

Fibula bone
Table of Contents
Introduction
On the lateral side of the tibia is the fibula, a long bone in the lower extremity. The tibia is thicker and much smaller than the fibula. It begins at the knee joint just behind the tibial head and continues laterally down the leg until it reaches the ankle joint. The interosseous border connects the fibula to the tibia via the interosseous membrane and is formed by a ridge on the medial surface of the fibula. This association frames a syndesmotic joint, meaning it has next to no versatility.
The middle and either end of the epiphysis of the fibula, like the tibia, are ossified. Around the eighth week of pregnancy, ossification of the fibula begins in the shaft and spreads to both ends. By the second decade of life, ossification has been completed. Cartilage remains at the fibula’s two ends.
Structure and Function of Fibula Bone
The fibula does not support weight, unlike the tibia. Its primary function is to stabilize the ankle joint by joining with the tibia. Numerous ligament attachment grooves on the distal end of the fibula stabilize and provide leverage during ankle movements. The lateral side of the fibular head is where the lateral (fibular) collateral ligament attaches. Knee stability is provided by this ligament. However, knee stability is largely provided by the fibula itself.
Blood Supply and Lymphatics
The fibular artery, also known as the peroneal artery, supplies the diaphysis with blood through a network of numerous small branches. The anterior tibial artery’s branches supply the epiphysis and the proximal fibular head. Additionally, the rest of the bone is supplied by the periosteum, which receives numerous small branches from the fibular artery. Because this bone is frequently used as a graft for the reconstruction of the mandible, it is essential to know the fibula’s blood supply.
Nerves
The lower limb’s lateral compartment is bordered by the lateral surface of the fibula, deep fascia, and intermuscular septum. The superficial fibular nerve, which controls plantar flexion and eversion, is located within this compartment. The borders of the lower limb’s posterior compartment are the posterior surface of the fibula, deep fascia, and interosseous membrane. This compartment is traversed by the tibial nerve, which controls plantar and digit flexion. The lower limb’s anterior compartment is partially bounded by the medial surface of the fibula.
Muscles Related to Fibula Bone
The fibula is where a lot of important muscles attach, which helps shape the fibular shaft.
- The fibular head is where the biceps femoris tendon attaches.
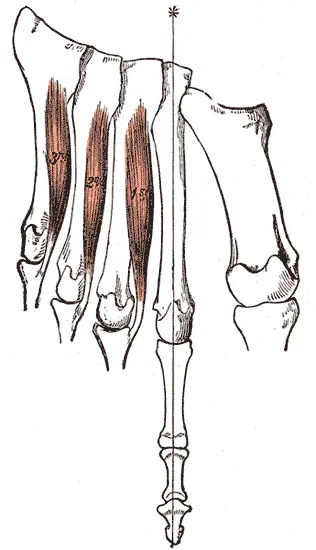
- The lateral fibula is where the tendons for the fibularis longus and brevis attach.
- The medial fibula is where the extensor digitorum longus and extensor hallucis longus tendons join.
Fibular muscle accessory tendon variations are quite common.
Surgical Considerations
In mandibular reconstructive procedures, femur bone grafts are the gold standard. This is due to the fact that weight bearing is primarily the role of the tibia, and removing the fibula from its anatomical location will have little effect. In addition, the fibula is long and thin while remaining extremely vascular. This makes it simple for dental implants to absorb grafts and osseointegrate. Only the shaft and two ends of the fibula are used as grafts when using the fibula.
Clinical importance
Congenitally
There is solid help in ongoing writing to utilize the fibular shaft length to appraise baby bone age. This might be a more precise option in contrast to the ongoing strategies for counting hardening focuses or seeing hand/wrist or knee radiographs as a method for assessing baby bone age.
The most common long-bone deficiency is fibular hypoplasia-aplasia or fibular hemimelia. The fibula may or may not disappear as a result of this. This is typically analyzed upon entering the world when appendage length disparity and absence of digits are noted. Additionally, the mortise in the valgus is destabilized by the absence of a lateral malleolus. Therefore, ankle fusion is typically required.
Neurologically
A slightly enlarged prominence on the proximal end of the fibula contains a facet that articulates with the tibia’s lateral condyle. The common fibular nerve—also referred to as the common peroneal nerve—is located just lateral and posterior to the fibular neck. During its course near the fibular head or as a result of direct injury, the common fibular nerve can become entangled. The most common type of entrapment neuropathy in the lower extremity is common fibular nerve entrapment. Foot drop and sensory deficits in the lateral limbs are possible symptoms, but due to the lack of obvious symptoms, misdiagnosis is common and may delay treatment.
Fractures
When the biceps femoris muscle contracts suddenly, an avulsion fracture can occur in the fibula. Because the biceps femoris tendon attaches to the fibular head, this causes a significant pull on the fibula.
The lateral malleolus continues to develop from the distal fibula. The lateral malleolus can be felt at the ankle because it is much more obvious than the medial malleolus. On the sidelong part of the lower leg, the distal fibula is additionally inclined to break (generally twisting), which can happen during constrained outside turns of the lower leg. Either direct trauma or eversion of the foot, also known as outward twisting of the foot, can cause injury. Typically, an eversion injury results in a transverse fracture of the fibula. A clinical dynamic device called The Ottawa Lower leg Rules (Paddle) can be utilized in thought sidelong malleolus wounds. The OAR is a reliable method for excluding fractures in children over the age of 18 and helps reduce the number of unnecessary radiographs.
Compartment syndrome is rarely caused by fractures of the femur alone. However, there is a greater likelihood that the fibular fracture will contribute to compartment syndrome when there is a tibial plateau fracture.
The ankle fracture is the most common type of fibula fracture, which occurs at the bone’s distal end. There are three categories in the Danis–Weber classification:
Type A: distal to the syndesmosis, which is the connection between the tibia and fibula’s distal ends, there is a fracture in the lateral malleolus.
Type B: Type C: Fibula fracture at the level of the syndesmosis a fibula fracture close to the syndesmosis.
Spiral fracture of the proximal third of the fibula known as a Maisonneuve fracture is accompanied by an interosseous membrane tear and distal tibiofibular syndesmosis. There is also a rupture of the deep deltoid ligament or a fracture of the medial malleolus.
A fracture of the fibular head caused by a sudden contraction of the biceps femoris muscle that pulls its attachment site on the bone is referred to as an avulsion fracture of the head of the fibula. The lateral collateral ligament of the knee and the biceps femoris tendon that attaches to the fibular head are closely related. As a result, in this kind of avulsion fracture, this ligament is prone to injury.
Compartment syndrome is rarely caused by fractures of the femur alone. However, there is a greater likelihood that the fibular fracture will contribute to compartment syndrome when there is a tibial plateau fracture.
FAQs
Its primary function is to stabilize the ankle joint by joining with the tibia. Numerous ligament attachment grooves on the distal end of the fibula stabilize and provide leverage during ankle movements.
The popliteal or posterior tibial artery, which branches from the popliteal or posterior tibial at the trifurcation point of the posterior tibial, anterior tibial, and peroneal just distal to the popliteal fossa, provides the majority of the fibula’s blood supply.
From the posterior tibial tubercle, the posterior-inferior tibiofibular ligament connects to the posterior lateral malleolus. It and the anterior-inferior tibiofibular ligament bind the tibia and fibula together.
Two long bones in the lower leg are the tibia and the fibula. The tibia is larger on the inside, while the fibula is smaller on the outside. ed in the lower leg. On the inside, the tibia is larger, while the fibula is smaller on the outside.
You have broken the outside bone of your ankle (fibula). This takes roughly 6 to about two months to mend, despite the fact that aggravation and enlarging can go on for three to a half years. As long as you feel comfortable, you can walk on your feet, but in the beginning, you might find it easier to walk with crutches.


6 Comments