Dorsiflexor muscle of Foot: Anatomy, Origin, Insertion, Function, Exercise
Table of Contents
Introduction
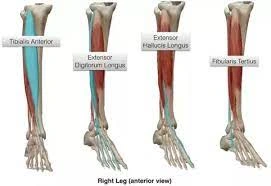
- The foot & ankle dorsiflexors include the tibialis anterior, the extensor hallucis longus (EHL), & the extensor digitorum longus (EDL). These muscles help the body clear the foot during the swing phase & control plantarflexion of the foot on heel strike. It acts to dorsiflex & invert the foot. This muscle is mostly situated near the shin.
- The dorsiflexor muscle is supplied by the deep fibular nerve (L4, L5), a branch of the common fibular nerve. The body of the muscle is entirely blood supplied by the branches of the anterior tibial artery; anterior muscular, medial muscular branches & anterior tibial recurrent artery.
- The primary function of the dorsiflexor is dorsiflexion, paralysis of this muscle results in foot drop, & an inability to dorsiflex. This paralysis can be caused by nerve injury, like direct damage to the deep peroneal nerve, & a muscle disorder, like ALS. “Foot drop” is often most common during gait when the patient cannot clear their foot during the swing phase.
Tibialis anterior muscle
Introduction
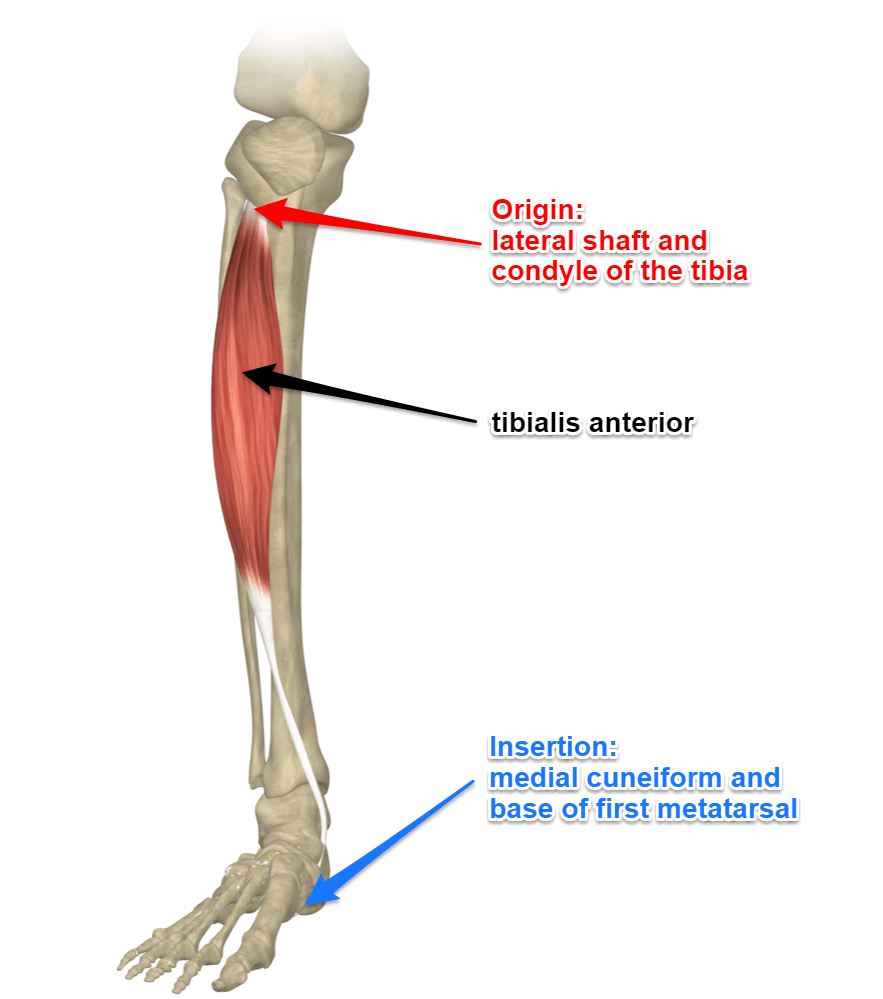
- The tibialis anterior is a muscle in humans that originates along the upper two-thirds of the lateral surface of the tibia & inserts into the medial cuneiform & first metatarsal bones of the foot. It acts to dorsiflex & invert the foot. This muscle is mostly situated near the shin.
- It is located on the lateral side of the tibia; it is thick & fleshy above, & tendinous below. The tibialis anterior overlaps the anterior tibial vessels &deep peroneal nerve in the upper part of the leg.
Origin of Tibialis anterior muscle
It arises from:
- Lateral condyle & upper half or 2/3 of the lateral surface of the body of the tibia
- Adjoining part of the interosseous membrane
- The deep surface of the fascia
- The intermuscular septum between it & the Extensor digitorum longus muscle.
Insertion
- Medial & under the surface of the 1st cuneiform bone, & the base of the first metatarsal bone
Structure
- It arises from the lateral condyle & upper half or two-thirds of the lateral surface of the body of the tibia; from the adjoining part of the interosseous membrane; from the deep surface of the fascia; & from the intermuscular septum between it & the extensor digitorum longus.
- The fibers of this circumpennate muscle are relatively parallel to the plane of insertion, ending in a tendon, apparent on the anteromedial dorsal aspect of the foot close to the ankle joint.
- After passing through the most medial compartments of the transverse & cruciate crural ligaments, it is inserted into the medial and under the surface of the medial cuneiform bone & the base of the first metatarsal bone.
The function of the Tibialis anterior muscle
- The tibialis anterior muscle is the medial muscle of the anterior compartment of the leg. It is responsible for dorsiflexing & inverting the foot, & the largest dorsiflexor of the foot. The muscle has 2 origins, one being the lateral tibial condyle & the other being the upper lateral surface of the tibia, & inserts on the medial surface of the medial cuneiform & adjoining part of the base of the first metatarsal of the foot allowing the toe to be pulled up & held in a locked position.
- It also allows for the ankle to be inverted giving the ankle horizontal movement and allowing for some cushion if the ankle were to be rolled. It is innervated by the deep peroneal nerve & acts as both an antagonist & a synergist of the tibialis posterior. However, the most certain antagonist of the tibialis anterior is the peroneus longus.
- The tibialis anterior aids in the activities of walking, running, hiking, kicking a ball, or any activity that requires moving the leg or keeping the leg vertical. It functions to stabilize the ankle as the foot hits the ground during the contact phase of walking (eccentric contraction) & acts later to pull the foot clear of the ground during the swing phase (concentric contraction). It also acts to ‘lock’ the ankle, as in toe-kicking a ball, when held in an isometric contraction.
- Antagonists are plantar flexors of the posterior compartment such as the soleus & gastrocnemius.
- The movements of the tibialis anterior are dorsiflexion & inversion of the ankle. However, the function of the tibialis anterior is dependent on whether the foot is weight-bearing or not (closed or open kinetic chain). When the foot is on the ground, the muscle helps to balance the leg & talus on the other tarsal bones so that the leg is kept vertical even when walking on uneven ground.
Relations
- The tibialis anterior muscle lies medial to the extensor digitorum longus & extensor hallucis longus, which makes it the most medial muscle in the anterior compartment of the leg. It also covers the anterior tibial vessels & deep fibular nerve in the proximal portion of the leg.
- The tendon of the tibialis anterior usually passes beneath the extensor retinaculum which holds it in place. However, in some cases, the superficial & deep layers of the extensor retinaculum form a separate tunnel for the muscle’s tendon. It’s mentioned that this is the only extensor tendon that has its own synovial sheath at the level of the superior extensor retinaculum. The sheath extends from above the superior extensor and retinaculum to the level of the talonavicular joint.
Nerve supply
- The tibialis anterior muscle is supplied by the deep fibular nerve (L4, L5), a branch of the common fibular nerve.
Variation
- A deep part of the muscle is rarely inserted into the talus, or a tendinous slip may pass to the head of the 1st metatarsal bone or the base of the first phalanx of the great toe.
- The tibiofascialis anterior is a small muscle from the lower part of the tibia to the transverse or cruciate crural ligaments or deep fascia.
Blood supply
- The body of the muscle is entirely supplied by the branches of the anterior tibial artery; anterior muscular, medial muscular branches & anterior tibial recurrent artery
- The tendon is mainly supplied by the branches of the anterior tibial artery but also by the branches of the posterior tibial artery. The former is the anterior medial malleolar artery & network, dorsalis pedis artery & medial tarsal arteries. The latter is the medial malleolar & calcaneal arteries.
Assessment of Tibialis anterior muscle
Palpation
- The client is supine. Place the resistance hand on the medial side of the distal foot.
- Resist the client from dorsiflexing & inverting the foot. Look at the distal tendon of the tibialis anterior on the medial side of the ankle joint & foot; it is usually visible.
- Feel the distal tendon by strumming perpendicularly across it. Constant palpating of the tibialis anterior proximally to lateral tibial condyle by strumming perpendicular to the fibers.
- Once the tibialis anterior has been located, have the client relax it & palpate to asses its baseline tone.
Power
- The action of the tibialis anterior muscle is considerably stronger than that of the other 3 dorsiflexor muscles of the foot.
Extensor hallucis longus
Introduction
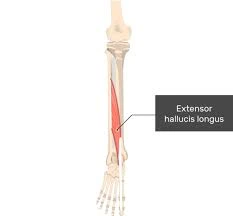
- The Extensor hallucis longus is a thin muscle, situated between the Tibialis anterior & the Extensor Digitorum Longus in the anterior compartment of the lower leg. It provides the only active extension force to the interphalangeal joint & the primary active extension force to the metatarsophalangeal joint. It has a smaller moment arm for dorsiflexion at the ankle than the anterior tibialis muscle. It has a smaller physiological cross-sectional part than either the anterior tibialis & the extensor digitorum longus.
Origin
- From the middle 2 quarters of the anterior part of the fibula & the adjacent interosseous membrane.
Insertion
- Extensor hallucis longus passes deep into the extensor retinaculum before inserting at the base of the distal phalanx of the big toe.
Structure
- The extensor hallucis longus muscle arises from the anterior surface of the fibula for about the middle 2/4th of its extent, medial to the origin of the extensor digitorum longus muscle. It also attaches from the interosseous membrane of the leg to a similar extent.
- The anterior tibial vessels & deep fibular nerve lie between it & the tibialis anterior.
- The fibers pass downward, & end in a tendon, which occupies the anterior border of the muscle, passes through a distinct compartment in the cruciate crural ligament, crosses from the lateral to the medial side of the anterior tibial vessels near the bend of the ankle, & is inserted into the base of the distal phalanx of the great toe.
- opposite the metatarsophalangeal articulation, the tendon gives off a thin prolongation on either side, to cover the part of the joint.
- An expansion from the medial portion of the tendon is generally inserted into the base of the proximal phalanx.
Function
- The main function of the extensor hallucis longus muscle is the extension of the big toe (hallux). This action happens in both metatarsophalangeal & interphalangeal joints of the hallux. This extension is a crucial movement in walking & running.
- Working together with other muscles from the anterior compartment of the leg, the extensor hallucis longus muscle dorsiflexes the foot in the ankle joint. When the foot is fixed on the ground(e.g. walking & doing squats) the muscle pulls the body slightly forward & prevents losing gravity & falling backward.
Relations
- The Extensor hallucis longus is situated between 2 muscles, posterolaterally to the tibialis anterior & posteromedially to the extensor digitorum longus muscle. The anterior tibial artery & vein & deep peroneal nerve run between the extensor hallucis longus & the tibialis anterior muscles
- The tendon of the extensor hallucis longus muscle in the dorsum of the foot runs medially to the tendon of the extensor digitorum longus. Between those 2 tendons, the dorsalis pedis artery pulse can be easily palpated.
- When extensor hallucis extends the big toe, the tendon of the muscle can be seen on the dorsal aspect of the big toe, laterally to the tendon of the tibialis anterior muscle. The space between these 2 tendons is an important clinical location; it serves as an entry point for injections or aspiration procedures in the ankle joint.
Blood supply
- The blood supply for the extensor hallucis longus muscle mainly comes from the anterior tibial artery & its branches. In further, the muscle can be supplied by the branches of the fibular artery.
- The venous blood from this part is mainly drained by the anterior tibial vein which empties into the popliteal vein.
Nerve Supply
- Deep peroneal nerve L4, L5.
variations
- Sometimes united at its origin with the extensor digitorum longus.
- The extensor ossis metatarsi hallucis, a small muscle, is many times found as a slip from the extensor hallucis longus, from the tibialis anterior, or from the extensor digitorum longus, or as a distinct muscle; it traverses the same parts of the transverse ligament with the extensor hallucis longus.
Extensor digitorum longus
Introduction
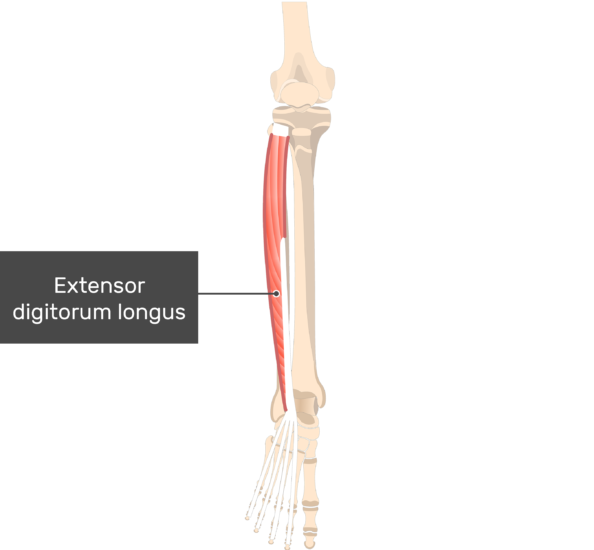
- The Extensor digitorum longus is a feather-like muscle of the anterior (extensor) compartment of the leg. Besides the extensor digitorum longus muscle, this compartment also contains the tibialis anterior, extensor hallucis longus 7 fibularis (peroneus) tertius muscles.
- Since all these muscles cross the dorsal aspect of the ankle joint, their general function is the dorsiflexion of the foot. As the extensor digitorum longus also crosses the subtalar, metatarsophalangeal & interphalangeal joints of the foot, it also Everses the foot & extends the toes
Origin and insertion
- It arises from the lateral condyle of the tibia; from the upper 3-quarters of the anterior surface of the body of the fibula; from the upper portion of the interosseous membrane; from the deep surface of the fascia; & from the intermuscular septa between it & the tibialis anterior on the medial, & the peroneal muscles on the lateral side. Between it and the tibialis anterior are the upper portions of the anterior tibial vessels & deep peroneal nerve.
- The muscle passes under the superior & inferior extensor retinaculum of the foot in company with the fibularis tertius. It divides into four slips, which run forward on the dorsum of the foot, & are inserted into the second and 3rd phalanges of the 4lesser toes.
- The tendons to the 2nd, 3rd, and 4th toes are each joined, opposite the metatarsophalangeal articulations, on the lateral side by a tendon of the extensor digitorum brevis. The tendons are inserted in the following manner: each receives a fibrous expansion from the interossei & lubricants, & then spreads out into a broad aponeurosis, which covers the dorsal surface of the 1st phalanx: this aponeurosis, at the articulation of the first with the second phalanx, divides into three slips—an intermediate, which is inserted into the base of the second phalanx; & two collateral slips, which, after uniting on the dorsal surface of the 2nd phalanx, are continued onward, to be inserted into the base of the third phalanx.
Function
- The primary function of the extensor digitorum longus is to extend the lateral 4 toes at the metatarsophalangeal joint. This means that when acting independently, it is unable to extend the whole length of the toes, extending only at the metatarsophalangeal, while at the interphalangeal joints the toes remain flexed. However, contracting together with lubricants which are the main extensors of the interphalangeal joints, this muscle contributes to extension at every joint between the bones of the lateral 4 toes.
- Acting in synergy with tibialis anterior, extensor hallucis longus & fibularis Tertius, this muscle participates in dorsiflexion of the foot when their proximal attachments are fixed. When the distal attachments are fixed & the body is in the anatomical position, all 4 muscles bring the trunk & lower limb to the front. This function moves the body weight-bearing point from the proximal to the distal portion of the foot.
- All of these actions are important for the gait cycle; the dorsiflexion angulates & lifts the foot above the walking surface, while the toe extension keeps the toes extended until the heel hits the ground.
Relations
- The extensor hallucis longus muscle is the most lateral of all the muscles in the extensor compartment & located laterally to the tibialis anterior & extensor hallucis longus. Anterior tibial artery & vein pass between the extensor digitorum longus & the tibialis anterior.
- Being within the inferior extensor retinaculum, the distal portion of the muscle crosses the anterior part of the ankle joint. While traversing the retinaculum, the tendon of extensor digitorum longus sits medially to the tendon of fibularis tertius & laterally to the extensor hallucis longus tendon. In the dorsum of the foot, tendons of the extensor hallucis longus muscle course superficially to the extensor digitorum brevis muscle.
Nerve supply
- The extensor digitorum longus is supplied by the deep fibular nerve (L5, S1), a branch of the common fibular nerve.
Variations
- This muscle varies considerably in the modes of origin & the arrangement of its various tendons.
- The tendons to the second & fifth toes may be found doubled, or extra slips are given off from one or more tendons to their corresponding metatarsal bones, to the short extensor, and to 1 of the interosseous muscles.
- The slip to the great toe from the inner tendon has been found.
Blood supply
- The leg part of the muscle is supplied by 2 arteries of the leg; the proximal part is supplied by the anterior tibial artery, while the distal part receives blood from the fibular artery.
- The tendons of the muscle are vascularized by the anterior lateral malleolar, lateral tarsal, metatarsal, plantar & digital arteries.
Assessment
- To assess the extensor digitorum longus toes 2-5 are dorsiflexed against resistance
Fibularis tertius muscle
Introduction

- The Fibularis tertius muscle, also known as peroneus tertius, is situated on the lower lateral aspect of the leg. It is a portion of the leg’s anterior, or extensor, compartment, together with 3 additional muscles; extensor digitorum longus, extensor hallucis longus & tibialis anterior. They are responsible for ankle dorsiflexion.
- Fibularis tertius extends from the distal end of the fibula to the base of the 5th metatarsal bone. Therefore, it spans & acts on 2 main joints of the foot; the talocrural (ankle) &bsubtalar joints. Due to its relatively small size & poor mechanical leverage, fibularis tertius is considered a weak dorsiflexor & evertor of the foot. In addition, the muscle is quite varied; it can be absent in some individuals, while in others it forms a portion of the extensor digitorum longus, being described as the muscle’s 5th tendon’.
Origin and insertion
Fibularis tertius originates from 3 locations:
- Is a direct attachment of the extensor digitorum longus muscle from the distal 3rd of the medial surface of the fibula.
- The anterior part of the interosseous membrane connects the tibia to the fibula. It divided the anterior from the deep posterior muscles of the leg.
- Anterior intermuscular septum, which divides the anterior & lateral compartments of the leg.
- The muscle fibers root in an inferolateral direction, forming a tendon that proceeds underneath the superior extensor retinaculum. Then, it is constant towards the inferior extensor retinaculum & courses through its loop, accompanied by the extensor digitorum longus muscle. Fibularis tertius finally inserts onto the medial part of the base of the 5th metatarsal bone
Structure
- The fibularis tertius attach from the lower 3rd of the front surface of the fibula, the lower portion of the interosseous membrane, & septum, or connective tissue, between it & the fibularis brevis. The septum is sometimes known as the intermuscular septum of Otto.
- The muscle passes downward & ends in a tendon that passes under the superior extensor retinaculum & the inferior extensor retinaculum of the foot in the same canal as the extensor digitorum longus muscle. It may be mistaken as a 5th tendon of the extensor digitorum longus.The tendon inserts into the medial portion of the posterior surface of the shaft of the 5th metatarsal bone.
- The fibularis tertius muscle is supplied by the deep fibular nerve. In rare cases, it may also be innervated by the common fibular nerve. This is unlike the other fibularis muscles, which are situated in the lateral compartment of the leg & are innervated by the superficial fibular nerve, & since the fibularis tertius muscle is found in the anterior compartment of the leg.
- The fibularis tertius may be absent in humans. It may be absent in as few as 5% of people, and as many as 72%, depending on the population surveyed. It is rarely found in other primates, which is 1 reason its action has been linked to efficient bipedalism.
Function
Due to its poor mechanical leverage, fibularis tertius can produce only 2 weak motions:
- Foot dorsiflexion around the talocrural joint, and with the help of extensor digitorum longus & tibialis anterior muscles.
- Foot eversion at the subtalar joint with the help of fibularis longus & fibularis brevis muscles.
- Through these functions fibularis tertius has a role in the gait cycle, acting with other foot dorsiflexors during the swing phase to clear the foot & toes off the floor. In addition, it has kept up functions for the ankle joint, preventing excessive inversion of the foot during physical activities. However, it is difficult to assess the true main of fibularis tertius because its function can be completed efficiently by other, more powerful muscles. In fact, fibularis tertius is absent in many individuals who do not accuse of any particular motion impairment.
Relations
- The Fibularis tertius is anterior to the fibularis brevis muscle and the anterior lateral malleolar artery. It also travels laterally to the extensor digitorum longus, with their tendons sharing a common sheath.
- Throughout its course, fibularis tertius passes laterally to the distal 3rd of the tibia, posterolaterally to the talocalcaneonavicular joint, & laterally to the tarsometatarsal joint of the foot.
Nerve supply
- Fibularis tertius is supplied by the deep fibular nerve, a branch of the sciatic nerve. It originates from the L5 & S1 spinal nerves.
Blood supply
Fibularis tertius collect arterial blood from several sources:
- Anterior tibial artery, across the anterior lateral malleolar artery
- Dorsalis pedis artery & its branches, such as the lateral tarsal artery, arcuate artery, metatarsal arteries, 4th dorsal metatarsal artery & digital arteries
- Posterior tibial artery, & the lateral plantar artery
Assessment
- Active motion & resisted movement for manual muscle testing involves combined ankle dorsiflexion & eversion.
Clinical Importance of dorsiflexor muscle
- The strength of eversion & dorsiflexion is not compromised in a person who lacks the Peroneus Tertius muscle. Peroneus Tertius seems to not provide higher protection against ankle ligamentous injury.
Peroneus Tertius Syndrome
- Peroneus Tertius Syndrome is a condition characterized by catching, clicking, locking, and popping the peroneus tertius tendon over the ankle during walking. It is a rare condition of anterolateral ankle pain and rear foot pain. This could be secondary to impingement & constriction of peroneus tertius in the extensor retinaculum.
- The Peroneus tertius muscle may be affected when a person has anterior compartment syndrome.
- The tendon may be used by surgeons as a donor for tendon transfer & tendoplasty procedures.
- While the motion of fibularis tertius cannot be tested in isolation, its tendon can sometimes be palpated. Firstly, the foot & toes should be dorsiflexed against resistance. The tendon can be felt laterally within the shallow depression situated anterior to the lateral malleolus. A tear of the tendon, which can result during a violent inversion, will result in pain & swelling over this specific location.
- The strength of eversion & dorsiflexion is not compromised in a person who lacks the Peroneus Tertius muscle. Peroneus Tertius seems to not provide higher protection against ankle ligamentous injury.
- The Extensor digitorum longus tends to be overactive & tight to compensate for an inhibited tibialis anterior. Stretching & myofascial release of the muscle together with activation tibialis anterior is indicated to regain muscle balance & improve functional ankle dorsiflexion.
- If Extensor digitorum longus muscles are tense or carry trigger points, it can cause various ailments & pains.
- Tensions in the EDL often lead to lower leg pain &local sensitivity to pressure.
- trigger points can trigger pain in the area of the ankle & foot.
Additional symptoms:
- Anterior ankle pain
- Bunion
- Dorsa forefoot pain
- Dorsal lesser toe pain
- Pain patterns of trigger points for the Extensor digitorum longus are:
- Dorsal forefoot pain
- Metatarsal head pain
- Bunion
- Anterior ankle and dorsal great toe pain⠀
- Trigger points are mainly activated through overload in sports.
- Jogging in general or jogging on uneven or slippery floors can quickly activate trigger points.
- In normal jogging, it is the monotonous motion sequence that triggers the overload of individual muscle fibers.
- Especially if you are not used to this kind of stress, give the muscle too little time to adjust or do not perform balancing activities such as massages & stretches. On uneven floors, the muscle requires to stabilize the ankle more heavily, which can overload it, too. On a slippery floor, the toes slip slightly backward with every step. This is a high stimulus for the muscle & may overload it. Other factors that development of trigger points are instabilities at the ankle joints.
- Take the quadruped stand.
- Place the foam roller under the shinbone.
- Shift some weight to the side to be massaged in order to push the roll into the muscle.
- If you don‘t shift the weight, you will as a result only press on the shinbone.
- Execute short & slow rolling movements over the entire length of the muscles & look for painful tensions
- Once you find one, roll sometimes from just prior to just behind the painful spot.
The primary function of the tibialis anterior is dorsiflexion, paralysis of this muscle results in foot drop, & an inability to dorsiflex. This paralysis can be caused by nerve injury, like direct damage to the deep peroneal nerve, & a muscle disorder, like ALS. “Foot drop” is often most common during gait when the patient cannot clear their foot during the swing phase.
Tendinitis
The tibialis anterior tendon (TAT), like any tendon, can become irritated & inflamed—a condition known as tibialis anterior tendinitis. Excessive tension on the tendon causes tendinitis, often due to repetitive, high-force activities, for example, hill running& direct contact with equipment, like a shoe that is too tight around the ankle & the tendon. The tendon traverses the anterior ankle & inserts on the medial foot, most patients will complain of pain at the front of the ankle or the medial midfoot. Pain will be aggravated by the stressful activity & alleviated by rest. Symptoms usually present gradually & get progressively worse.
Tibial Stress Syndrome (Shin Splints)
- The tibialis anterior muscle is also overused, resulting in a tibial stress syndrome more frequently known as shin splints. Anterior tibial stress syndrome (ATSS) is acute & experienced by new runners or walkers; medial tibial stress syndrome (MTSS) is more chronic & occurs in athletes. The anterior tibialis muscle is more commonly added in the former, while the tibialis posterior muscle is more commonly added in the latter. The tibialis anterior can also cause MTSS.
- Both syndromes are caused by repetitive stress & strain on the tibia, often due to training errors or various biomechanical abnormalities. Training errors include the recent onset of increased activity, intensity, & duration of running & walking on hard or uneven surfaces. Biomechanical abnormalities include hyperpronation of the subtalar joint & tibial torsion. Tibial stress syndrome, particularly MTSS, can improve to a stress fracture of the tibia. This is more general in females than males due to a higher incidence of diminished bone density & osteoporosis.
Anterior Compartment Syndrome
- Compartment syndrome happens when tissue pressure within a closed, non-extensible muscle compartment exceeds the perfusion pressure. Pressure greater than 30 mm Hg (in relaxed muscles, normal tissue pressure is 10-12 mm Hg) compromises circulation & can lead to necrosis and ischemia. In acute compartment syndrome, the increased pressure is caused by bleeding or edema, usually due to fracture or trauma. In chronic compartment syndrome, more pressure in skeletal muscle is due to overexertion. Unlike other exertional injuries, like ATSS & MTSS, chronic compartment syndrome does not respond to NSAIDs & physical therapy. In the leg, the anterior compartment is most commonly affected by compartment syndrome.
Paralysis of Extensor hallucis longus
- In the paralysis of Extensor hallucis longus, the action of Extensor hallucis brevis is dominant, the distal phalanx does not extend & the proximal phalanx extends in the direction of adduction.
Effect of Weakness
- Weakness of Extensor hallucis longus decreases extension at the metatarsophalangeal & interphalangeal joints. As it is the only muscle for the extension of the interphalangeal joint, decreased dorsiflexion of the great toe is diagnostic for Extensor hallucis longus weakness.
- During normal locomotion, an individual contacts the floor with the heel of the foot 1st. The ground reaction force put in a plantarflexion moment to the foot, which is resisted by all of the dorsiflexors functions. Weakness of the Extensor hallucis longus diminishes an individual’s ability to control the descent of the medial part of the foot, particularly the great toe.
- Patients with weakness of the extensor hallucis longus also report that the toe tends to fold under the front when they are pulling on socks or shoes &can cause tripping.
Effect of Tightness
- Tightness of the Extensor hallucis longus pulls the metatarsophalangeal joint of the great toe into extension, which, as in the fingers & thumb, tends to produce flexion at the interphalangeal joint, leading to a claw toe deformity.
- Hyperextension of the great toe pulls the plantar plate distally, exposing the metatarsal head to excessive loads & producing pain. Similarly, hyperextension of the metatarsophalangeal joint pulls the interphalangeal joint into the toe box of a shoe, causing pain & calluses, or corns, on the dorsal surface of the interphalangeal joint.
Claw Deformities of the toes :
Claw toe deformities in a foot with sensation are fully painful. Claw deformities in a foot without sensation put the individual at risk of skin breakdown as the result of increased pressure under the metatarsal heads & between the dorsal surfaces of the toes & the shoe.
Trigger point referral
Extensor hallucis long refers pain to in the distal part of the 1st metatarsal & great toe, as well as the dorsum of the foot. It may reach up the leg as far as the place. These points are situated just distal to the junction between the middle & distal thirds of the leg, just anterior to the fibula. The patient may also complain of Paralysis of Extensor hallucis longus.
compartment syndrome
Compartment syndrome is a relatively frequent cause of the dysfunction of the extensor hallucis longus muscle. Compartment syndrome is a medical emergency caused usually by blunt force trauma to the anterior side of the leg. Due to strong & inflexible fascial membranes, the swelling increases the pressure which compromises the circulation & function of the muscles (e.g. the extensor hallucis longus) within that space.
Dorsiflexors muscle stretching exercise
- Standing Shin Stretch
- Kneeling Shin Stretch
- Seated Shin Stretch
- Lying Shin Stretch
- Toe walking
- Ankle ABC’s
- Standing Stretch

Standing Shin Stretch
How to do:
- Stand tall. You need to use a hand on a wall & other support for balance.
- Slightly bend both knees.
- The right foot remains squarely on the floor. The foot is to be stretched or the left foot is placed just behind this stable & right foot, with the toe of the left foot touching the ground.
- Keeping your toe firmly on the ground, pull the left leg forward so you feel a stretch from the top of your left foot through the shins.
- Once you feel a stretch, hold it for 10-30 seconds.
- Repeat the stretch with the right foot.

Kneeling Shin Stretch
How to do:
- Kneeling can be used for gradually stretching the shins.
- You must have good knee flexion to perform this stretch as you will be sitting on the heels. If it causes pain in the knees, don’t perform it.
- Kneel on a mat with the tops of the feet flat on the ground & the buttocks over the heels.
- You feel stretching on the shin.
- Hold for 10-20 seconds.

Seated Shin Stretch
How to do:
- Sit on a chair.
- Drop the knee towards the floor so the toe of your foot is extended into the ground as in the standing stretch.
- gradually pull forward while the toe is planted on the floor, similar to the standing stretch but seated.
- Hold for 10-20 seconds.
- Repeat for both feet.

Lying Shin Stretch
How to do:
- The lying Shin Stretch stretch is similar to the lying quadriceps stretch.
- Lie on the one side. Now, bend the upper knee so your foot is behind the back.
- Reach back & grasp the forefoot, pulling it towards the back.
- Hold for 10-20 seconds.
- Repeat for both feet.

Toe walking
How to do:
- Stand tall. Now transfer the body weight onto the toes & heels off the floor.
- Then walk on the toes which gives to you dynamic shin stretch.
- You can use the wall for support throughout the walk.
- Walk for 1-2 minutes.
Ankle ABC’s
- How to do: Moving the ankle in multiple directions is one way to slowly stretch the Dorsiflexors muscle.
- Take a comfortable sitting position with the feet unsupported. Remove your shoes & socks.
- Slowly draw the alphabet in the air, leading with the big toe. Take as far as possible in each direction. Never allow your knee to move — all movement might come from your ankle.
- Every time the foot is pointed downward, you should feel a pulling sensation along the front of your shin.
- Repeat the alphabet 2-3 times on both legs.
Manual Toe Stretching:
- You can also use a towel to stretch the toes. Sit on the floor with the legs perfectly outstretched and a towel wrapped properly around your toes. Make sure that you hold the towel ends with your hands & pull the toes towards you. maintain yourself in this position for 20 to 30 seconds. You can also forgo the towel if you like & try pulling the toes by using your hands.
Toe Taps:
- This toe exercise helps to stretch the joint. As you sit in a comfortable chair, gently extend the big toe towards the ground as you try to point the other toes up. hold onto that position for about a second & then tap them lightly back down to the floor. Repeat this about 10-12 times & then reverse this process by gently pulling the big toe up as you keep the other toes on the floor.
Hammer Toe Finger Splint:
- The claw Toe Finger Splint is also referred to as “squeeze” & involves using the fingers for creating little splits between the toes for stretching them. Sit in a comfortable position & then bring one foot up & then place it right on your opposite thigh. Then slide the fingers gently in between the toes, gently pinching the fingers for squeezing the toes together. Repeat the exercise 12 times. If you like you can perform each toe simultaneously by putting one finger between them & pinching.
Rolls:
- This particular claw toe exercise involves tapping the toes gently on the floor from one side to the other. First, stand barefoot on some flat surface && try lifting all the toes off the ground, while making sure that you keep the heel planted. Now bring the toes gently down on the surface one by one, starting with the small & then ending with the big. Repeat the exercise 10 times & then move in the opposite direction.
Health Benefits of Dorsiflexors muscle stretching
There are many type benefits you might know:
- Reduce the risk of injury to calves, ankles & feet
- Reduced chance of getting tibialis anterior tendonitis
- Better ground clearance when walking to avoid tripping
- Reduce the risk of growing shin splints & stress fractures
- Fast-up recovery of shin splints.
- Increased athletic performance in sports where the ankle is “locked” like in soccer to kick a ball
- Increases the ankle range of motion. such as dorsiflexion,inversion, & adduction.
- It also maintains the medial arch of the foot.
- It also helps in the anticipatory postural adjustment part during gait beginning tibialis anterior perform knee flexion at the stance limb by causing forward displacement of the tibia.
- It also helps in eccentric deceleration of foot plantar flexion, pronation & eversion.
Strengthening exercise of Dorsiflexors muscle
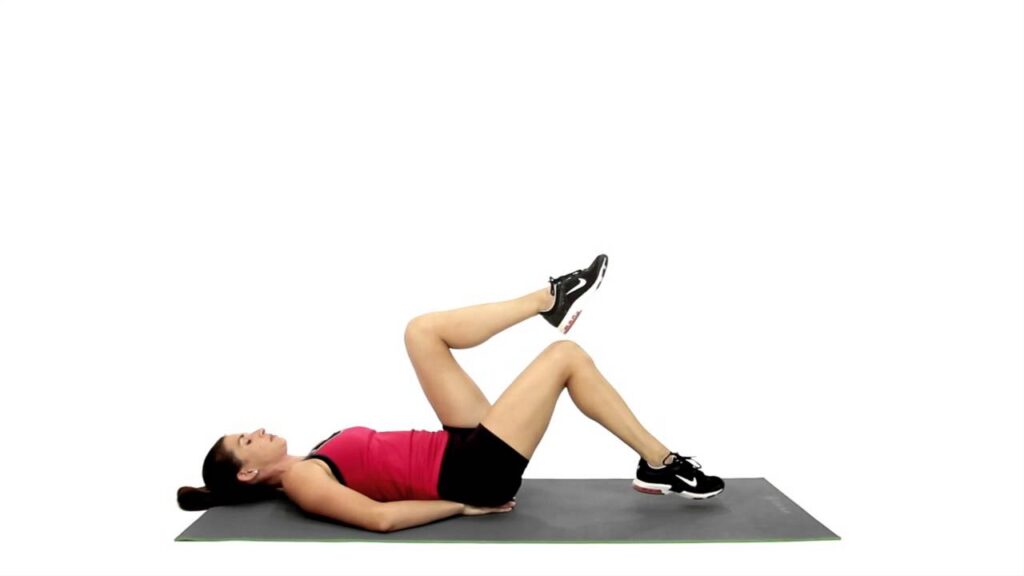
- Seated Elastic Band Exercise
- Cuff Weight Exercise
- Isometric Exercise
- Seated Calf Stretch
- Seated Toe Raises
- Wall Toe Raises
- Heel Walk
Seated Elastic Band Exercise

How to do it?
- For the Seated Elastic Band Exercise exercise, you need an elastic resistance band.
- To perform the Seated Elastic Band Exercise exercise you have to Sit on the floor with the leg extended in front of you. now Alternatively you can sit on a chair with the foot propped up on another chair.
- Wrap a resistance band over the ankle. Attach one end to a stable object like the leg of a table, & secure the other around the foot near the toes. It may be helpful to have the lower leg resting on a small pillow so the heel of the foot does not rub on the floor.
- To perform this exercise Pull the toes & foot up while keeping the knee extended. The ankle might be moved as you flex the foot up
- Pull the foot up as much as you can, & hold the end position for 2 seconds.
- Slowly relax back to the starting position.
- Do this exercise for 10-20 repetitions or until the anterior tibialis muscle tires & you can no longer flex the ankle up.

Cuff Weight Exercise
How to do it?
- For Cuff Weight Exercise you need a cuff weight.
- A cuff weight is a padded weight that you can wrap around the ankle. for Cuff Weight Exercise you have to sit in the chair & wrap a cuff weight around the toes. Make sure it is secure. Let the footrest on the floor, start this exercise by sitting with the cuff weight on the foot & then flexing the ankle so the foot & toes move up towards the knee.
- When the foot is flexed up, hold the position for 2 seconds,
- Gradually lower your toes back down to the initial position.
- Repeat the exercise for 10-20 repetitions.
Isometric Exercise
How to do it?
- Isometric exercise is a type of movement in which you push against an object you can not move. It is simple to do, & it can help strengthen the muscle in specific ranges of motion (ROM) in the ankle.
- To do isometric anterior tibialis strengthening you have to Sit in a chair & lie down.
- Cross 1 leg over the other with the affected leg on the bottom.
- Put the foot on top of the ankle you wish to exercise.
- Press the top of your weak foot into the sole of the other foot. Press down with the powerful foot to resist it. Remember, that movement occurs from the foot not from the ankle.
- Hold this position for 5 seconds, & then slowly release. Perform about 10 -15 repetitions of the exercise, 2 – 3 times a day. Isometric exercise can help to strengthen the muscles, but strength only occurs in the specific ROM in which you are exercising. That means that you might vary the position of the ankle when performing the exercise.
Seated Calf Stretch
How to do it?
- If your anterior tibialis muscle is weak, then you have difficulty flexing the foot. This means you have a shortened calf. A shortened calf will be a tight muscle, so stretching the calf may be necessary to correct the foot drop fully.
- To perform this exercise you have to Wrap a towel around the ball of the foot, & the knee should be extended.
- Pull the ends of the towel so your foot flexes up & stretches your calf.
- Hold the stretch for 15-30 seconds.
- Relax. Perform this 3 times.
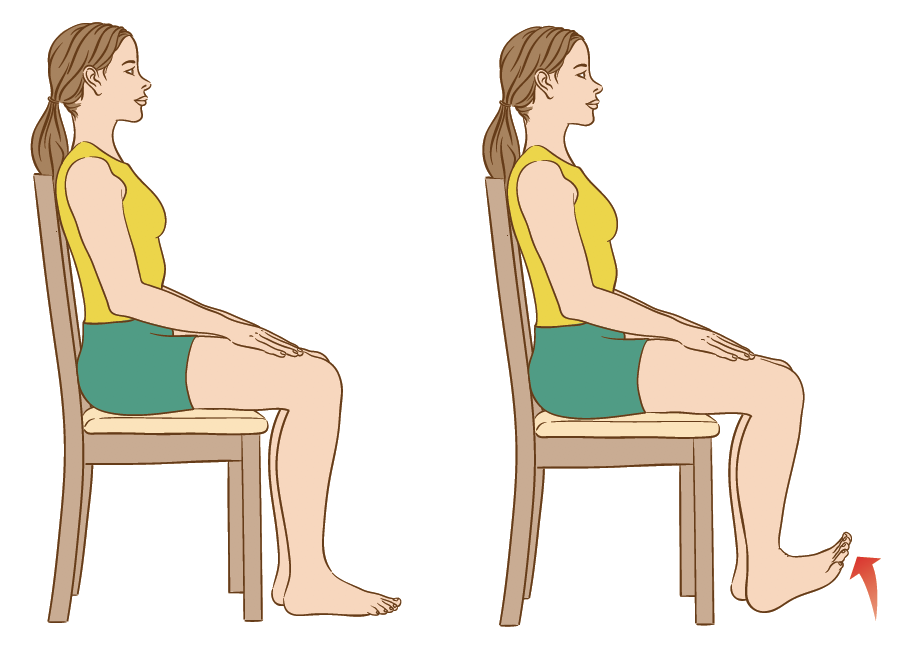
Seated Toe Raises
How to do it?
- For the Seated Toe Raises exercise, you have to Sit on a chair with the feet placed in front of you
- Now gradually raise your toes off of the ground.
- Hold for 2-5 seconds at the top
- Repeat for 2 -3 sets of 20-25 repetitions
Wall Toe Raises
How to do it?
- For the Wall Toe Raises exercise, you have to Stand 12-15 inches away with the back towards the wall with the feet hip-width apart.
- the knees might be slightly flexed then lean back into the wall.
- Elevate the toes off the floor & hold at the top for 2-4 seconds then lower the toes back to the floor.
- Repeat for 2-3 sets of 15-20 repetitions
Heel Walk

How to do it?
- For the Heel Walk exercise, you have to stand on both feet hip-width apart with no shoes on.
- Elevate the toes off the floor so that your heels are in contact with the floor.
- Walk forward while leaning back and placing weight on the heels.
- Do this for 30-40 seconds.
- Repeat this 2 to 3 times.
When did you not do the Dorsiflexors strengthening exercise?
- If you feel any pain during this exercise then do not do this exercise.
- If you are already suffering from foot & ankle pain.
- If your doctor advised you to take rest.
- If the lower limb bones are recently fractured.
Health benefits of Besides Dorsiflexors strengthening exercise:
- Assist to Reduce the risk of injury to the calf, foot, & ankle joints.
- Assist to reduce the chance of getting Besides Dorsiflexors tendonitis.
- Assist to increase ground clearance when walking to avoid tripping
- Reduce the risk of growing shin splints & stress fractures
- Speed up recovery of shin splints.
- Boost player performance in sports where the ankle is locked like in soccer to kick a ball
What are the safety & precautions of doing the Besides Dorsiflexors exercise?
There are some safety measures you require to look for:
- Don does not bounce during the stretch. it causes injuries to the muscles. Such as strain.
- Never overstretch a Besides extensor digitorum long muscle.
- Do not perform it so many times, it causes fatigue to the muscle. You might use a suggested time of repetition
- The holding time of the stretch should be recommended by your therapist which is normally 30-60 seconds.
- Never perform a stretch on the prior injured part of the body. Such as fractures, sprains, etc.
- Never stretch cold muscles, it causes pain. stretch it once you warm up the muscle.
FAQ
Muscles of the ankle
The tibialis anterior & the extensor hallucis longus produce dorsiflexion & inversion of the foot. The peroneus tertius produces dorsiflexion & eversion of the foot.
Dorsiflexion is mainly because it allows the shin bone to move forward freely. If the tibia is pushed in a vertical position, it can cause the top of our body to lean forward to keep up for the lack of mobility in the ankle when squatting
Muscles that Dorsiflex the Foot & Ankle
Anterior Tibialis.
Extensor Hallicis Longus.
Extensor Digitorum Longus.
The branches of the common peroneal nerve innervate & control the muscles in the legs that lift the ankle & toes upward (dorsi flexion). Mild peroneal nerve injuries can cause numbness, tingling, pain & weakness.