Clubfoot (Congenital talipes equino Varus)
Table of Contents
What is a Clubfoot?
Clubfoot describes a range of foot abnormalities generally present at birth (congenital) in which the baby’s foot is twisted out of shape or position. In clubfoot, the tissues incorporating the muscles into the bone (tendons) are shorter than normal. Clubfoot is a fairly normal birth defect and is generally an isolated problem for an otherwise healthy newborn.
- Clubfoot may be mild or severe.
- About fifty percent of children with clubfoot have it on both feet. If the child has clubfoot, it will make it harder to walk normally, so doctors suggest treating it soon after birth.
- Clubfoot can be unilateral (30%-40%) or bilateral (60%-70%).
- It is twice as usual in men than in women.
- It is the most usual congenital malformation of the foot affecting 1-2 newborns per 1000. Most frequently it is an isolated abnormality, but sometimes it is connected with other congenital malformations or syndromes.
- It is also known as talipes equinovarus deformity.
- Talipes Equinovarus comes from the following:
“Tali” means Ankle,
“Pes” means Foot.
“Equinus” means foot pointing downside (like a horse’s foot).
“Varus” means deviated towards the midline.
When clubfoot is congenital, It is also called CTEV means congenital Talipes Equinovarus.
Epidemiology
- Clubfoot is more usual in males with a 2.5 to 2.8:1 Male: Female ratio.
- So many cases have been noted between countries and regions ranging from 1-1.50 per 1000 live births, rising up to 3 per 1000 live births.
- Likewise, ethnic differences in events have been reported with the lowest incidence (0.6%) among the Chinese Population, and the highest incidence (6.8%) in the Polynesian Region.
- The accumulative incidence is supposed 1 per 1000 live births among Caucasians.
- Worldwide 80% of babies born with clubfoot are in low-and middle-income countries.
What are the Causes of Clubfoot?
- In an estimated 80% of cases, clubfoot is idiopathic.
- The remaining 20% is present in alliance with other disorders, most usually Spina Bifida, Cerebral Palsy, and Arthrogryposis. Incidence of clubfoot varies worldwide from an estimated 0.39/1000 live births in the Chinese, 1-2/1000 in Caucasians, and can be as high as 7-8/1000 in Polynesians.
- Birth generality has been reported as differing between 0.51 and 2.03/1000 live births in LMICs.
- The causes of clubfoot are badly understood.
- There is almost certainly a genetic component and environmental factors, seasonal variation, and in-utero positioning have all been recommended as possible causal factors but these have not been frequently demonstrated.
- In some countries and cultures, there are various beliefs about what causes a child to be born with clubfoot.
- These include spiritual influences, spells, or curses frequently leading to mothers being blamed for the deformity.
- These ideas can cause the baby with clubfoot to be kept out from society, so therefore it is important to explain to families that children with clubfoot are an important part of society.
What are the Symptoms of Clubfoot?
The foot is made up of 26 bones. Most applicable for this congenital deformity are the Talus, Calcaneus, and Navicular. The underlying deformity of clubfoot can be most simply understood if it is parted up into 4 components, whose foremost letters make up the word CAVE. These elements are Cavus, Adductus, Varus, and Equinus. The Cavus and Adductus deformities resulted in the midfoot, while the Varus and Equinus deformities happen in the hindfoot.
Cavus
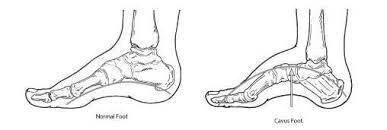
- The midfoot is the initial part of the deformity of the clubfoot.
- The arch of the foot is elevated than normal.
- The result of the first metatarsal is plantarflexed in relation to the calcaneum and hindfoot.
Adductus
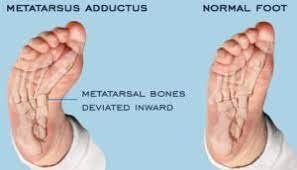
- It is the movement toward the midline.
- Adductus is the secondary part of the clubfoot deformity.
- The forefoot is adducted towards the midline.
- This is the subsidiary part of the deformity of clubfoot.
- The navicular moves medially and initiates to dislocate off the talus.
- The calcaneum as well rotates medially under the talus as part of the adductus deformity.
Varus
- It means moving toward the midline.
- The Varus of the hindfoot is the tertiary part of the deformity of clubfoot.
- The heel is in varus in contact with the tibia.
Equinus
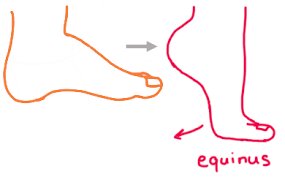
- It means an elevation in the plantar flexion of the foot.
- The entire foot spike downwards in relation to the tibia.
- Equinus of the hindfoot is consequently the fourth part of the clubfoot deformity.
- The deformity includes equinus/plantarflexion at the ankle merged with adduction and inversion at the subtalar, midtarsal, and anterior tarsal joints.
- Clubfoot may be described as a “congenital dislocation of the Talo-Calcaneal-Navicular (TCN) Joint.
- The navicular moves medially on the talus in clubfoot, at the time the calcaneum rotates under the talus in clubfoot.
- The foot is situated in adduction and inversion by ligaments and muscles.
- Muscles that are shrinked are triceps surae, tibialis posterior, flexor digitorum longus, and flexor hallucis longus.
- Further, there is an imbalance between the inverter-plantar flexor muscles and the inverter-dorsiflexor muscles.
- The calf and peroneal muscles are generally poorly developed.
- Weaker peroneal muscles permit the foot to be inverted.
- The ligaments of the posterior and medial aspects of the ankle are thick and taut.
Classification
Not all Clubfeet are the same and it is necessary that all individuals treating clubfoot use the same terms to describe the different types. Each type of clubfoot has a unique quality and can need specific treatment. Early identification of the type of clubfoot one is dealing with may help guide appropriate treatment. Although there is no universal classification system for clubfoot, clubfoot may be classified depending on the nature of the deformity:
Positional Clubfoot
- Positional clubfoot mention to a flexible foot that was held on to overtime in an abnormal position in utero.
- When the child is born, because of the prolonged positioning, they can present with one or both feet in an atypical resting position.
- Children with positional clubfoot usually exhibit an unrestricted passive range of motion of the forefoot and ankle.
- The foot at the duration of birth has some deformity. Still, bony alignment is not affected and foot position is likely corrected through conservative treatment including a program of stretching, range of motion, and weight bearing.
- In a little number of cases post conservative treatment the foot needs 1 or 2 Casts to ensure they are maintained in a perfect position although in the majority of cases these feet generally correct well and do not lead to any long-lasting, significant impairment.
Idiopathic Clubfoot
- Usually, clubfoot is classified as “Idiopathic Clubfoot” meaning there is no identified cause for the deformity.
- In idiopathic clubfoot, there may also be a definite hereditary effect, in that if a person has a relative, parent, or sibling who has clubfoot, then they are more likely to have clubfoot or have a baby with it (4-10% chance).
- Within the group of idiopathic clubfoot, there is a wide spectrum of disabilities dependent on severity, as well as whether the clubfoot has been untreated, partly treated, poorly treated, or successfully treated.
Untreated Clubfoot
- All clubfeet from birth up to 2 years of age that have had very little or no treatment may be considered untreated clubfeet.
Treated Clubfoot
- Untreated clubfeet that have been put right with Ponseti treatment are termed “treated clubfeet”.
- Treated clubfeet are generally braced full-time for three months and at night up to age 4 or 5 years.
Recurrent Clubfoot
- This is a clubfoot that has achieved a great result with Ponseti treatment, but the deformity has recurred.
- The ordinary reason is because of abandoning the braces early.
Neglected Clubfoot
- The neglected clubfoot is a clubfoot in a child older than two years, where little or no treatment has been performed.
- The neglected clubfoot can respond to Ponseti treatment, but also can have a bony deformity that needs surgical correction.
Complex Clubfoot
- Any foot with a deformity that has received any treatment other than the Ponseti method can have added complexity due to additional pathology or scarring from surgery.
Resistant Clubfoot
- This is a clubfoot where Ponseti treatment has been accurately performed but there has been no significant improvement.
- It is generally found that this kind of clubfoot is not in fact idiopathic after all and is secondary or syndromic.
Atypical” Clubfoot
- This is a kind of clubfoot dealt with in the advanced section of this course.
- It involves a foot that is frequently swollen, has a plantarflexed first metatarsal, and an extended big toe.
- It may take place spontaneously but most generally happen after the slippage of a cast.
Secondary Clubfoot
- Additionally, happens when there is another disease or condition that is causing or linked to the development of clubfoot.
- Such conditions are generally Neurological like Spina Bifida connected with concurrent sensory and or motor impairments or Syndromic Disorders like Arthrogryposis connected with more global findings and involvement of other musculoskeletal issues.
Who is at risk for congenital clubfoot?
Boys are up to twice as likely to evolve clubfoot as girls are. Having a hereditary history of clubfoot also puts the baby at higher risk.
Children are also at higher risk if they have:
- Some other birth defects, like spina bifida or cerebral palsy.
- A genetic disease, such as Trisomy 18 (Edward syndrome).
- A woman can be at higher risk for having a baby with clubfoot if she had oligohydramnios at the time of pregnancy.
- This is a problem of not having sufficient amniotic fluid, the fluid nearby the baby, and also Zika infection at the time of pregnancy, which may lead to birth defects and other problems.
- Smoked, drank alcohol, or used illegal drugs at the time of pregnancy.
Diagnosis
- Clubfoot is usually identified antenatally, by ultrasound scan, or at birth.
- The examination after birth consists of taking the foot and manipulating it slowly to see if it may be brought into a normal position.
- If not, there is a positive identification of clubfoot.
Prognosis
- The prognosis can be dependent on when treatment begins.
- When treatment is starting earlier the child starts weight bearing, and the chances of victorious treatment and relatively ‘normal’ foot function are greater Patients wearing the Foot Abduction Brace also come up with a good prognosis, by preventing relapse.
- In younger children, some can achieve partial, or even full correction with the Ponseti treatment.
- In others, a period of casting following the Ponseti principles can require to be supplemented with surgery to gain full correction of the foot position.
There are some Exercises to Treat Clubfoot at Home
The doctor can advise you on some simple exercises that can be done at home to treat the baby’s clubfoot. They are:
Metatarsus Adduction (stretching instep out)
- To perform this exercise, put the left hand on the inside of the baby’s foot.
- Place the fingers of the right hand between the toes and slowly stretch the front side of the foot (with the toes) downwards, away from the heel.
- Hold it for 10 to 15 seconds and bring it back to its normal position.
Ankle Plantarflexion (foot goes down)
- To perform this exercise, hold the baby’s heel and ankle with the left hand.
- Put the right hand above the foot.
- Slowly push the midfoot and toes down using the palm of the right hand while the left-hand holds the heel in place.
Ankle Dorsiflexion (foot goes up)
- To perform this exercise, hold the baby’s heel with the right hand.
- Slowly pull the calf muscles down using that hand.
- Put the left hand in the middle of the back of the baby’s foot and gently push it towards the heel.
Toe Stretches
- For this exercise, make the baby lie down and slowly pull his toe one by one while keeping the ankle and heel at 90 degrees.
Strengthening Exercises
- To strengthen the baby’s muscles, slowly tickle the toes, calf, and backside of the foot of the baby.
- The baby will respond to it by lifting his leg and stretching the muscles.
- Repeat it ten times.
Treatment of Clubfoot
Too many various kinds of treatment methodologies for clubfoot have been used but since the 1970’s. the Ponseti Method of treatment has grown in favor and has completely put back the previous methods of treating clubfoot in many countries, which include a mix of surgical and conservative techniques. Ponseti Method incorporates 2 equally important phases: the Corrective and Maintenance Phases.
Corrective Phase
- During this phase the position of the foot is usually corrected using a series of manipulations and plaster of Paris casts, then finally a tiny outpatient procedure is taken place to cut the Achilles tendon (tenotomy).
- The corrective phase usually takes 6–8 weeks and the child is seen weekly for treatment.
Maintenance Phase
- Once the corrective phase has achieved a great position for the foot, the treatment is not over as the foot will tend to return to its deformed position, so the goal of the maintenance phase includes keeping the corrected position for the next 4–5 years.
- This is achieved by placing the child’s feet into a brace for 23 hours a day for the first 12 weeks.
- Then at night-time until 5–6 years old.
- The Ponseti Method is not that tough, cost-effective treatment that has become universally used around the world.
- Too many research studies in nations across the globe in the last 20 years have shown that in more than 90% of cases of newborn babies with idiopathic clubfoot, it may be treated successfully with the Ponseti technique.
- The Ponseti Method’s effectiveness is backed up by a large and growing body of evidence and has now become the treatment of choice for clubfoot.
The goals of treatment
To have functional, pain-free feet
Wear normal shoes
To avoid permanent disability
At the time of the Ponsetti Management of Clubfoot, there are Ten Key Messages to keep in mind:
- Assess, Plan, and Treat.
- Constantly stay in touch with Parents from the Start (Especially about Braces!).
- Correct First then Maintain.
- Correct Cavus First.
- Never Touch the Heel.
- TWO People to Cast.
- Toe to Groin Casts.
- In most cases, Tenotomy is required.
- Cover the Talus before Tenotomy.
- continuously Talking to Parents – they are key to maintaining correction through good adherence to Bracing!.
Exercise Stages After Ponseti Method
Stage 1
Full-Time Boots and Bar. The baby will wear the boots and bar for 23 hours a day after. The final cast is removed. We recommend that you do exercises with your child during the hour that he or she spends out of the brace. Although stretching is not part of Dr. Ponseti’s original protocol, it is obtaining extensive acceptance as a very useful part of the treatment process. Stretching may help the child’s foot stay flexible by maintaining the correction that was achieved after casting and tenotomy.
Massaging the Foot
- After the cast is removed, the baby’s foot might be sensitive to touch.
- Throughout the hour that the child spends out of the boots and bar, you should gently massage the foot with lotion or cream.
- Apply different strokes (e.g., tapping, tickling) and surfaces (e.g., cotton balls, washcloths) to rub the foot.
- This will help desensitize the foot.
Stimulating the Muscles
- Due to the original clubfoot deformity, the muscles that pull the baby’s foot in and down are stronger than the ones that pull it.
- out and up.
- To help balance the strength of these muscles, stimulate the outside border of the baby’s foot and watch it fan out and up!
Stretching within Abduction and Dorsiflexion (Out and Up)
- Stretch the child’s foot out (i.e., abduction) and up (i.e., dorsiflexion) when the child.
- Spends time out of the boots and bar.
- Think about how the last cast glance, and try to stretch the foot into the same position.
- Hold the stretch for thirty seconds and repeat five times.
Stretching Into Plantar Flexion (Down)
The muscles on the front of the baby’s ankle might become tight because of the amount of time that the child must spend in a cast to correct the clubfoot deformity. It is necessary to stretch these muscles so that your child will be able to achieve a full toe-down foot posture.
- To stretch the child’s ankle, place one thumb across the child’s lower shin (just above the ankle joint) and the other thumb across the midfoot.
- Push down on the child’s foot to stretch it into a toe-down posture.
- Hold the stretch for 20 seconds and repeat it five times.
- If the baby is consistently pulling a foot out of the boot or if the child develops a sore, you need to contact the clinic as soon as possible to make an appointment.
- If the baby does not have a sore or if the boots and bar are not making the sore any worse, please try to reapply the boots and bar until the appointment.
Stage 2
Wearing the Boots and Bar at Night time and During Naps. After 3 months of full-time wear, the child will then graduate to the nights and naps stage. You should continue to do the stretches and strengthening exercises that will help the child’s feet as they grow. If you notice that the child’s foot is becoming stiff or regressing towards the original clubfoot appearance, perform these stretches three times a day and call to make a clinic appointment as soon as possible.
Stretching the Achilles Tendon
- With the child’s knee straight, cup your child’s heel in the palm of the hand.
- Pull down on the heel as you use the other hand to push up on the midfoot (be careful not to push up on the toes).
- Hold the position for 20 seconds and repeat five times.
Playing in a Squat Position
- Once the child is walking, encourage him or her to play in a squat position with both heels flat on the floor.
- This position stretches the calf muscles and keeps the ankles and feet flexible.
- As the child becomes older, encourage him or her to jump like a frog, walk like a bear, and waddle like a duck!
Strengthening the Muscles
- As the child grows, it is too much important to strengthen the muscles that pull the foot up and out.
- Help to activate these muscles by placing the finger near the outer edge of the foot and asking the child to use his or her toes to touch your finger.
Alternative Exercises
- Another way to strengthen the muscles is to play in a sandbox or a plastic tub with a bottom full of sand.
- Have the baby sit with his or her heel down in the sand and then use the foot to sweep the sand outwards.
- The child can use this motion to build mountains of sand and then stomp through them afterward! Using the foot to draw pictures in the sand is also great fun.
- The child may make pictures of rainbows by using a windshield-wiper action and big outward movements of the foot.
- Ask the child to try to keep the heel down in the sand while performing these movements.
- As a child ages, he or she may perform other strengthening exercises such as walking on heels and on the inside borders of the feet. When the child learns the alphabet, ask him or her to use the foot to draw letters in the air!
SURGERY
- Achilles Tendon Lengthening
- Tendon Transfer Surgery
- Reconstructive surgery
What are the risks of clubfoot surgery?
Risks of congenital clubfoot surgery include:
- Nerve injury.
- Infection.
- Bleeding.
- Stiffness.
FAQ
Clubfoot is caused by shortened Achilles tendon, which causes the foot to turn in and under. Clubfoot is twice as common in boy babies. Treatment is important to correct clubfoot and is generally done in two phases — casting and bracing.
Adjustment of the deformity is in the order of CAVE, i.e. the cavus is corrected first then comes after by the adductus, etc. At this point, there is often a residual equinus deformity that needs percutaneous Achilles tendon release which is performed in the hospital under a short general anesthetic.
These components are Cavus, Adductus, Varus, and Equinus. The Cavus and Adductus deformities happen in the midfoot, while the Varus and Equinus deformities happen in the hindfoot.
The Ponseti method is reportedly most effective for treating clubfoot in babies up to 9 years of age. Although, whether age at the start of treatment influences the rate of successful correction and the rate of relapse is unknown.
Neurogenic clubfoot is caused by a neurological condition, a condition that influences the nervous system (brain, spinal cord, and nerves).