
Cervical Dystonia
Table of Contents
What is Cervical Dystonia?
- Cervical Dystonia of the neck also termed Spasmodic Torticollis or the Wry neck, is a dystonic condition that refers to an abnormal, asymmetrical head or neck alignment, which might be due to many causes. The word torticollis is derived from the Latin words tortus for twisted or the collum for the neck.
- The most normal case will no have an obvious cause, or the pain or difficulty with turning the head generally go away after a couple of days, even without any specific treatment. This creates the neck muscles to spasmodically contract. If a person has cervical dystonia, the head twists or twists to 1 side with pain. It can also tilt forward and backward. Cervical dystonia might go away without any treatment, but there is a chance of recurrence.
- Cervical dystonia will happen to anyone. However, it is most probably diagnosed in people between the ages of 45 to 60. It is mostly seen in women than men.
- Cervical Dystonia is occurred because of a spasm of the Sternocleidomastoid Muscle unilaterally or bilaterally.
- There is no permanent cure for cervical dystonia. The disorder many times resolves without any treatment, but sustained remissions are uncommon. Injecting botulinum toxin injection into the painful muscles often decreases the signs or symptoms of cervical dystonia. Surgery might be necessary in a few cases.
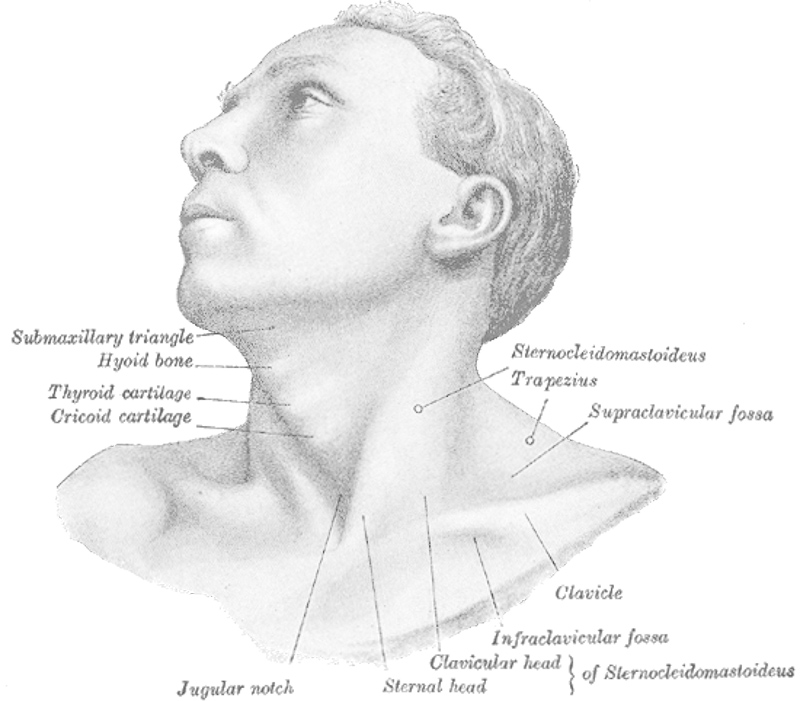
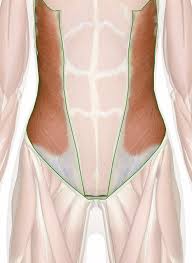
Anatomy of the Neck
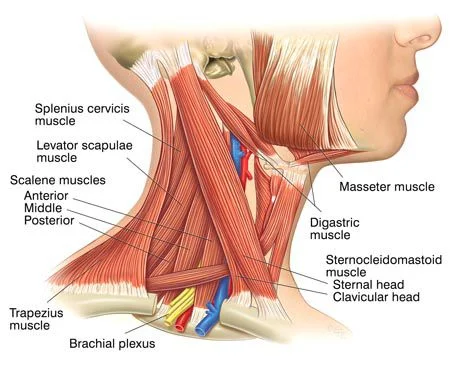
- The underlying anatomical distortion creating cervical dystonia or torticollis is a shortened sternocleidomastoid muscle. This is the muscle of the neck that arises at the sternum or the clavicle or ends in the mastoid process of the temporal bone on the ipsilateral or same side.
- There are 2 sternocleidomastoid muscles in the human body when they both contract, the neck is flexed in movement. The primary vascular supply for these muscles arrives from the occipital artery, superior thyroid artery, transverse scapular artery, or transverse cervical artery. The primary nerve supply to these muscles is from cranial nerve XI (the accessory nerve) but the 2nd, 3rd, and 4th cervical nerves are also included.
- Pathologies in these blood or nerve supplies can lead to torticollis.
Sternocleidomastoid muscle
origin
- Sternal head:
- superior part of the anterior surface of manubrium sterni
- Clavicular head:
- the superior surface of medial 3 of the clavicle
Insertion
- The lateral surface of the mastoid process of the temporal bone, the Lateral half of the superior nuchal line of the occipital bone
Nerve Supply
- The nerve supply of sternocleidomastoid muscle is by the accessory nerve (cranial nerve XI) & direct branches of the cervical plexus (C2 &C3).
Blood supply
- Superior thyroid artery & the external carotid artery
Actions
- Bilateral contraction: atlantooccipital joint/ superior cervical spine: head or neck extension; Inferior cervical vertebrae: neck flexion
- Unilateral contraction: cervical spine: neck ipsilateral flexion, neck contralateral rotation
- Sternoclavicular joint: elevation of clavicle or the manubrium of the sternum.
Signs and symptoms of Cervical Dystonia
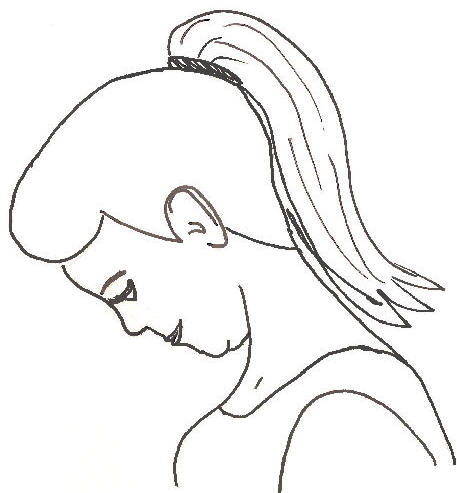
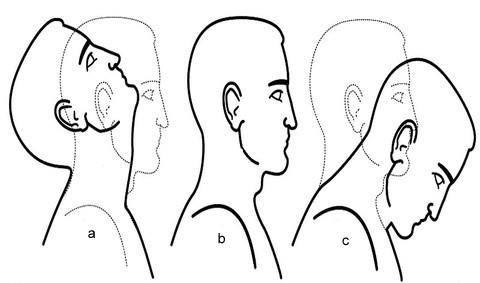
Cervical Dystonia is a fixed and dynamic tilt, and rotation, with flexion or the extension of the head or the neck. The type of Cervical Dystonia can be illustrated depending on the positions of the head or the neck.
- Rotational torticollis: the head rotates with the longitudinal axis
- Laterocollis: the head is tipped near the shoulder
- Retrocollis: hyperextension of the head or the neck backward
- Anterocollis: forward flexion of the head or the neck
A mixture of these movements may often be observed. Cervical Dystonia might be a disorder in itself as well as a symptom of different conditions.
Other symptoms include :
- Neck pain
- Decreased neck movement
- Tenderness on the cervical spine
- Thickened or tight sternocleidomastoid muscle
- Occasional formation of a mass
- Tremor in head
- Unequal shoulder heights
The muscle contractions included in cervical dystonia can cause the head to twist in a variety of directions, including:
- Ear toward shoulder
- Chin toward shoulder
- Chin straight down
- Chin straight up
- The most normal type of twisting situated with cervical dystonia is when the chin is pulled toward the shoulder. Some people experience a mixture of abnormal head postures. A jerking movement of the head also may occur.
- Many people who have cervical dystonia also feel neck pain that will radiate into the shoulders. The disorder can also be causing headaches. In some people, the pain from cervical dystonia might be exhausting or disabling.
Cervical Dystonia video
Which are the Causes of Cervical Dystonia?
- A multitude of conditions may lead to the development of Cervical Dystonia involving muscular fibrosis, congenital spine abnormalities, or toxic or traumatic brain injury. A rough categorization discerns congenital dystonia and acquired dystonia.
Other categories include:
- Traumatic
- Osseous
- Ocular
- CNS/PNS
- Idiopathic/Spasmodic
- Non-muscular soft tissue
- Congenital muscular dystonia
- Drug-induced
- Congenital muscular dystonia is the most common dystonia which is present at birth. The cause of congenital muscular dystonia is unclear. Birth trauma and intrauterine malposition might be considered to be the cause of damage to the sternocleidomastoid muscle in the neck. Other alterations to the muscle tissue originate from repetitive microtrauma within the womb and asudden alteration in the calcium concentration in the body which create a prolonged period of SCM muscle contraction.
- Any of these mechanisms might result in a shortening and excessive contraction of the sternocleidomastoid muscle, which reduced its range of motion in both rotation and lateral bending. The head typically is tilted in lateral bending near the affected muscle or rotated near the opposite side. In other words, the head itself is tilted in the direction nearer to the contracted and shortened muscle with the chin tilted in the opposite direction.
Congenital Cervical Dystonia :
- Congenital Cervical Dystonia is presented at one to fourth weeks of age, or a spasm of the SCM muscle or hard mass generally develops. It is commonly diagnosed using ultrasonography or a color histogram and clinically by evaluating the infant’s passive cervical range of motion.
- Congenital Cervical Dystonia contributes to the majority of cases seen in clinical practice. The diagnosed incidence of congenital torticollis is 0.3-2.0%. Many times a mass, such as a sternocleidomastoid tumor, is seen in the affected muscle at the age of two to four weeks. Gradually it is missed, usually by the age of 8th months, but the muscle is still fibrotic.
Acquired Cervical Dystonia :
- Noncongenital muscular Cervical Dystonia might result from scarring or disease of cervical vertebrae, adenitis, tonsillitis, rheumatism, enlarged cervical glands, retropharyngeal abscess, and cerebellar tumors. It can be spasmodic (clonic) and permanent (tonic). The afterward type might be due to Pott’s Disease (tuberculosis of the spine).
- A self-limiting spontaneously occurring form of torticollis with 1 and more painful neck muscles is by far the most general (‘stiff neck’) or it will pass spontaneously in one to fourth weeks. Usually, the sternocleidomastoid muscle and the trapezius muscle are included. Sometimes draughts, colds, and unusual postures are implicated; however, in many cases, no clear occurrence is found. These episodes are generally seen by physicians.
Tumors of the skull base (posterior fossa tumors) might compress the nerve supply to the neck or cause cervical dystonia or torticollis, or these problems are necessary to be treated surgically. - Infections in the posterior pharynx may irritate the nerves supplying the neck muscles or cause Cervical Dystonia or torticollis, these infections can be treated with antibiotics if they are not too severe or chronic but they could require surgical debridement in severe or intractable cases.
- Ear infections or surgical removal of the adenoids might cause an entity known as Grisel’s syndrome, a subluxation of the upper cervical joints, commonly the atlantoaxial joint, due to inflammatory laxity of the ligaments developed by an infection.
- The use of certain drugs, such as antipsychotics, may create Cervical Dystonia or torticollis.
Antiemetics – Neuroleptic Class – Phenothiazines - There are many numerous rare causes of Cervical Dystonia. A very very uncommon cause of acquired Cervical Dystonia is fibrodysplasia ossificans progressiva (FOP), the hallmark of which is malformed great toes.
Idiopathic Cervical Dystonia :
- Cervical Dystonia with recurrent, but transient contraction of the muscles of the neck or especially of the sternocleidomastoid, is termed idiopathic or spasmodic Cervical Dystonia. Synonyms are “cervical dystonia”, “intermittent Cervical Dystonia” or the “idiopathic cervical dystonia”, varies on the cause.
- Cervical Dystonia a common condition is also called spastic Cervical Dystonia. This causes the neck muscles to spasmodically contract. If you have idiopathic cervical dystonia, the head twists and twists to 1 side with pain. It can also tilt forward and backward. Cervical dystonia can go away without any treatment, but there is a chance of recurrence sometimes in severe cases where medications and physical therapy are not responding well, surgery might be required.
- Cervical dystonia may happen to anyone. However, it is most commonly diagnosed in people between the ages of 45 to 60. It also affects women mostly than men.
Trochlear Cervical Dystonia :
- Cervical Dystonia may be unrelated to the sternocleidomastoid muscle, instead caused by damage to the trochlear nerve (4th cranial nerve), which gives the superior oblique muscle of the eye. The superior oblique muscle is included in depression, abduction, or the intorsion of the eye. When the trochlear nerve is affected, the eye is extorted because the superior oblique is not working well.
- The affected person might have vision problems unless they rotate their head far from the side that is affected, causing intorsion of the eye or balancing out the extorsion of the eye. This can be diagnosed by the Bielschowsky test, also known as the head-tilt test, where the head is turned to the defected side. A positive test confirms when the affected eye elevates, seeming to float up.
Risk factors
Risk factors for cervical dystonia consist of:
- Age. While Cervical Dystonia can occur in people of any age, it most generally begins after the age of 30.
- The person’s sex. Women are more prone to develop cervical dystonia than men.
- Family history. If a close family member has cervical dystonia and some other type of dystonia, you are at a higher chance of developing the disorder.
Complications of Cervical Dystonia
- In some cases, the involuntary muscle contractions situated with cervical dystonia can spread to nearby areas of the body. The most prime locations include the face, jaw, arms, or trunk.
- People who have cervical dystonia may also have bone spurs that may decrease the amount of space in the spinal canal. This can be creating a tingling, numbness, or weakness in the arms, hands, legs, and feet.
Diagnosis of Cervical Dystonia
- Evaluation of a person with cervical dystonia begins with history taking to determine circumstances surrounding the birth or any possibility of trauma or associated symptoms. Physical examination reveals decreased rotation or bending to the side opposite from the affected muscle. is not occur by vision problems (IV cranial nerve palsy, nystagmus-associated “null position,” etc.).
- Physical Evaluation might include a thorough neurologic examination, or the possibility of associated conditions such as developmental dysplasia of the hip or clubfoot should be examined.
- Radiographs of the cervical spine should be done to rule out obvious bony abnormality, or MRI should be considered if there are serious structural problems and other conditions.
- Ultrasonography can be used to see muscle tissue, with a color histogram created to determine the cross-sectional area or thickness of the muscle.
- Evaluation by an optometrist and the ophthalmologist might be considered in children to ensure that the
Differential Diagnosis :
- Spasms nutans
- Cranial nerve IV palsy
- Myasthenia gravis
- Sandifer syndrome
Medical Treatment
Many types of oral medications are reported by the Dystonia Foundation to help for easing the symptoms situated with cervical dystonia. These consists of:
- Anticonvulsants, like topiramate (Topamax), are specifically used as a treatment for both epilepsy and migraine, or it has been reported successful use in treating the condition of cervical dystonia
- Dopaminergic, such as bromocriptine (Parlodel), levodopa (Sinemet), or amantadine (Symmetrel), block the neurotransmitter dopamine
- GABAergics, such as diazepam (Valium), which points to the neurotransmitter GABA-A
- Benztropine (Cogentin), or anticholinergics, such as trihexyphenidyl (Artane) block the neurotransmitter acetylcholine
Surgery
- Surgery is needed in severe or chronic cases, where medications and physical therapy are not responding well to the patient.
- Surgical treatment is the sterna or the clavicular heads of the sternomastoid are differentiated close to the beginning along with the release of the tight fascia. The head is afterward immobilized in a plaster cast in an over-corrected position for two to four weeks. Mobilization is start as soon as the cast is removed.
Botox Therapy for Cervical Dystonia

Introduction
- Botox (onabotulinumtoxinA) is a prescription brand name for the drug. It’s approved by the Food or Drug Administration (FDA) to treat cervical dystonia in adults. This movement disorder develops involuntary muscle spasms in the neck. You may also hear it termed “spasmodic torticollis.”
Here are the basics of Botox:
- Drug class: neurotoxin
- Active ingredient: onabotulinumtoxinA, which is a biological Trusted Source
- Available as biosimilar: no
- Drug form: in liquid solution form
The Goal Of Botox For Cervical Dystonia
- The Food or Drug Administration (FDA) has approved Botox for the treatment of cervical dystonia in adults. The aim of the treatment is to ease abnormal head positions and neck pain.
How the Botox is Working in Cervical Dystonia
- Botox is a type of drug called a neurotoxin. It works by exhibiting nerves from functioning.
- The nerves communicate with other parts of the body by using a neurotransmitter known as acetylcholine. (Neurotransmitters are chemical messengers.) Botox acts by preventing nerves from releasing acetylcholine. As a result, the nerves will not send messages to muscles telling them to contract or spasm. With cervical dystonia, Botox cures nerves from causing muscle contractions or spasms in the neck.
- Over time, the effects of Botox injections go down. This is because the nerves generate new endings that can begin releasing acetylcholine again.
How The Botox Is Given
- Botox arrives in a liquid solution. To treat cervical dystonia, the drug is given as intramuscular injections into the neck muscles. Only a healthcare professional will have permission for giving the botox injections, which you will receive during “treatment sessions.”
How Often It’s Given
- The doctor will suggest to you how often you will require to receive Botox injections for cervical dystonia. Relay on the findings of clinical studies, they may begin with the injections every three months. They may then make do settings depending on any side effects you have or how well the drug eases the symptoms.
- In a clinical study, people who received Botox for cervical dystonia noted that the effects seemed to go off about three months after their previous dose. Botox treatment appeared to be so much effective at relieving cervical dystonia symptoms six weeks after the injections were given.
Dosage of Botox
The dosage of Botox for treating cervical dystonia will rely on:
- the severity of the condition
- muscles affected
- the severity of pain you have due to the condition
- The doctor will identify the total amount of Botox that’s right for you. This will be differentiated into multiple injections for the affected muscle and muscles.
- The normal Botox dose for cervical dystonia in clinical studies was 236 units, given over the course of more injections to affected muscles. Usually, the doctor will begin you on a low dose, which they may increase, depending on how the body responds.
Precautions Before Receiving The Botox Therapy
- Before you use Botox Therapy, there’s some necessary key information to keep in mind. The botox drug might not be a safe option for you if you have some diagnosed medical conditions and other factors that affect your health. Some of these are mentioned under this.
Boxed Warning: Spread of Toxin Effects
- Botox had a boxed warning Trusted Source. This is the most critical warning from the Food or Drug Administration (FDA). A boxed warning alerts doctors or patients about drug effects that might be dangerous.
- On occasion, Botox may spread from where it’s injected to different parts of the body. This will result in botulism, a serious condition that may cause symptoms such as:
- difficulty breathing
- a lack of energy
- difficulty swallowing
- difficulty speaking
- double vision
- drooping eyelids
- loss of control over the bladder
- muscle weakness
- hoarse voice
- Botulism can occur hours, days, or weeks after a Botox injection is given. It’s quite serious to talk with the doctor if you experience any of the symptoms mentioned above while using Botox Therapy.
- In uncommon cases, difficulty breathing and swallowing might be life-threatening. People who already have trouble breathing and swallowing will be at higher risk of these problems.
Side Effects of Botox Therapy
- Like different medications, Botox injections might cause mild side effects. These side effects can be temporary, lasting a few days and weeks. But if they last for an extended time, and if they bother you or it becomes severe, it’s important to talk with the doctor and pharmacist.
Mild side effects of Botox injections for cervical dystonia will consist of:
- cough
- back pain
- flu-like symptoms, such as fever, muscle pain, or nausea
- dysphagia (trouble swallowing)
- neck pain
- headache
- upper respiratory infections, such as the common cold
- rhinitis (inflammation in the nose)
- dizziness
- vision problems
- muscle weakness and loss of strength
Serious Side Effects
Serious side effects from Botox injections might include:
- allergic reaction
- spread of toxin effects, which potentially could cause life-threatening breathing and swallowing difficulties.
Physiotherapy Treatment for Cervical Dystonia
- Physiotherapies treatments include such as stretching to release tightness, massage therapy to the sternocleidomastoid muscle, strengthening exercises to increase muscular balance, and handling to stimulate symmetry. A TOT collar is commonly applied. The early beginning of the treatment is very necessary for a full recovery or to reduce the chance of remission.
- Physiotherapy is a great option for treating cervical dystonia in a non-invasive or cost-effective manner. While outpatient cervical dystonia in babies’ physiotherapy is much more effective, Home therapy performed by a parent or any guardian is just as effective in reversing the effects of congenital cervical dystonia. It is necessary for physiotherapists to educate parents on the necessity of their role in the treatment or to create a home treatment plan along with them for better results for their child.
- 5 components have been recognized as the “first choice intervention” in physical therapy for the treatment of cervical dystonia or involved neck passive range of motion, neck or trunk active range of motion, development of symmetrical movement, environmental adaptations, or caregiver education.
- In therapy, parents and guardians should expect their child to be provided with these necessary components, Lateral neck flexion or overall range of motion can be achieved quicker in newborns when parents conduct physical therapy exercises a couple of times a day.
Cervical Brace For Cervical Dystonia

- A cervical brace is used to assist or protect the neck or spinal cord. These types of cervical braces are typically used for the treatment of cervical dystonia, neck injuries, neck surgeries, or some instances of neck pain.
- Cervical braces come in soft or hard varieties. The soft type of cervical brace is commonly used for acute cervical dystonia, and moderate neck pain, while the hard brace is typically used for severe neck pain, spinal fractures, or injuries.
- Although a cervical brace might be a useful tool for short-term treatment, it has been shown that wearing a cervical brace for a long period of time might lead to weakening or stiffening of the neck muscles.
Tips For Wearing A Cervical Brace
- If you require to wear a cervical brace, the healthcare provider will likely give you precise instructions about what you should or should not do while wearing it.
In common, when wearing a cervical brace, it’s best to:
- Move instead of resting and sitting much time. Slow movement, like walking, can help prevent the neck muscles from stiffening up. Stiff muscles may prolong the recovery.
- Focus on good posture. Try not to slouch and hunch over. Maintain the back straight, shoulders back, head straight with the ears positioned over the shoulders.
- Avoid sitting in soft, or low chairs. This might affect the posture or put unnecessary pressure on the neck.
- Avoid lifting and carrying anything heavy object. Also avoid strenuous activities, like running, and other high-impact activities.
- Leave the collar on at all times, except when cleaning it and as directed by the physical therapist or doctor provider.
- Make sure the collar fits tightly but is comfortable. If the collar will not fit tightly enough, it likely does not provide the assistance you need, which could cause more pain and injury. If it’s very loose, it could rub against the skin or cause irritation and blisters to the skin.
How Long Cervical Brace is Wear
- The length of time that a cervical brace is needed to wear depends on the severity of the condition.
- For moderate cervical dystonia pain that’s not caused by a sudden injury, it’s normally recommended that you do not wear a cervical brace for more than a week. Prolonged use of a cervical bracer can cause the neck muscles to stiffen or weaken.
- If a person is wearing a cervical brace for serious cervical dystonia and a sudden injury, talk with the physical therapist or doctor about how long you require to wear it.
Stretching Exercise for Cervical Dystonia
Table SCM Stretch
Instructions:
- Sitting in front of a table.
- Keep the chin in & down throughout this stretch.
- Place the left fist on the left side of the chin.
- Place the left elbow onto the table in front of you.
- Rest the weight of the head onto your fist.
- Tilt the head to the left.
- Apply more pressure to the chin to gear up the stretch.
- The goal is to feel a firm stretch on the right side of the neck.
- Hold for 30 secs.
- Perform on the alternate side.
SCM Stretch
Instructions:
- Tuck the chin in & downwards.
- Tilt the head to the right.
- Put the right hand on the opposite side of the head.
- Apply downward compression.
- Slowly turn the head to the left.
- The goal is to feel a firm stretch in the left Sternocleidomastoid.
- Hold for 30 secs, 3 rep.
- Repeat on the alternate side.
SCM Stretch Variation
Instructions:
- Place the fingers on top of the left collar bone.
- Pulling the skin down.
- Tuck the chin in & down.
- Slowly turn the head towards the left side.
- Tilt the head towards the right.
- The goal is to feel a stretch on the left Sternocleidomastoid.
- Hold for 30 secs, 3 rep.
- Repeat on the alternate side.
Chair Lean Stretch

Instructions:
- Sitting down on a chair.
- Using the right hand, grab onto the side of the chair.
- Keep the shoulder completely relaxed.
- Lean the body completely towards the left.
- Tuck the chin in & downwards.
- Tilt the head towards the left.
- Place the left hand on the right side of the head
- Apply downward compression.
- The goal is to feel a stretch on the right Sternocleidomastoid.
- Hold for 30 secs, 3 rep.
- Repeat on the alternate side.
Neck Elongation Stretch
Instructions:
- Tuck the chin in & downwards.
- Slide the head towards the right side.
- Elongate the right side of the neck in an upwards direction.
- The goal is to feel a stretch on the right side of the neck.
- Repeat on the alternate sides.
- Perform 30 reps, 3 rep.
Strengthening Exercise for Cervical Dystonia
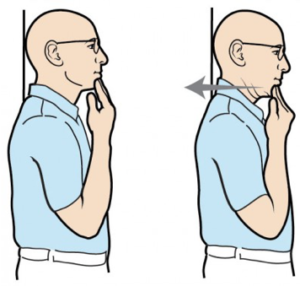
Chin tuck Exercise
- Sitting straight & look straight ahead with the ears parallel over the shoulders.
- Put two to three fingers on the chin.
- Stabilize the finger, pull the chin & head straight behind up to a gentle stretch is felt at the base of the head & top of the neck.
- Hold for 5 to 10 secs. Repeat seven to ten times.
Neck flexion Exercise (Neck tilt)
- In Relax sitting position flex the head down to rest the chin on the chest (Flex the neck fully).
- Gently tense the neck muscles & hold for 4 to 8 secs.
- Return to the initial position & repeat seven to ten times.
Neck extension exercise
- In Relax sitting position without arching the back, slowly move the head backward so you are looking upward.
- Hold for 5 to 10 secs. Return to starting position.
- This is a good exercise to do during working hours to prevent neck strain.
- Gently tense the neck muscles & hold for 5 to 10 secs.
- Return to a neutral position & repeat 10 times.
Neck flexion Exercise (side to side)
- Flex the head down towards the shoulder, & try to touch the shoulder with the ear (Without elevating the shoulder).
- Gently tense the neck muscles & hold for 8 secs.
- Return the head to a neutral position & repeat in the opposite direction.
- Repeat 10 times on both sides.
Neck Rotation exercise
- Rotate the head towards one side, keeping the chin at the same height & moving within comfortable limits.
- Gently stretch the neck muscles & hold for 8 secs.
- Return the head to the neutral position & repeat in the opposite direction.
- Repeat 10 times each on both sides.
Revolved Triangle Exercise

- Stand with the feet about four feet apart.
- Face the right toes forward & the left toes out at a slight angle.
- Square the hips & face forward in the same direction the right toes are pointing.
- Lift the arms up at the sides so they are parallel to the floor.
- Slowly hinge at the hips to fold forward, stopping when the torso is parallel to the floor.
- Bring the left hand to the leg, the floor, or a block, wherever you can reach.
- Extend the right arm straight up with the palm facing away from the body.
- Turn the gaze to look up toward the right thumb.
- Exhale to turn the neck to look down at the floor.
- Inhale as you return the gaze upward.
- Keep the rest of the body stable & continue these neck rotations as you stay in the pose for up to one min.
- Perform on the alternate side.
Upward Plank Exercise
- This pose allows you to passively hang the head back or down, and ease the tension in the neck or shoulders. This lengthens or stretches the SCM, chest, & shoulder muscles.
- Make sure the back of the neck is completely relaxed to avoid pressing the spine. If it is uncomfortable for you to let the head hang beside, you can tuck the chin into the chest & lengthen the back of the neck. Precise on engaging the neck muscles without straining.
- You can also allow the head to comfort back on some type of assistance such as a chair, a wall, or stacked blocks.
- How to do- Come into a seated position with the legs straight in front of you.
- Press the palms to the floor alongside the hips.
- Lift the hips & bring the feet under the knees.
- Deepen the pose by straightening the legs.
- Open the chest and & let the head drop back.
- Hold for up to 30 secs.
- Do this pose up to three times.
Prone Cobra Exercise

- This exercise is done by lying face downwards on the ground & uses gravity as resistance in the reinforcing process.
- Lying face downwards on the floor, put the forehead on a rolled-up hand towel for comfort.
- Place the arms by the side, and palms downwards on the ground.
- Touch the tongue on the upper palate of the mouth.
- Pinch the shoulder blades together & raising the hands off the ground.
- Roll the elbows inwards, palms outwards, & thumbs upwards.
- Gently raise the forehead about an inch off the towel keeping the eyes looking straight forward at the ground
- Hold the position for 7 to10 secs.
- Do10 repetitions.
Isometric Neck Exercise
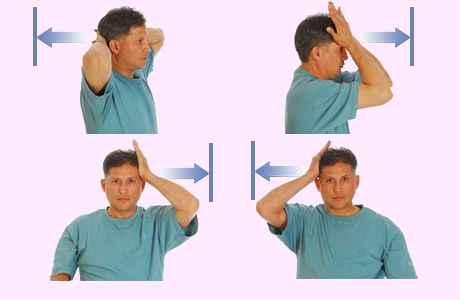
- Isometric neck exercise helps to strengthen the neck muscles. This exercise is commonly recommended by Physiotherapists from day 1st to relieve Neck pain.
Isometric Neck Exercise
How to perform this exercise In a sitting Position, - keep the Body in an upright erect position, Put both hands behind the neck (as seen in the images), or try the neck to push pressure on the hands or at the same time resist the neck muscles, both hands maintain align position for 4 to 5 secs or then relax.
The first day does 8 repetitions & the second day 10 repetitions. Do some exercise on the forehead & each side of the neck.
Do the exercise by pressing on the side of the head. Repeat 8 times, then alter sides.
Prone Rows Exercise

- Lie down on the stomach with the arms hanging off the side of the bed (managing angling the body so the head seems the corner of the bed).
- Use a pillow below the stomach for feeling better. Begin by pulling arms beside while bending elbows or squeezing shoulders blades combine then slowly return to the initial position.
- Do not lift the head up while pulling the arms back.
- Do repetition 20 times. Perform 2 times a day.
Standing pushups exercise

- Stand about an arms-length down from the wall with the bases spread piecemeal.
- Place the hands on the wall, making sure that they parallel with the shoulders.
- Keeping the reverse straight, sluggishly bend or flex the elbows, bringing the upper body toward the wall.
- Unbend or extend the elbows & return to the starting position.
- Repeat 20 times. Perform 2 times a day.

Lateral extension exercise
- Start by looking straight ahead. Slowly lean the head to the left side. Use the left hand for resistance, use the muscles in the neck to press against it. Hold for 5 to 10 secs, then return to the initial position.
- Then, slowly lean the head to the alternate side. Hold for 5 to 10 secs.
- Return to the initial position. Do 10 repetitions. This is a good exercise to do while in working hours, especially if you have to keep the head in a steady position for prolonged periods, as in working at a computer. Do this exercise every half hour to prevent neck strain.

Tilted forward flexion exercise
- Sluggishly lean the head to the leftism. Using the left hand for resistance, use the muscles in the neck to press against it. Hold for 5 to 10 secs, also return to starting position.
- Also, sluggishly lean the head to the other side. Hold for 5 to 10 secs.
- Return to starting position. Do 10 repetitions. This is a good exercise to do during work, especially if you have to keep the head in a steady position for a prolonged time as in working at a computer. Do this exercise every partial hour to help with the prevention of neck tightening.
Massage Therapy for Cervical Dystonia
Myotonic Release

- Objective: To decrease or eliminate contractures or adhesions found in the person’s SCM muscle. Contractures or adhesions in the SCM can result from chronic recurrence strain injuries, overuse injuries, whiplash, or other injuries to the muscles and other structures in the neck area.
- Positioning: Have the person lying supine, in a relaxed state. Stand at the head of the table, or passively bring the person’s head into a position of flexion, ipsilateral side flexion, or contralateral rotation. This will place the SCM in a maximally contracted or shortened position.
- Technique: First, ask the patient to help support the weight of his head for a few secs. This action will activate the SCM, allowing you to trace the muscle visually.
- Once you have visually traced the muscle, squeeze the inferior end of the muscle by placing it between the index finger or the middle finger.
- Begin to massage or strip superiorly together the length of the muscle, slowly moving near its joining site on the mastoid process, all the while, maintaining the squeeze pressure on the muscle.
- As you strip superiorly together with the muscle, slowly move the person’s neck into contralateral side flexion, ipsilateral rotation, or slight extension.
- This movement will lengthen the SCM while the strip is being performed.
- At the end of the myotonic strip technique, the contact hand would be on the superior end of the muscle at the mastoid process.
- Hold the contact at the end of the movement for approximately 3-5 secs. Repeat this stroke a total of 3-4 times.
- This myotonic technique is a very much effective technique in addressing contractures, adhesions, or trigger points in the person’s SCM muscles. In addition, this technique simultaneously adds a range of motion element to the joints in the cervical Spine, as well as to massage element to the SCM muscle itself.
Passive Stretch of the Sternocleidomastoid Muscle(SCM)
- Objective: To lengthen the SCM muscle. This will help decrease the pain from trigger points or muscle tension. As well, it will enhance the flexibility, strength, or overall functionality of the muscle by decreasing the contractures or adhesions, or by assisting in functionally realigning scar tissue that has been treated with friction massage methods.
- Positioning: As with more techniques for the SCM, the best positioning for a stretch to the person SCM is to have him once again, lying supine with his head in a normal position, or his neck muscles fully relaxed. As the therapist, you will start the technique by standing at the head of the table assisting the person’s head or neck with both hands.
- Technique: To massage the SCM muscle, gently bring the person’s head from the neutral position into a position of the same side or ipsilateral rotation, contralateral side flexion, or slight extension and start massaging in that direction. Make sure to perform this massage in a gentle, considerate manner, or within the patient’s pain tolerance. If the person feels pain, then you have gone too deep with the massage. Also, check in with the person during the stretch to ensure that he is respire properly. Hold this stretch for approximately 30 secs, or then slowly release the stretch by returning the patient’s head back into a normal position. Repeat this stretch a total of three times.
Ischemic Compression:
- Objective: To release the trigger points (hyperirritable bands in the muscle belly) in the sternal head of the SCM. Trigger points will occur in muscles because of the injury (to the muscle itself or to different structures in the neck region), and overuse. They are a source of local as well as referred pain, or they decrease the flexibility, strength, or overall functionality of the muscle.
- Positioning: Ask the patient to lie supine on the table, completely relaxed. To perform this ischemic compression to the SCM, the therapist should be standing (or seated) at the head of the massage table.
- Technique: First, trace the trigger point. To locate a trigger point in the SCM, feel the muscle to feel for a taut band and a twitch response in the muscle belly. (A common position of SCM trigger points is in the mid to inferior area of the muscle belly of the sternal head). Once you have traced the trigger point, apply an ischemic compression by slowly squeezing the trigger point between the thumb or index finger. The patient may feel referred pain surrounding the cheek or into the maxilla, over the supraorbital ridge above the eye, or deeper within the orbit of the eye. Keep in communication with the patient, checking to ensure that you are sustaining within the limits of his pain tolerance.
- Hold this technique for approximately 20 secs to 1 min, until the patient tells you the pain has diminished, and until you feel the muscle fibers begin to relax under the pressure. Once you feel this release, slowly release the pressure. Once you have released the pressure, apply a few effleurage strokes to flush out the area, or then follow up with a passive massage to the muscle.
Children with Cervical Dystonia
Nature of the deformity :
- The head is fixed inside flexion to the ipsilateral or same side (i.e, on the side of the affected muscle) while it is rotated to the other side. The shoulder on the affected side is elevated.
- Scoliosis with convexity to the sound side might be present in the cervical region. Facial asymmetry with a smaller eye or lowering of the corners of the mouth or an eye with a deviation of the nose on the affected side might be present. In uncommon bilateral affections, both the sternomastoid are shortened or contracted. The head is protruded forward with sustained kyphosis.
The basic objectives are :
- To correct the deformity by the release of the shortened and contracted soft tissues
- To hold the correction by suitable exercise regime; avoiding relapse.
Early stages – mild cases :
- Children along with a mild degree of deformity reporting early for treatment can be treated with physiotherapy.
The physiotherapy procedures are :
I. Evaluation: Careful evaluation of range of motion or the degree of deformity.
II. Massage: Massage will relax the muscle preceding the stretching maneuvers.
III. Hot Pack – Therapy Modality: Carefully administered thermo-therapy modality enhances relaxation.
IV. Relax Passive motions: The child is positioned in a supine position with the head beyond the edge of the table with the neck in extension by placing a pillow below the thoracic region; Shoulders are stabilized by a helper.
- To achieve relaxation, all the movements of the cervical spine are done in a form of gently relaxed passive motions.
- This should be followed by considerate passive stretching to the affected sternomastoid. E.g. when the left sternomastoid is involved the head should be gently bent inside flexion to the right, held there for a while, or then rotated gently to the left. Try to gain as much overcorrection as possible by applying gentle traction to gain furthermore stretching.
- Maintenance of Correction: Once the correction is done. It has to be held by passively holding and keeping a weight cuff.
- The same maneuver can be repeated during alternate visits.
- Active correction: Active correction is best done by supporting the child’s head to follow an object moving in the proper arc of correction. The bright-colored sound-producing things are ideal to grab the child’s attention.
- PNF: patients with neck extension can be used to benefit with an emphasis on stretch or traction
- Home treatment program: This assumes a primary role as these manipulations require to be repeated. The mother should be educated properly for this. The best method is to put the child prone or teach the mother to precisely move the head nearer the affected side or the child is encouraged to look behind over the right shoulder.
- Positioning: Exact positioning of the head during sleep is necessary. The child should be made to sleep on the different side of the lesion or the position of the head adjusted by a pillow and sandbag in a maximally corrected posture during the sleep. This positioning has 2 advantages:- 1st, there is organic relaxation of the muscle- 2nd, whatever correction is achieved, it is held for a longer period during sleep. However, the mother should frequently check the correction.
- Older children or adults: With advancing age the deformity gets organized or does not get managed by conservative management which requires surgery.



2 Comments