
Compartment Syndrome: Physiotherapy Treatment
Table of Contents
What is a Compartment Syndrome?
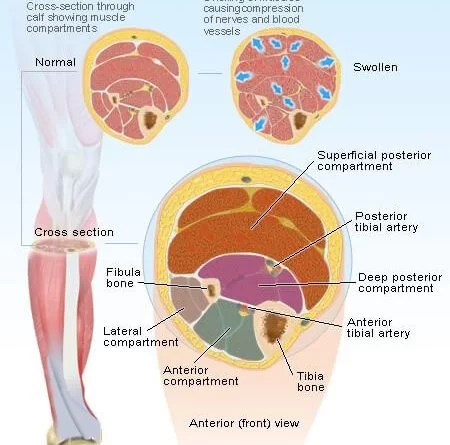
Compartment syndrome is a condition in which increased pressure within one of the body’s compartments results in insufficient blood supply to tissue within that space.Compartment syndrome usually results from bleeding or swelling after an injury. There are two main types: acute and chronic.The leg or arm is most commonly involved.
Groups of organs or muscles are organized into areas called compartments. Strong webs of connective tissue called fascia form the walls of these compartments.After an injury, blood or edema may accumulate in the compartment. The tough walls of fascia cannot easily expand, and compartment pressure rises, preventing adequate blood flow to tissues inside the compartment. Severe tissue damage can result, with loss of body function or even death.
Causes of Compartment Syndrome
Acute compartment syndrome is the most common type of compartment syndrome. Acute compartment syndrome occurs in about 3% of those who have a mid-shaft fracture of the forearm.Compartment syndrome can develop from the fracture itself, due to pressure from bleeding and edema. Or compartment syndrome may occur later, as a result of treatment for the fracture such as surgery and POP.
Acute compartment syndrome can also occur after injuries without bone fractures, including:
- Crush injuries
- Burns
- Overly tight bandaging
- Prolonged compression of a limb during a period of unconsciousness
- Surgery to blood vessels of an arm or leg
- A blood clot in a blood vessel in an arm or leg
- Extremely vigorous exercise, especially eccentric movements (extension under pressure)
- vigorous exercise.

Signs and Symptoms of Compartment Syndrome
Acute
There are five characteristic signs and symptoms related to acute compartment syndrome: pain, paraesthesia (reduced sensation), pallor, and pulselessness. Pain and paresthesia are the early symptoms of compartment syndrome.
- Pain – The pain would be disproportionate to the findings of the physical examination, is not relieved by analgesia up to and including morphine. The pain is aggravated by passively stretching the muscle group within the compartment. However, such pain may disappear in the late stages of the compartment syndrome.The role of local anaesthesia in delaying the diagnosis of compartment is still being debated.
- Paresthesia (altered sensation) – A person may complained of “pins & needles”, numbness, and tingling sensation. This may progress to loss of sensation (anesthesia) if no intervention has been made.
- Paralysis – Paralysis of the limb is a rare, late finding. It may indicate both nerve or muscular lesion.
- Pallor and pulselessness – A lack of pulse rarely occurs in patients, as pressures that cause compartment syndrome are often well below arterial pressures. Absent pulses only occurs when there is arterial injury or during the late stages of the compartment syndrome.

- Swelling, tightness and bruising.

Chronic
The symptoms of chronic exertional compartment syndrome (CECS) are brought on by exercise and consist of a sensation of extreme tightness in the affected muscles followed by a painful burning sensation if exercise is continued. After exercise is ceased, the pressure in the compartment will decrease within a few minutes, relieving painful symptoms. S
Symptoms will occur at a certain threshold of exercise which varies from person to person but is rather consistent for a given individual and can range anywhere from 30 seconds of running to about 10–15 minutes of running. CECS most commonly occurs in the lower leg, with the anterior compartment being the most frequently affected compartment.Foot drop is a common symptom of CECS.
Different Types of Compartment Syndrome
Acute compartment syndrome
Acute compartment syndrome is a medical emergency that is typically caused by a serious injury. Acute compartment syndrome can irreversibly harm muscles if left untreated. Moreover, it may result in death, paralysis, or disability.
Chronic compartment syndrome
Usually, chronic compartment syndrome does not require immediate medical attention. Physical strain, such as prolonged exercise, is frequently the cause of it. For this reason, medical professionals sometimes refer to it as exertional compartment syndrome.
Differential Diagnosis
Patients with exercise-induced lower leg pain, differential diagnosis includes:
- medial tibial stress syndrome (MTSS)
- fibular and tibial stress fractures
- fascial defects
- nerve entrapment syndromes,
- vascular claudication
- lumbar disc herniation.
Diagnosis
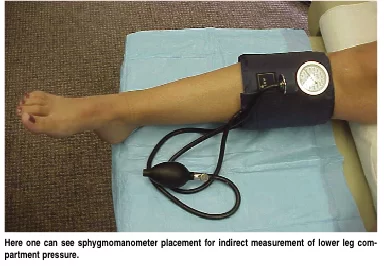
Apart from the typical signs and symptoms, measurement of intra-compartmental pressure is also important for diagnosis. A transducer connected to a catheter is inserted 5 cm into the zone of injury.A pressure higher than 30 mmHg of the diastolic pressure in conscious or unconscious person is associated with compartment syndrome; and fasciotomy is indicated. For those with hypotension, a pressure of 20 mmHg higher than the intra-compartmental pressure is associated with compartmental syndrome.
According to Blackman one of the tools to diagnose compartment syndrome is X-ray to show a tibia/fibula fracture, which when combined with numbness of the extremities is enough to confirm the presence of compartment syndrome.
Less invasive measurement techniques:
- Laser Doppler ultrasound
- Methoxy isobutyl isonitrile enhanced magnetic resonance imaging (MRI)
- Phosphate-nuclear magnetic resonance (NMR) spectroscopy
Treatment of Compartment Syndrome
Medical Management
- The gold standard treatment is fasciotomy, but most of the reports on its effectiveness are in short follow-up periods.It is recommended that all four compartments (anterior, lateral, deep posterior and superficial posterior) should be decompressed by one lateral incision or anterolateral and posteromedial incisions.Surgery Patients may be able to participate in all common activities a few days post surgery.Treatment should begin with rest, ice, activity modification and if appropriate, nonsteroidal anti-inflammatory drugs.

Physiotherapy Treatment:
The cessation of causative activities is the only nonoperative treatment that can be relied upon to reduce CECS pain. If pain permits, regular physical activities should be adjusted.
Patients who want to maintain their cardiorespiratory fitness may choose to cycle instead of run because cycling has a lower risk of compartment pressure elevation. Patients who refuse surgical intervention or who have mild symptoms may benefit somewhat from massage therapy.
However, nonoperative treatment has not always been successful, and symptoms will not go away on their own. As previously mentioned, if compartment syndrome is left untreated, it can result in ischemia of the muscles and nerves, which can ultimately cause irreversible damage such as muscle necrosis, tissue death, and a lifelong neurological deficit within the compartment.
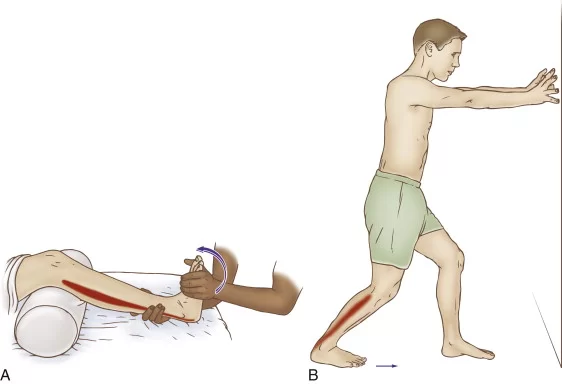
- Aquatic exercises, such as running in water, can maintain/improve mobility and strength without unnecessarily loading the affected compartment. Massage and stretching exercises also have been shown to be effective.

Post-surgical management
Post-surgical therapy for CECS includes:
- Assisted weight bearing exercise with variation,
- Early mobilisation is recommended as soon as possible to minimise scarring, which can lead to adhesions and a recurrence of the syndrome.
- Activity can be upgraded to stationary cycling and swimming after healing of the surgical wounds,
- Isokinetic muscle strengthening exercises can begin at 3-4 weeks,
- Running is added into the activity program at 3-6 weeks,
- Full activity is introduced at approximately 6-12 weeks, with a focus on speed and agility.



The following are recommendations for a full recovery and to avoid recurrence;
- Wearing more appropriate footwear to the terrain
- Choosing more appropriate surfaces and terrain for exercise
- Pacing your activities
- Avoiding certain activities altogether
- Mastering strategies for recovery and maintenance of good health (e.g, appropriate rest between sessions)
- Modifying the workplace to lower the risk of injury
- Postoperative physiotherapy treatment and exercise is essential for a successful recovery. depending on the nature of the procedure, expected timelines for healing and progress made during rehabilitation. Treatment incorporates strategies to restore range of motion, mobility, strength and function.
Prevention
Acute compartment syndrome caused by an injury or accident cannot be avoided. To avoid difficulties, however, you can seek early diagnosis and treatment.
Inform your healthcare practitioner if you believe that your cast or splint is overly tight. If you’ve taken painkillers and the affected area of your body is still hurting or swelling, pay close attention. It is necessary to alter the cast or splint in order to avoid compartment syndrome.
Prognosis
Treatment for acute compartment syndrome must start right away. If the pressure isn’t released right away, the illness may cause:
- Muscle contracture (deformity).
- Permanent damage to muscles and nerves, within 24 hours.
- Permanent disability.
- Amputation.
- Death.
Conclusion
Take medical attention right away if you believe you have acute compartment syndrome following an injury. Additionally, if you experience persistent, strange discomfort, edema, or muscular weakness, see a healthcare professional. You should check just to be sure because it might turn out to be shin splints or tendonitis.
Chronic compartment syndrome could be the cause. A medical professional can offer tips on how to improve your condition and protect your muscles and nerves from harm.
FAQ
5 characteristic signs of a compartment syndrome:
Pain,
Pallor (pale skin tone),
Paresthesia (numbness feeling)
Pulselessness (faint pulse)
Paralysis (weakness with movements).
Numbness, tingling, or pain may be associated in the leg and foot.
An increase in internal muscular pressure known as compartment syndrome limits blood flow and produces pain. If it occurs unexpectedly, it may be dangerous and require prompt medical attention.
A musculoskeletal disorder called chronic exertional compartment syndrome is triggered by physical activity. Although it can affect the muscle compartments in any limb, the lower legs are the most frequently affected. There are four compartments in the lower leg, and any one of them could be impacted.
Non-steroidal anti-inflammatory medicines (NSAIDs), such as ibuprofen or naproxen, are prescribed by doctors to treat pain and reduce swelling and inflammation in the affected muscle compartments. These drugs are used orally and are available without a prescription.
3 ways to treat compartment syndrome are:
To release pressure, a cast or bandage that is excessively tight should be cut or loosened.
Avoid the workout or repeated activity, or altering the method.
To reduce swelling, elevate the affected region above the level of the heart.
Early signs and symptoms include tense, swollen compartments, pain with passive stretching of the affected compartment’s muscles, and increasing pain that is out of proportion to the injury.
To diagnose compartment syndrome: Compartment Pressure Testing
In order to do this test, a physician first numbs the affected muscles with a tiny injection of anesthetic. To measure the pressure inside the muscle compartment, he or she introduces a handheld equipment that is attached to a needle into the compartment.
In order to release pressure in the affected compartment, a surgeon will need to make incisions in your skin and fascia if you have acute compartment syndrome. Resting will assist if you have chronic compartment syndrome. That usually settles the problem down.



Hi
I wish to know where I can get intracompartment pressure measured for diagnosing chronic exertional compartment syndrome.