

Polydactyly
Table of Contents
What is Polydactyly?
Polydactyly consists of poly which means multiple & dactyls, which means digits. Polydactyly, also known as hyperdactyly, is the most typical congenital anomaly of the hand & foot. It is determined by an additional finger and toe that may result from insufficient development during anterior-posterior patterning of the developing limb. It may occur in isolation [ non-syndromic polydactyly ] or associated with other birth weaknesses as a part of a syndrome [ syndromic polydactyly ].
Because it can be a component of a syndrome, the therapist or clinician should be prepared to consider the newborn baby with polydactyly & consider the other syndromic manifestations that may be associated with this anomaly. There is an increased movement of polydactyly to involve the right hand rather than the left hand, the upper limb rather than the lower limb, & the left foot rather than the right.
Types of Polydactyly
Polydactyly usually occurs without other anomalies. This is called isolated/nonsyndromic polydactyly.
Periodically it is associated with another hereditary condition. This is called syndromic polydactyly.
Isolated polydactyly
There are 3 types of isolated polydactyly, categorized by the part of the extra digit:
- Postaxial polydactyly appears on the outside of the hand and foot, where the 5th digit is. On the hand, this is named the ulnar side. This is the most typical type of polydactyly.
- Preaxial polydactyly appears on the inside of the hand and foot, where the thumb or big toe is. On the hand, this is named the radial side.

Central polydactyly appears in the middle digits of the hand and foot. It’s the least typical type.
Causes of Polydactyly
- Preaxial polydactyly- Hemingway mutant,
- Ectopic SHH-expression,
- Right forelimb
Mutations in Hoxa- or Hoxd groups are reported to lead to polydactyly. Interchanges of Hoxd13 & GLI3 induce synpolydactyly, a mixture of extra & consolidated digits. Additional signal transduction routes in this context are the Wnt signaling pathway or Notch.
In the typical case of preaxial polydactyly [ Hemingway mutant ], a cis-acting conversion around 1Mb upstream of the SHH gene has been implicated. Generally, SHH is described in an organizer area, called the zone of polarizing activity (ZPA) on the posterior side of the limb. From there it diffuses anteriorly, & laterally to the development direction of the limb. In the mutant, a smaller ectopic expression in a unique organizer area is seen on the anterior side of the limb.
When it happens by itself, it is associated with autosomal dominant transformations in single genes, i.e. it is not a multifactorial trait. But a mutation in a combination of genes can provide rise to polydactyly.
Conditions associated with polydactyly contain:
- syndactyly [ webbed hands or feet ]
- asphyxiating thoracic dystrophy
- Carpenter syndrome
- Ellis-van Creveld syndrome [ chondroectodermal dysplasia ]
- Laurence-Moon-Biedl syndrome
- Rubinstein-Taybi syndrome
- Smith-Lemli-Opitz syndrome
- trisomy 13
Syndromes
Because polydactyly can be part of a syndrome known as a hereditary deficiency or association congenital deficiency not known, children with a congenital upper extremity deformation should be investigated by a geneticist for other congenital abnormalities. This should also be done if a syndrome is supposed, or if more than 2 or 3 generations of the family are affected.
Ulnar polydactyly
Ulnar polydactyly is usually bilateral & associated with syndactyly & polydactyly of the feet. This can be a superficial or complex polydactyly. Ulnar polydactyly appears as a different congenital disease, but can also be part of a syndrome, such as
- Trisomy 13
- Greig cephalopolysyndactyly syndrome
- Meckel syndrome
- Ellis–van Creveld syndrome
- McKusick–Kaufman syndrome
- Down syndrome
- Bardet–Biedl syndrome
- Smith–Lemli–Opitz syndrome
Radial polydactyly
Radial polydactyly is associated with multiple syndromes:
- Holt–Oram syndrome,
- Fanconi anemia [ aplastic anemia by the years of 6 ],
- Townes–Brocks syndrome,
- Greig cephalopolysyndactyly
Central polydactyly
The syndromes associated with prominent polydactyly are :
- Bardet–Biedl syndrome
- Meckel syndrome
- Pallister–Hall syndrome
- Legius syndrome,
- Holt–Oram syndrome.
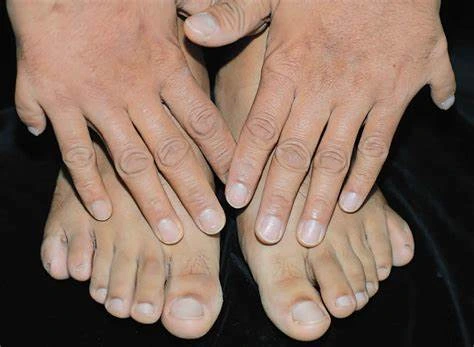
Signs and symptoms of Polydactyly
Male with unilateral preaxial polydactyly impacting the left thumb. The excessive digit had normal sensation but no joint & hence could not move independently.
In humans or animals, this situation can present itself on one or both hands or feet. The extra digit is generally a small portion of soft tissue that can be removed. Sometimes it includes bone without joints: rarely it may be a completely functioning digit. The additional digit is most common on the ulnar [pinky finger ] little finger side of the hand, less common on the radial (thumb) side, & rarely within the middle 3 digits. These are comprehended as central [ ring, middle, index fingers ], postaxial [ little (pinky) finger ], preaxial [ thumb ], and polydactyly. Polydactyly can diverge into 3 major types, which are conferred below, and depend on the location of the additional digit.
Polydactyly with a completely functional additional digit, muscles to hold the extra digit may be duplicated, resulting in improved motor control that permits the patient to carry out specific tasks with one hand that would generally require two.
Ulnar or postaxial polydactyly
Postaxial polydactyly
This is the most common problem, in which the extra digit is on the ulnar side of the hand, thus the side of the little ( pinky ) finger. This can also be named postaxial polydactyly. It can manifest very subtly, for example only as a nubbin on the ulnar side of the little ( pinky ) finger, or very distinctly, as a fully expanded finger. Most generally, the extra finger is important, consisting of an end phalanx with a nail, & connected to the hand with a small skin pedicle. The mostly neurovascular burden can be defined, with no tendons present in the extra digit. A triplication of the little ( pinky ) finger is very irregular. Ulnar polydactyly appears 10 times more often in African populations. The incidence in Caucasians is notified as 1 in 1,339 live births, compared with 1 in 143 live births in Africans & African Americans. Ulnar polydactyly is also usually part of a syndrome. The ulnar polydactyly primarily appears isolated, whereas the representation in Caucasians is commonly associated with a syndrome, though in a retrospective investigation, only 4 of 37 patients of ulnar polydactyly were syndromic.
Radial or preaxial polydactyly
Preaxial polydactyly
This is a less typical situation, in which the affectation is on the side of the hand towards the thumb. Radial polydactyly guides to the presence of an extra digit [ or extra digits ] on the radial side of the hand. It is most regular in Indian populations & it is the 2nd most common congenital hand condition. The incidence of radial polydactyly is registered as 1 in every 3,000 live births. The clinical features of radial polydactyly will rely upon the time of duplication. Radial polydactyly counters from a barely perceptible radial skin tag to terminate replication. Thumb polydactyly differs from the slightly visible broadening of the distal phalanx to the full reproduction of the thumb involving the 1st metacarpal. Radial polydactyly is repeatedly associated with many syndromes.
Central polydactyly
This is a very irregular situation, in which the extra digit is on the ring, middle, or index finger. Of these fingers, the index finger is numerous often involved, whereas the ring finger is rarely involved. This kind of polydactyly can be associated with syndactyly, cleft hand, & many syndromes. Polysyndactyly presents different degrees of syndactyly affecting fingers 3 & 4.
History and Physical
Patients with polydactyly may show in infancy or later & may occur in isolation or with other birth deficiencies. Polydactyly of hand & foot can be categorized into three main categories: preaxial, central, & postaxial. In 1995, the congenital hand board of the International Federation of Societies for surgery of the hand selected to change the terms preaxial & postaxial polydactyly to radial & ulnar polydactyly. Radial polydactyly involves the thumbs, & ulnar polydactyly affects little fingers. Central polydactyly contains the ring, middle, & index fingers.
The most typical type of polydactyly of hand is radial polydactyly, & the prevalence rate is higher in whites reached other ethnic populations. Most of the patients are sporadic & unilateral without any associated systemic problems. In some cases, the extra digits are noticed anterior to the thumb. Radial polydactyly was further categorized by wassel in 1969 into 7 subtypes, serially from type I to type VII, & it is used by hand surgeons very actually during the control of the patients. Ulnar polydactyly was organized by Temtamy & Mckusick into two classifications, type A & type B. The words radial, central, & ulnar are used to describe the polydactyly of the upper limb.
In contrast, the words tibial, central, & fibular are utilized to describe polydactyly of the lower limb. Polydactyly of the lower limb was categorized by Swanson based on the presentation of the extra digit on the foot. When the main 3 digits are involved, then it is named central polydactyly.
Epidemiology
Preaxial polydactyly
The situation has an assessed occurrence of 0.3 to 3.6 per 1000 live births. Postaxial hand polydactyly is most systematic in the United States in black males. Preaxial polydactyly happens in 0.08 – 1.4 in 1,000 live births. In the United States, it is more common in white people & also somewhat frequent in Native American & Asian people.
Diagnosis
Right-sided reproduction of the right little toe in an 8.5-month-old male, with two toes [ fifth & sixth ] forming joints with the 5th metatarsal bone, which is mildly enlarged distally. The reproduced toes have almost normal growth. The 5th toe has gentle varus angulation, & the 6th toe has significant valgus angulation.
X-ray of type 3 central polydactyly [ the middle fingers are the same size ].
Classification is achieved by using x-ray imaging to see the bone structures.
Ulnar polydactyly
Type 1 ulnar polydactyly: an extra digit is connected by skin & nerves.
The variety of ulnar polydactyly exists in either 2 or 3 types. The two-stage classification, according to Temtamy & McKusick, involves types A and B. In type A there is an additional little finger [pinky finger] at the metacarpophalangeal joint. The little ( pinky ) finger can be hypoplastic or fully evolved. Type B varies from a nubbin to an extra, nonfunctional little [ pinky ] finger part on a pedicle. According to the type 3 classification:
Type I contains nubbins or floating little [ pinky ] fingers,
Type II contains reproductions at the MCPJ,
Type III contains reproductions of the whole ray.
Radial polydactyly
The wassel type is the most accustomed classification of radial polydactyly, specified upon the most proximal group of skeletal reproduction. The most common type is Wassel 4 [ about 50% of such duplications ] followed by Wassel 2 [ 20% ] & Wassel 6 [ 12% ].
Central polydactyly
The variety of central polydactyly is founded on the extent of reproduction & affects the following 3 types:
Type 1: It is a central reproduction, not attached to the neighboring finger by osseous or ligamentous branches: it repeatedly does not include bones, joints, cartilage, or tendons.
Type 2A: It is a nonsyndactylous duplication of a digit and part of a digit with normal elements. The articulates with a broad or bifid metacarpal or phalanx.
Type 2B: It is a syndactylous duplication of a digit & part of a digit with normal components, & talks with a broad or bifid metacarpal or phalanx.
Type 3: It is a complete digital duplication, which has a well-formed reproduced metacarpal.
Differential Diagnosis
Polydactyly may be present in isolation or may be associated with the features of some syndromes involving the following:
- Trisomy 13
- Meckel syndrome
- Down syndrome
- Acrocallosal syndrome
- Basal cell nevus syndrome
- Diamond-Blackfan anemia
- Bardet-Biedl syndrome
- Biemond syndrome
- Fanconi anemia
- Ellis van Creveld syndrome
- McKusick-Kaufman syndrome
- Mirror hand deformity [ ulnar dementia ]
- Mohr syndrome
- Oral-facial-digital syndrome
- Pallister-Hall syndrome
- Rubinstein-Taybi syndrome
- Short rib polydactyly
- VACTERL: vertebral deficiencies, anal atresia, cardiac deficiencies, trachea esophageal fistula, renal abnormalities, and limb anomalies
Treatment of Polydactyly
Ulnar polydactyly
It generally does not interrupt with hand function, but for social reasons, it can minister operatively.
Type A ulnar polydactyly
The treatment of Type A ulnar polydactyly is complicated as it aims to release the supplement digit while keeping a stable, functional small finger. When the produced proximal phalanx communicates with a common, broad metacarpal head, the ulnar collateral ligament must be considered. In articulation with a 6th metacarpal the muscle functioning of the abduction of the pinky, [ little ] finger, means abductor digit minimi must be preserved. In patients with a common metacarpal articulation, an elliptical incision at the floor of the post-axial digit is made. This incision may be extended proximally to sufficiently expose the abductor digit minimi. The ulnar collateral ligament & the insertions of the abductor digit minimi are then advanced with a periosteal sleeve. The duplicated extensor & flexor tendons to the ulnar digit are transected & after that, the digit is amputated at its presentation with the metacarpal. At last, the collateral ligament & abductor digit minimi are reinserted at the base of the preserved proximal phalanx & a wire is then positioned across the reconstructed joint. In patients with a duplicated metacarpal, the additional digit is amputated in a common ray fashion with the transfer of the abductor digit minimi to the possessed small finger.
Type B ulnar polydactyly
In this situation, osseous & ligamentous structures are absent. The surgical technique is equal to radial polydactyly, in which the level of duplication & anatomical features should suggest operative therapy. The pedicled ulnar additional digit can be dismissed by suture ligation to make the skin bridge of the developing child. This might be more comfortable than the excision of the extra digit when the child is 6-12 months old. Ligation inhibits the vascular supply to the duplicated digit, resulting in dry gangrene & subsequent autoamputation. This must be done regarding the presence of a neurovascular bundle, truly in very small skin bridges. When the ligation is done inappropriately it can provide a residual nubbin. Also, a neuroma can evolve in the location of the scar. An excision can control the outcome of a residual nubbin & the acuity due to a neuroma.
For babies with ulnar type B polydactyly, the suggested treatment is ligation in the neonatal nursery. The excision of an extra digit in the neonatal nursery was a safe & simple procedure with adequate clinical & cosmetic work.
Radial polydactyly
Because neither of the 2 thumb parts is normal, a conclusion should be taken on combining which features to create the best possible composite digit. Rather than amputating the most hypoplastic thumb, the conservation of skin, nails, collateral ligaments & tendons is demanded to augment the residual thumb. Surgery is recommended in the 1st year of life, generally, between 9 & 15 months of age. Surgical options rely on the type of polydactyly.
Bilhaut-Cloquet procedure
This type of procedure is advised for Wassel types 1 & 2 in which both thumbs are severely hypoplastic by some congenital hand surgeons. The procedure includes a composite wedge resection of the central bone & soft tissue. This will be conducted with a process to the lateral tissue of each thumb. The purpose is to achieve a normal thumb, which affects the size, which is possible. If the width of the nail bed is more significant than 70% of the contralateral thumb, it may be shattered.
Ablation with collateral ligament reconstruction
This type of procedure is used for all wassel types of polydactyly & is the most generally used procedure. It is advised in all circumstances of thumb duplication with a hypoplastic, less-functional thumb. One could consider the Bilhaut-Cloquet. The ulnar thumb is preferably maintained as it is the more progressive one in most cases.
By dividing the radial collateral ligament from distal to proximal, a periosteal sleeve can be carried. In this method, the radial collateral band of the radial digit will function as the absent radial collateral ligament of the maintained ulnar thumb.
A peak of the FPB & APB has been achieved in Wassel type IV duplication: this can be accomplished through the periosteum. As the tendons insert proximally, the ridge is completed proximally too to potentially rebalance the ulnar thumb. After the radial thumb is amputated, the ulnar aspects are centralized and fixed with a Kirschner wire. In most cases, a longitudinal & sagittal osteotomy is required to centralize the bony parts of the ulnar thumb. While the soft tissue of the radial thumb was maintained, it is now connected to the radial side of the ulnar thumb together with the periosteal sleeve. The APB & FPB of the ablated radial thumb is connected to the distal phalanx for more stability. If required, the extensor pollicis longus & the flexor pollicis longus are reattached to centralize their course.
In Wassel types 5 & 6 the opponens pollicis muscle must be moved to the ulnar metacarpal. Soft tissue with collateral ligament reconstruction is used to bypass angular malformation in the preserved thumb. Tendon centralization is also usually used for correction. Still, patients with osseous malformations may happen. To provide alignment, osteotomies are required to be done. This operation may require bone grafting, which is received from the amputated thumb.
On top plasty procedure
This type is suggested when one thumb is more extensive proximally & the other thumb has a larger distal component. [ The approach is initially described as a way to lengthen amputated digits ]. The purpose is to create a functional thumb by connecting less-hypoplastic elements. On top plasty process is infrequently employed in the treatment of congenital thumb duplication. It might be required for Wassel types 4, 5, and 6.
At the level of the mid-proximal phalanx and mid-metacarpal, the distal part is moved to the proximal component. The tendons of the distal part are preserved as the remainder of the distal part is amputated. The neurovascular bundle which provides the distal part is reserved & transferred proximally.
Central polydactyly
Early osteotomy &ligament reconstructions should be done to control malformations, such as angular growth deformations.
The surgical therapy of central polydactyly is highly unstable. After the surgery, the hand must be available & stable, but also aesthetically pleasing. This needs intraoperative creativity & flexibility. In difference, a functional, 4-fingered hand achieved through ray amputation may be preferable to a 5-fingered hand with a malformed or stiff reconstructed finger.
Cases of polysyndactyly are approached via a standard opposing zig-zag incision. The incision is partial to the accessory digit, preserving extra skin for the subsequent closure. Relying on the level & extent of duplication, the flexor & extensor tendons may need centralization or rebalancing. Also, the collateral ligaments must be maintained or reconstructed. Broad articular surfaces should be tightened & phalangeal wedge osteotomies may be needed to give an axial alignment. Attention must also be provided to reconstruct the intermetacarpal ligament. Also, one should take in mind the requirement for sufficient web-space soft tissue.
Deterrence and Patient Education
Polydactyly may transfer throughout generations by an autosomal dominant way of inheritance. If the parent holds the trait, both male & female children bring the risk of inheriting the condition. Parents should be apprised about prenatal ultrasonography to notice polydactyly of the fetus & screening for other fetal abnormalities.
Enhancing Healthcare Team Outcomes
The diagnosis & administration of polydactyly usually needs an interprofessional team approach with healthcare providers such as geneticists, neonatologists, primary clinicians, & surgeons. Clinicians must discuss with parent’s family history & advise them properly about all the possible outcomes of the newly analyzed baby. Neonatal health care workers also have to advise those homes with familial reproduction of polydactyly for taking genetic counseling concerning their risk examination.
Prognosis
Ulnar polydactyly
Type A ulnar polydactyly
There are no substantive effect studies concerning the function of these hands following surgical intervention. This is caused by the fact that there is a normal part of these patients’ hand ablation with collateral ligament reconstruction. In a study on 27 patients experiencing surgical excision for Type A ulnar polydactyly, only one difficulty was noted in the form of an infection. However, no experimenters have objectively reviewed the functional range of motion [ ROM ]or articular stability.
Type B ulnar polydactyly
In a study on 21 patients with Type B ulnar polydactyly regaled with suture ligation, it was found that the duplicated digit was generally amputated at an average of ten days & no complications of infection or bleeding were noted. In a large study on 105 patients regaled with suture ligation an overall difficulty rate of 23.5% was reported, citing a residual tender or inappropriate bump in 16%, infection in 6%, & bleeding in 1% of patients. Parents should be enlightened as to the progression of necrosis, & that revision of residual tissue and scar may be required when the child is 6 months of age or older.
Radial polydactyly
Bilhaut procedure
Advantages: By connecting two hypoplastic thumbs adequate thumb size is received. Furthermore, the IP & MCP joints are very durable as the collateral ligaments are not disregarded during reconstruction.
Disadvantages: Violation during reconstruction can cause growth arrest or asymmetric growth. Nail disfigurement could also happen after reconstruction. Although the joints are stable, limitation of flexion may be possible. The intermediate IP flexion in a reconstructed thumb is 55 degrees less than in the contralateral thumb. MCP flexion averaged 55 degrees in reconstructed thumbs, which corresponded to 75 degrees in the contralateral thumb.
Ablation with collateral ligament reconstruction
Advantages: The reconstructed joints manage to remain flexible. Also, it preserves the nail bed & physis, this increases the deterrence of nail deformations over time.
Disadvantages: Obtain a stable thumb of appropriate size, fluctuation of the IP & MCP joint arise, as well as a size mismatch. Thumbs are characterized as unacceptable if IP joint deviation surpasses 15 degrees, MCP joint deviation exceeds 30 degrees, & thumb size is unsuitable based on the examiner’s assessment. Also, a thumb size 1/3 greater or less than the contralateral thumb is described as unacceptable.
On-top plasty procedure
No surgical results studies exist for considering the function of the thumbs after an on-top plasty reconstruction.
Central polydactyly
Few clinical development studies exist concerning the treatment of central polydactyly. In Tada’s study, 12 patients were examined. All patients required secondary surgical procedures to address flexion contractures & angular variation at the IP joint level. However, many primary aspects contribute to the complicatedness of central polydactyly reconstruction. That’s why, treatment completely relies on the anatomic deformities present, the degree of severity of syndactyly, & the function of the duplicated finger.
Complications
In polydactyly of the hand, bleeding & anesthetic difficulties may occur during the perioperative period. Functionality can be reduced later due to contracture or ligamentous laxity. A painful neuroma is another difficulty, specifically when using suture ligation, & it occurs at the treatment site. Beneath the suture ligation site, painful neuroma forms because the digital nerves of the additional digit are cut off at the skin level, so it cannot abandon the soft tissues. As a result, the children are prone to damage to the skin tag resulting in skin breakdown.
In polydactyly of the foot, hallux varus is the most typical difficulty of tibial polydactyly that may cause a successive surgical correction.
FAQ
Postaxial polydactyly: An extra little finger or toe provider might guide the baby’s polydactyly with other terms. Providers sometimes guide to additional big toes as tibial polydactyly & extra little toes as fibular polydactyly.
It might be incredible to see an extra finger or toe after the baby is born, but polydactyly is incredibly treatable. The child will have no long-term effects from having the extra digit withdrawn, & polydactyly doesn’t mean they’ll have any other developmental difficulties.
Some of the causes for polydactyly or additional fingers in infants are Carpenter syndrome,
Patau syndrome
Jeune syndrome
Polydactyly could be of 3 types: preaxial, central, & postaxial polydactyly. It can be analyzed during prenatal & postnatal ultrasounds and an X-ray.
Sometimes, polydactyly is interpreted during the first three months of pregnancy. This is done using an ultrasound and embryo fetoscopy. Cure relies on which type of disease a person has, Small finger duplication may not need treatment, as it does not normally impact how people can use their hands.
The feedback provided will help us show more appropriate content in the future. Polydactyly (additional digits) overall runs about one in 500 live births. There are considerable variations by location & genetic background. The extensive majority of people are born with six or more fingers.
The medical word for having additional fingers or toes is called “polydactyly”. Often they are not fully formed, but sometimes they are. Preaxial or radial polydactyly results in extra thumbs, central polydactyly adds middle fingers, & postaxial or ulnar polydactyly.


2 Comments