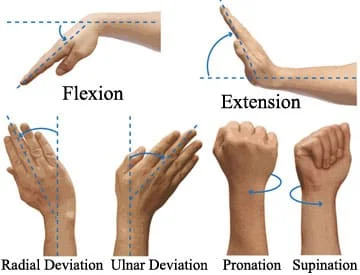
The distal radius forms the proximal side of the wrist joint. There, the radius articulates with the proximal row of carpal bones (allowing flexion and extension); it also articulates with the distal ulna (creating a joint for pronation and supination).
The distal ulna attaches to a meniscus-like structure, the triangular fibrocartilage discus, which can be torn with wrist fractures.
On the lateral side of the radius is a styloid process, onto which the brachioradialis inserts and from which the radial collateral ligament of the wrist originates.
At the distal metaphysis of the radius, the cortex of the bone is thinner than the bone proximal and distal, and the relative amount of cancellous bone increases. The distal metaphysis of the radius is therefore a relative weak point. This make fractures more likely, especially in patients with decreased bone mineral density.
Low energy extra-articular fracture of the distal radius. Can be associated with ulnar styloid Etiologyfracture, TFCC tear, scapholunate dissociation.
Causes of Colle’s Fracture
Females are predilected more than males for this type of injury and oftentimes there is a precedent history of osteoporosis.’ In the United States and in Northern Europe, colles fractures are the most common fractures in women up to the age of 75 years. It is known that these fractures appear mostly by young adults and the elderly. Stable Colles’ fractures present with minimal comminution. Unstable fractures are distinctly comminuted often with corresponding avulsions of the radial or ulnar styloid, that have the potential to cause compression neuropathies, especially of the median nerve. Other complications that have been reported are degenerative joint disease and reflex sympathetic dystrophy.
Colle’s fractures are the most common type of distal radial fracture and are seen in all adult age groups and demographics. They are particularly common in patients with osteoporosis, and as such, they are most frequently seen in elderly women. The relationship between Colles fractures and osteoporosis is strong enough that when an older male patient presents with a Colles fracture, he should be investigated for osteoporosis because his risk of a hip fracture is also elevated.
Younger patients who sustain Colle’s fractures have usually been involved in high impact trauma or have fallen, e.g. during contact sports, skiing, horse riding.
Younger patients have stronger bone, and thus, more energy is required to create a fracture in these individuals. Motorcycle accidents, falls from a height, and similar situations are common causes of a DRF. Trauma is the leading cause of death in the 15- to 24-year-old age group, and this is also reflected in the incidence of lesser traumas.
- “Dinner Fork” Deformity
- History of fall on an outstretched hand
- Dorsal wrist pain
- Swelling of the wrist
- Increased angulation of the distal radius
- Inability to grasp object
- Signs and Symptoms- Pain, numbness, tenderness, bruising, deformity of wrist.
- treatment. As the population lives longer, the frequency of this type of fracture will increase.
Older patients have much weaker bones and can sustain a DRF from simply falling on an outstretched hand in a ground-level fall. An increasing awareness of osteoporosis has led to these injuries being termed fragility fractures, with the implication that a workup for osteoporosis should be a standard part of The clinical presentation of Colles fracture is commonly described as a dinner fork deformity. A distal fracture of the radius causes posterior displacement of the distal fragment, causing the forearm to be angled posteriorly just proximal to the wrist. With the hand displaying its normal forward arch, the patient’s forearm and hand resemble the curvature of a dinner fork.
Common Signs of a Colle’s Fracture
If you have suffered trauma to your wrist or have fallen onto your hand or wrist, you may have a Colle’s fracture. Common signs and symptoms of a wrist fracture or Colle’s fracture include:
- Pain
- Swelling in the arm, wrist, or hand
- Bruising
- Loss of mobility in the wrist
- Visible deformity of a lump on the back side of your forearm near your wrist.
Diagnosis
A careful history including the mechanism of injury establishes suspicion for a Colle’s fracture. Diagnosis is most often made upon interpretation of pasteroanterior and lateral views alone.
The classic Colle’s fracture has the following characteristics;
Transverse fracture of the radius
2.5 cm (0.98 inches) proximal to the radio-carpal joint
dorsal displacement and dorsal angulation, together with radial tilt
Other characteristics on plain radiographs may include:
Radial shortening
Loss of ulnar inclination
Radial angulation of the wrist
Comminution at the fracture site
Associated fracture of the ulnar styloid process in more than 60% of cases.
Differential Diagnosis
- Scapholunate ligament tear
- Median nerve injury
- TFCC (triangular fibrocartilage complex) injury, up to 50% when ulnar styloid fx also present
- Carpal ligment injury:Scapholunate Instability(most common), lunotriquetral ligament
- Tendon injury,attritional EPL rupture, usually treated with EIP tendon transfer
- Compartment syndrome
- Ulnar styloid fracture
- DRUJ (Distal Radial Ulnar Joint) Instability
- Galeazzi Fracture: highly associated with distal 1/3 radial shaft fractures
Investigation Of Colle’s Fracture :
X-RAY : Mostly Used.
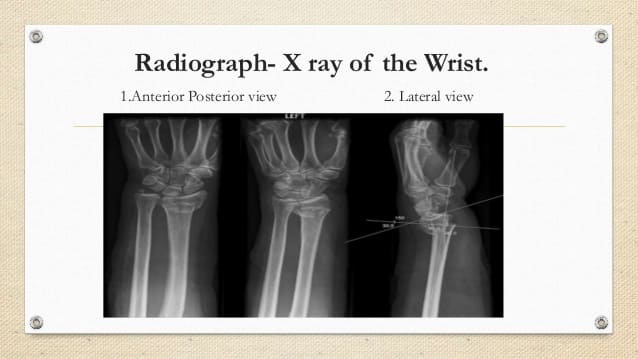
Mostly Examination With X-Ray Are Enough If No Other Major Injury is Associated With This.
MRI
CT Scan
Orthopedic Treatment:
Orthopaedic Treatment/Management depends Mainly on the severity of the fracture. An undisplaced fracture may be treated Immobilization Technique with a cast/Plaster . The cast is applied with the distal fragment in palmar flexion & ulnar deviation. A fracture with mild angulation and displacement may require closed reduction. There is Few evidence Shows that immobilization with the wrist in dorsi-flexion as opposed to palmar-flexion results in less redisplacement and better functional status. Significant angulation and deformity may require an open reduction and internal fixation or external fixation. The volar forearm splint is best for temporary immobilization of forearm, wrist and hand fractures, including Colle’s fracture. There are several established instability criteria: dorsal tilt >20°, comminuted fracture, abruption of the ulnar styloid process, intraarticular displacement >1mm, loss of radial height >2mm.
A higher amount of instable Fracture Require operative treatment.Treatment modalities differ in the elderly.
Regular Follow Up With X-ray Examination are Require at one, two, and six weeks to verify proper healing.
After Removal Of Cast/Fixation/Plaster Wrist Joint Stiffness Removal Physiotherapy Exercise Are Recommended.


Post-Operative Physiotherapy Treatment:
Many patients will present to a physiotherapist with pain, edema, decreased range of motion, decreased strength, and decreased functional abilities. Once a Colle’s fracture has healed, rehabilitation is recommended in an attempt to restore function and strength to the fractured wrist.
The primary focus in early rehabilitation is to mobilize the wrist, which is indicated approximately 7-8 weeks post fracture. If the fracture has been managed using an internal fixation device, early mobilization can begin as early as 1 week post surgery. Caution should be paid to fractures that have been treated with external fixation as the wrist is often held in a pronated position. This can predispose the patient to a contracture at the distal radio-ulnar joint.
Other soft tissue injuries that may affect rehabilitation progress include; edema, cast impingement, infection, osteomyelitis, adherent scar, intrinsic or extrinsic muscle tightness, joint capsular tightness, neurovascular injury, ligament injury, and post-traumatic arthritis.
Initial Rehabilitation
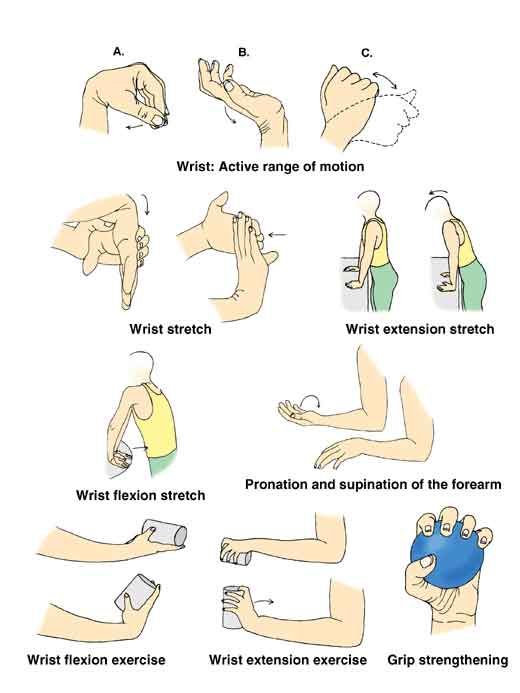
One of the primary goals in early rehab is to restore normal range of motion (ROM) at the wrist with both passive ROM and progression to active ROM. Wrist flexion and extension are often the first motions emphasized working within the patients pain free avaialble range. Wrist flexion and extension are often the first motions emphasised working within the patients pain free available range. The addition of ROM exercises helps to limit scar tissue and adhesion formation that commonly occur after surgery. It is also important to emphasise motion at the joint above and below (shoulder, elbow, and fingers) during all phases of rehab. One of the primary focuses in early rehab is to limit pain and the amount of oedema present in the wrist and hand region.
Sub-acute Phase:
The next phase of rehab in the treatment of Colle’s fracture continues to focus on increasing wrist ROM and the commencement of strengthening exercises. For fractures that were surgically treated, ROM should be regained between 6 to 8 weeks post-op. Examples of ROM exercises that can performed include: wrist flexion/extension, radial/ulnar deviation, pronation/supination, and making a fist and opening.In the sub-acute phase, ROM exercises can progress into strengthening by performing all exercises with a weight in the hand or performing grip squeeze with a foam ball or a towel roll. During strengthening, it is important to address all forearm muscles but also the extrinsic and intrinsic hand muscles progressively building resistance as the individual gets stronger. During this phase, progressive stretching can begin to increase available ROM. Each stretch should be held for 30-60 seconds for 3 repetitions. If the patient is unable to tolerate a slow, prolonged stretch, shorter stretches of 10 seconds can be performed for 10 repetitions.
Modalities For Pain Relief:
Heat/Paraffin Wax :
Heat whether in the form of a heat pack or paraffin wax can be very beneficial in the early stages to increase ROM and decrease pain.It is often used with cold therapy to improve venous return.
Massage
Massage to reduce scar tissue and retrograde massage to reduce swelling are two effective modalities used in rehabilitation post colles fracture. The benefit is that can also be taught to the patient to continue independently when in their own homes.
Cryotherapy
Cryotherapy is an effective modality for controlling edema in the acute phase after trauma and during rehab due its ability in helping to decrease blood flow through vasoconstriction limiting the amount of fluid escaping from capillaries to the interstitial fluid. Cryotherapy can also be combined with compression and elevation in the treatment of oedema.To control pain using cryotherapy, the modality should be applied to the area for 10-15 minutes which can result in pain control up to 2 hours post application. Precautions for the use of cryotherapy include: over a superficial branch of nerve, over an open wound, poor sensation or mentation, and very young or very old patients.Contraindications for cryotherapy include; Acute febrile illness, Vasospasm e.g. Raynaud’s disease, Cryoglobinaemia, Cold urticaria.
TENS ( Transcutaneous electrical nerve stimulation) :
The use of transcutaneous electrical nerve stimulation (TENS) may be used as an adjunct during any phase of rehab to address pain but can be particularly useful for patients that are increasing the level of activity of the wrist. Conventional (high-rate) TENS is useful for disrupting the pain cycle through a prolonged treatment session as great as 24 hours a day. Low-rate TENS is another form of electrical stimulation that is successful in diminishing pain by targeting motor or nociceptive A-delta nerves. Low-rate TENS has been reported to be effective in pain control for up to 4-5 hours post-treatment.
The literature is still not conclusive on this topic and the results of one study may contradict or, on the contrary, reinforce the results of another study.Yet there is evidence supporting the beneficial effects of electrical stimulation, especially in combination with physiotherapy exercises.
Exercise Of Wrist Joint:
Exercise is beneficial in the restoration of range and also vital to strengthen the hand, wrist, elbow and shoulder. Immobility at the wrist has a huge effect on range of movement and power. Exercises to increase ROM can be as simple as walking the hand up the wall, whereas exercises such as tearing paper, writing and drawing are great for strengthening the wrist and for improving the strength and dexterity of the hand. Being able to use opposition and pinching are vital for improving function and regaining independence in ADLs. Even simple tasks like buttoning a shirt can be difficult after a colle’s fracture.
After about four to six weeks of immobilization, your doctor may remove the cast and you may be referred to physical therapy. Some of the common impairments that your physical therapist may measure and evaluate include range of motion (ROM), strength, pain, and swelling. If you had an ORIF to reduce the fracture, your physical therapist may assess your surgical scar tissue. He or she may also analyze your hand, wrist, and arm function.
After your initial evaluation, your physical therapist will work with you to develop an appropriate plan of care to help improve the impairments and functional limitations that you may have. Be sure to ask any questions if you have any. Your PT may prescribe a specific exercise program after your Colle’s fracture.
Range of motion Exercise:
After a Colle’s fracture, you may have lost a lot of mobility in the hand, wrist, and elbow. Your shoulder may also be tight, especially if you have been wearing a sling. The range of motion exercises for the hand, wrist, and elbow may be prescribed, and you may have to perform ROM exercises at home.
To Achieve Full Range Of Motion Compare With Normal Wrist And Try To Reach Full Range Of Wrist Joint Flexion , Wrist Extension And Wrist Ulnar Deviation And Radial Deviation.
To See Youtuve Video Of Wrist Mobilization Exercise :
Strengthening Exercise :
Loss of strength is common after a Colle’s fracture. Exercises that focus on hand, wrist and elbow strength may be prescribed. Again, you may be required to perform exercises at home to get the best results from physiotherapy.
Pain and swelling:
After a Colle’s fracture, you may experience pain and swelling around your wrist and hand. Your physical therapist can provide you with various treatments and modalities to help decrease the swelling and pain.
Scar tissue:
If you have had an ORIF procedure to reduce your Colles’ fracture, there will likely be scar tissue that has developed around the surgical incision. Your physical therapist may perform scar tissue massage and mobilization to help improve the mobility of your scar. He or she can also teach you how to do it on yourself.
After a few weeks of physical therapy, you should notice that your mobility and strength are improving while your pain and swelling are decreasing. You may be finding it easier to use your arm and hand to perform functional activities. While the fracture should be fully healed six to eight weeks after injury, you may still be limited for up to 12 to 16 weeks. Be sure to work closely with your doctor and physical therapist to know what to expect.
A broken wrist or Colle’s fracture can be a painful and scary experience. It may be difficult for you to use your hand and arm to perform basic functions like dressing, feeding yourself, or brushing your hair. You may be unable to perform your job or engage in recreational activities. Your physical therapist can help you improve your functional mobility to be sure you can quickly and safely return to normal activity.




6 Comments