

Elbow Joint
Elbow Joint
The elbow joint serves as a pivotal connection between the upper arm bone (humerus) and the two forearm bones, the radius and ulna. This crucial joint facilitates a wide range of movements essential for everyday activities, including bending (flexion) and straightening (extension) of the arm, as well as rotational movements of the forearm (pronation and supination).
The elbow is the joint connecting the upper arm to the forearm.
Structures of the Elbow Joint
Articulating Surfaces
It consists of two separate articulations:
- Trochlear notch of the ulna and the trochlea of the humerus
- Head of the radius and the capitulum of the humerus
- Note: The proximal radioulnar joint is found within the same joint capsule of the elbow, but most resources consider it as a separate articulation.
- The radius and ulna also meet one another in the elbow to permit a small amount of rotation of the forearm.
- The elbow therefore functions to move the arm like a hinge (forward and backward) and in rotation (outward and inward).
- The biceps muscle is the major muscle that flexes the elbow hinge, and the triceps muscle is the major muscle that extends it.
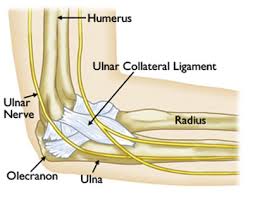
- The primary stability of the elbow is provided by the ulnar collateral ligament, located on the medial (inner) side of the elbow.
- The outer bony prominence of the elbow is the lateral epicondyle, a part of the humerus bone.
- Tendons attached to this area can be injured, causing inflammation or tendonitis (lateral epicondylitis, or tennis elbow).
- The inner portion of the elbow is a bony prominence called the medial epicondyle of the humerus.
- Additional tendons from muscles attach here and can be injured, likewise causing inflammation or tendonitis (medial epicondylitis, or golfer’s elbow)
- It is classed as a hinge-type synovial joint.
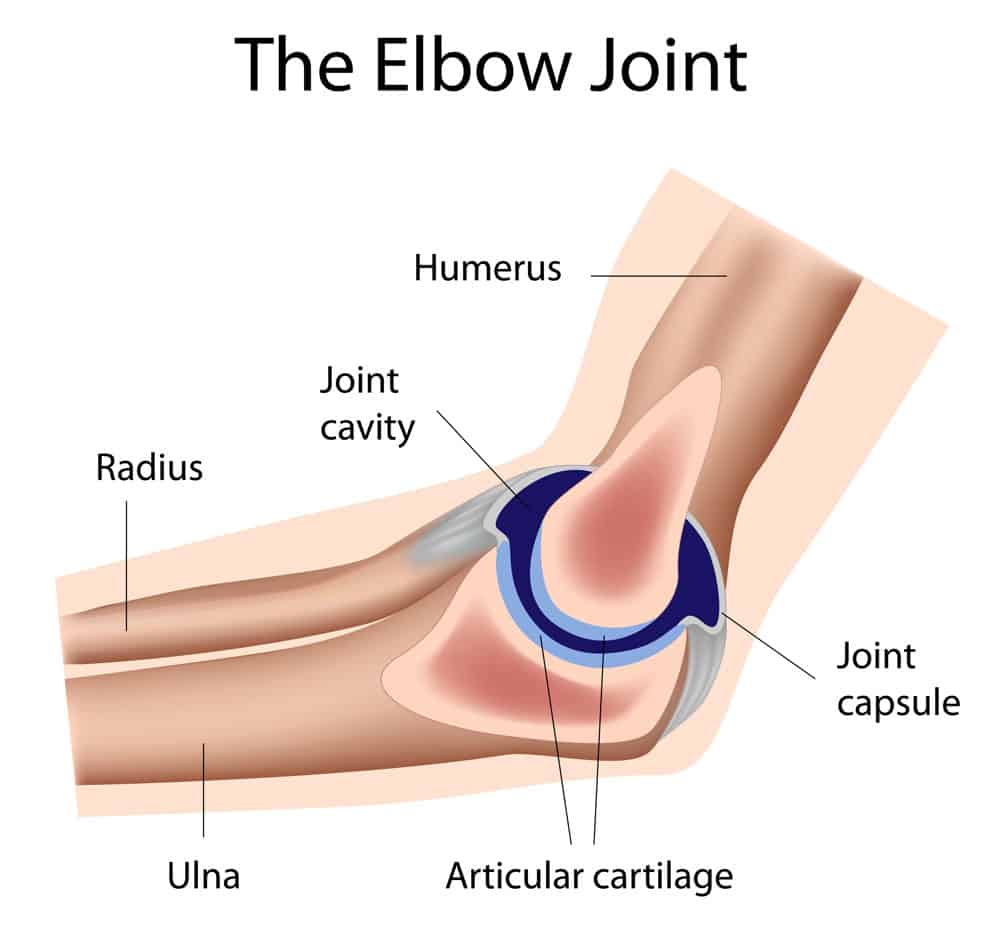
The elbow is a hinged joint made up of three bones, the humerus, ulna, and radius.
- The ends of the bones are covered with cartilage.
- Cartilage has a rubbery consistency that allows the joints to slide easily against one another and absorb shock.
- The bones are held together with ligaments that form the joint capsule.
The joint capsule is a fluid filled sac that surrounds and lubricates the joint.
- The important ligaments of the elbow are the medial collateral ligament (on the inside of the elbow) and the lateral collateral ligament (on the outside of the elbow.)
- Together these ligaments provide the main source of stability for the elbow, holding the humerus and the ulna tightly together.
- A third ligament, the annular ligament, holds the radial head tight against the ulna.
- There are tendons in your elbow that attach muscle to bone.
- The important tendons of the elbow are the biceps tendon, which is attached the biceps muscle on the front of your arm, and the triceps tendon, which attaches the triceps muscle on the back of your arm.
- The muscles in your forearm cross the elbow and attach to the humerus.
There are actually three joints at the elbow.
- Humeroulnar joint – Hinge joint formed between the humerus and the ulna.
- Allows flexion and extension of the elbow
- Humeroradial joint– Between the radius and humerus.
- Participates in flexion and extension but more importantly in supination and pronation of the forearm.
- Proximal radioulnar joint – A pivot joint formed by the radius and ulna.
- It participates in supination and pronation as well.
Anatomy of the Elbow Joint
- In anatomic position [elbow is extended, the forearm is supinated], the long axis of the forearm has a lateral inclination or valgus at the elbow.
- This is called the carrying angle and is measured to be 13±5 degrees for females and 11 ± 4 for females.
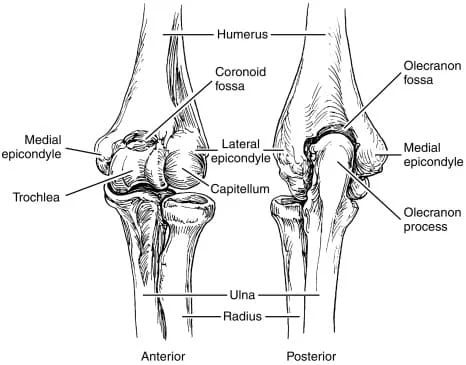
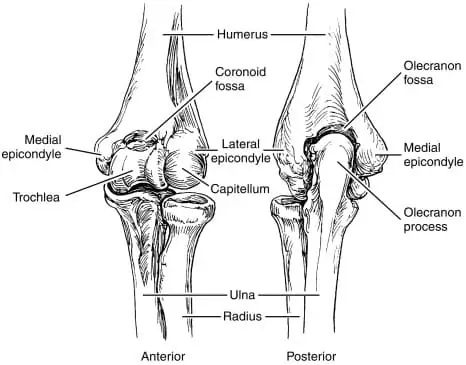
Distal End of Humerus
- The humeral condyle, the distal end of the humerus, is made up of the capitellum laterally and the trochlea medially.
- This condyle is covered by articular cartilage and articulates with the trochlear notch of the ulna and the concave superior aspect of the head of the radius.
- The axis of the trochlea is externally rotated by 3 -8 degrees and compared with the longitudinal axis is in 4- 8° of valgus.
- The articular surface of the trochlea and capitellum is projected anteriorly at an angle of 40° to the axis of the humerus.
- The trochlea, the distal medial articulating end of the humerus, acts as a pulley for the ulnar trochlear notch to rotate around as the elbow is flexed.
- The capitellum is a rounded ball of bone that adjoins the trochlea laterally.
- It is the distal lateral articulating end of the humerus. It articulates with the radial head.
- Superior to the articulating surface, the middle of the width of the humerus is marked by two depressions.
- On the anterior surface, it is the coronoid fossa that accommodates the coronoid process of the ulna on flexion.
- Lateral to it is a smaller fossa called the radial fossa that accepts the radial head on flexion.
- A depression on the posterior aspect is called the olecranon fossa, which accommodates the olecranon of the ulna on extension.
- The olecranon is the proximal end of the ulna, from which the C-shaped trochlea notch is carved
- Lateral to the humeral condyle are the medial and lateral epicondyles, and superior to those on their respective sides are the medial and lateral supracondylar ridges.
- The epicondyles and ridges serve as attachment sites for ligaments and muscles.
- Medial epicondyle serves as the origin of flexor muscles of forearm and hand whereas lateral epicondyle serves as extensor origin.
Ulna
- The upper end of ulna provides articular cartilage–covered trochlear notch carved out of the olecranon process.
- The olecranon posteriorly serves as attachment of triceps muscle, a powerful elbow extensor.
- Anteriorly, the trochlear notch ends in a blunt central point called the coronoid process.
- The tuberosity of the ulna lies inferior to the coronoid process on the anterior aspect of the ulna.
- After that, further distally, is the shaft.
- Laterally, the coronoid process is the radial notch, in which lies the head of the radius.
Radius

- Head of the radius bone is the main participant in the elbow joint.
- Its superior aspect contributes to the hinge portion of the elbow joint.
- The medial circumferential aspect of the head of the radius forms the radioulnar articulation.
- After the head, the bone narrows distally into the neck.
- Anteromedially, a thick structure is called the Distal. The head of the radius is a narrowing of the bone, referred to as the neck, and anteromedially is the radial tuberosity, followed distally by the shaft.
The joint capsule is contiguous between the hinge and radioulnar aspects of the joint.
Joint capsule and Ligaments
- The capsule has an outer fibrous layer and an inner synovial layer.
- The superior aspect of the joint capsule begins just superior to the coronoid and olecranon fossae and continues inferiorly, covering just past the proximal radial-ulnar articulation.
- Anterior or cordlike band
- A posterior fan-like band
- Oblique band
- The oblique band also helps to deepen the trochlear notch.
- The radial collateral ligament is the lateral thickening that extends from the lateral humeral epicondyle and distally blends into the annular ligament of the radius.
CAPSULAR LIGAMENT (JOINT CAPSULE)
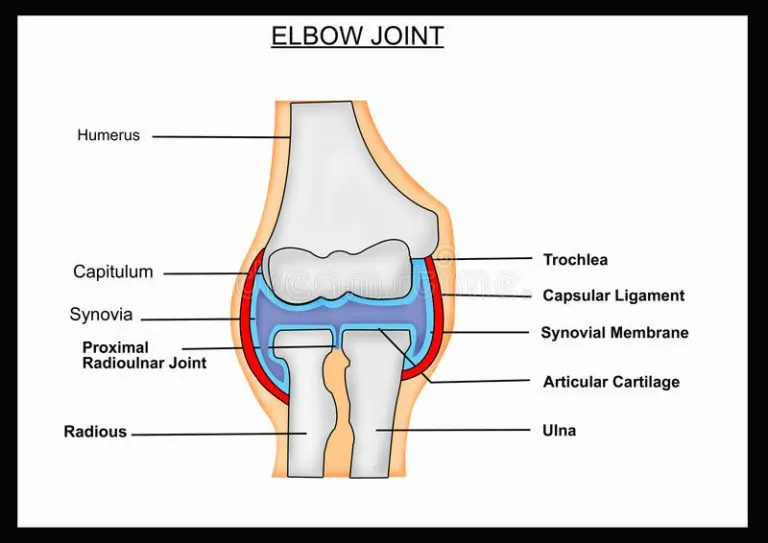
- Capsular Ligament is a sac made up of fibers that encloses the joint cavity. The inner surface of the capsule is lined by the synovial membrane
- The ulnar collateral ligament is the medial thickened part of the capsule.
- Ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid and olecranon of the ulna.
- It is a triangular thickening with 3 main bands
MEDIAL LIGAMENT (ULNAR COLLATERAL LIGAMENT)
- It is triangular in shape, with its apex attached to the medial epicondyle of the humerus and base to the coronoid and olecranon processes of the ulna.
- The Medial collateral ligament is a triangular-shaped ligament made up of three smaller ligaments named the anterior oblique ligament, posterior oblique ligament, and the transverse ligament, also sometimes called Cooper’s ligament.
- The anterior oblique ligament originates from the anterior inferior surface of the medial epicondyle of the humerus and inserts onto the coronoid process of the ulna.
- The anterior oblique ligament is the strongest and most important medial stabilizer of the elbow joint and protects against excessive valgus forces.
- The posterior oblique ligament also originates from the medial epicondyle but, as its name suggests, runs posteriorly to insert onto the olecranon of the ulna.
- The transverse ligament passes between the previous two, running from the coronoid process and the tip of the olecranon.
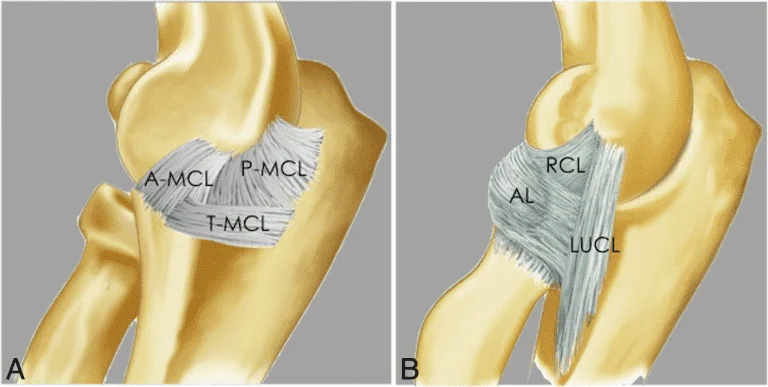
LATERAL LIGAMENT (RADIAL COLLATERAL LIGAMENT)
- It extends from lateral epicondyle of the humerus to the annular ligament with which it blends.
- The lateral collateral ligament is also composed of three parts: The annular ligament, the lateral radial collateral ligament, and the lateral ulnar collateral ligament.
- The three components of the LCL provide stability during varus stresses applied to the elbow and posterolateral rotational stability.
- The lateral ulnar collateral ligament is the predominant stabilizer in the posterolateral rotational structure as it crosses over the inferior aspect of the radial head, originating from the lateral epicondyle of the humerus and inserting at the supinator crest of the ulna.
- The annular ligament stabilizes the proximal radioulnar joint and originates and inserts at the sigmoid notch of the ulna as it wraps around the neck of the radius.
- The annular ligament of the radius wraps around the head of the radius and attaches to the ulna anteriorly and posteriorly.
- It allows the head of the radius to rotate inward during supination and pronation while maintaining the stability of the radial ulnar joint.
Muscles of the Elbow Joint
- biceps brachii, brachialis, brachioradialis, and pronator teres all flex the elbow and lie
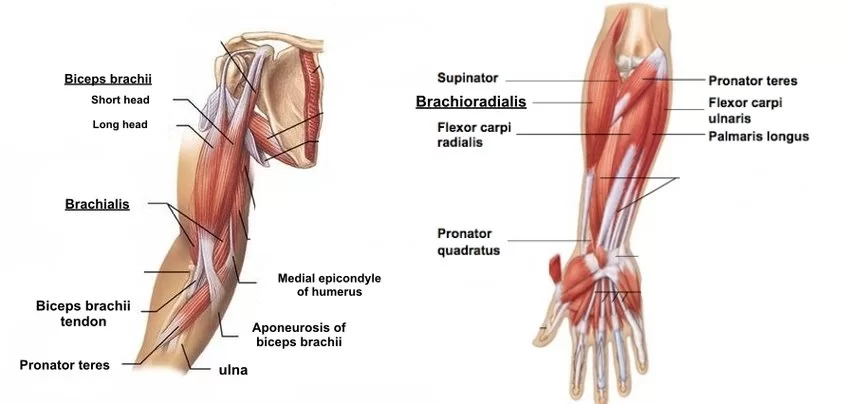
- Muscles which act primarily on the elbow joint include those responsible for flexion, including biceps brachii, brachioradialis, and brachialis.
- The biceps brachii has a modest impact on elbow flexion and acts as the primary muscle responsible for supination.
- The biceps brachii is especially unique as it has two distal attachments at the elbow joint, a more laterally oriented tendon inserting on the proximal radius, and a medially oriented aponeurosis which continues into the fascia of the proximal forearm.
- Extension of the elbow joint is accomplished almost entirely from contraction of the triceps brachii with very modest action from the anconeus muscle.
- The triceps brachii and anconeus serve to extend the elbow and lie posteriorly.
- The supinator and biceps brachii function to supinate the forearm at the elbow and the pronator teres and pronator quadratus pronate the forearm.
Movements are caused as follows
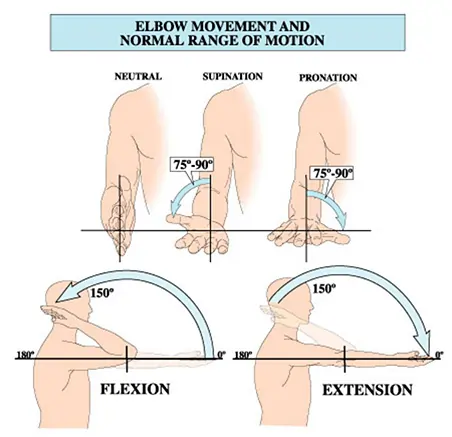
- ROM – Range of Motion
- Functional ROM
- 30° to 130 flexion/extension
- Total ROM is 0-150 degrees
- 50° supination/supination
- Normal carrying angle
- normal valgus carrying angle
- 5-10° for males
- 10-15° for females
- This diminishes with flexion
- Axial loading
- In the extended elbow
- 40% of the weight is through the ulnohumeral joint
- 60% of the weight is through the radiohumeral joint
Extension: Triceps brachii and anconeus
Flexion: Brachialis, biceps brachii, brachioradialis
- Contribution to elbow stability comes in the form of protection against varus and valgus forces.
- Muscles that protect against valgus forces by initiating a varus force include the flexor digitorum superficialis, flexor carpi ulnaris, flexor carpi radialis, and the pronator teres.
- Muscles that contribute to varus stability by initiating a valgus force include extensor digitorum communis, extensor carpi radialis brevis and longus, anconeus, and extensor carpi ulnaris.
Bursae of the Elbow Joint
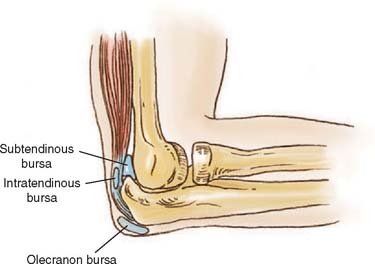
- Intratendinous – located within the tendon of the triceps brachii.
- Subtendinous – between the olecranon and the tendon of the triceps brachii.
- Subcutaneous – between the olecranon and the overlying connective tissue.
Nerve supply of Elbow Joint
Nerve of the Elbow
Musculocutaneous nerve
- Origin: lateral cord of the brachial plexus
- It exits laterally, distal to the biceps tendon
- It will terminate as the LABC (forearm), which is found deep to the cephalic vein
- Innervation at the elbow
- It supplies the biceps and brachialis
- The nerve runs between these muscles
Radial nerve
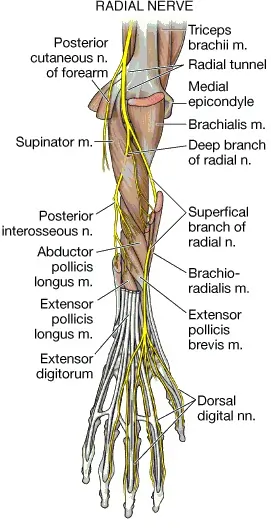
- Origin: posterior cord of the brachial plexus
- It leaves the triangular interval (teres major, long head of triceps and humeral shaft)
- Found in spiral groove 13 cm above the trochlea
- Pierces lateral intermuscular septum 7.5 cm above the trochlea
- This is usually at the junction of the middle and distal third of the humerus
- Lies between the brachialis and the brachioradialis
- Distally it is located superficial to the joint capsule, at the level of the radiocapitellar joint
Median nerve
- Origin: medial/lateral cords of the brachial plexus
- It courses with brachial artery, running from lateral to medial
- Lies superficial to brachialis muscle at level of elbow joint
- Innervation at elbow
- It gives branches to elbow joint
- It has no branches in upper arm
- Origin: medial cord of brachial plexus
- Runs medial to brachial artery, pierces medial intermuscular septum (at the level of the arcade of Struthers) and enters posterior compartment
- It traverses posterior to the medial epicondyle through the cubital tunnel
- Innervation at elbow
- It gives branches to elbow joint
- It has no branches in upper arm
- First motor branch to FCU is found distal to the elbow joint
- The elbow joint is supplied by the musculocutaneous, radial, and ulnar nerves.
- Nervewise, the inferior lateral cutaneous nerve of the arm and the posterior cutaneous nerve of the forearm supply lateral elbow.
- The medial cutaneous nerve of the forearm supplies sensation to the medial aspect of the elbow.
- The cubital fossa is supplied by musculocutaneous nerve (the lateral cutaneous nerve of the forearm).
Dermatome
- The skin over the joint belongs anteriorlaterally to C6 dermatome and anteromedially to C5, C8, and T1 dermatomes.
- Posteriorly, the C6 dermatome laterally and the C8 dermatome medially are split down the middle by the C7 dermatome.
Blood Supply of Elbow Joint
- The blood supply to the elbow joint is by the branches from the periarticular arterial anastomoses of the elbow.
Blood Supply of Elbow
- Is located medially in the upper arm
- It enters the cubital fossa laterally
- Contents– biceps tendon (lateral), brachial artery, median nerve (medial)
- Lateral border–brachoradialis
- Medial border–pronator teres
- Proximal border –distal humerus
- At the level of elbow it splits into the radial and ulnar arteries
Principle branches
- Superior/inferior ulnar collateral
- Nutrient/muscular
- Supratrochlear
elbow anastomosis
Clinical Significance of Elbow Joint
Elbow joint is a frequently injured joint and the site of many disorders
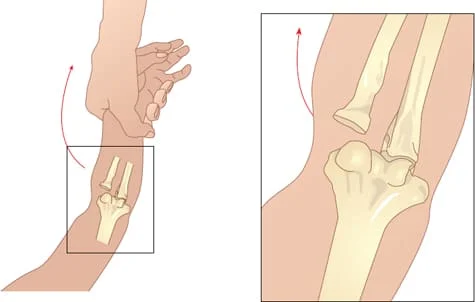
Dislocation of Elbow
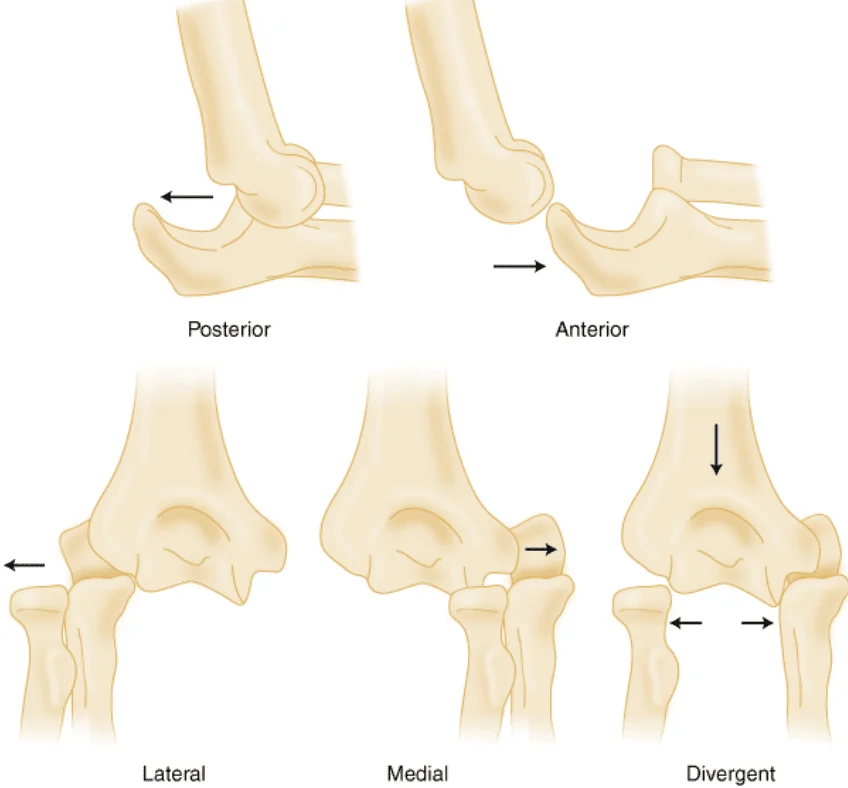
- Lateral View Of Dislocation Of Elbow
- Dislocation of the elbow could occur in isolation or as part of more severe trauma which may cause fracture of the bones too.
Pulled Elbow
- In children, when a distraction force is applied along the long axis of the forearm from a point distal to the elbow, the head of the radius can be pulled out of the annular ligament that holds it in place.
- This injury is called “pulled elbow” and occurs in young children.
- The injury usually involves a parent or other adult figure lifting a child up vertically with a single hand.
Lateral epicondylitis
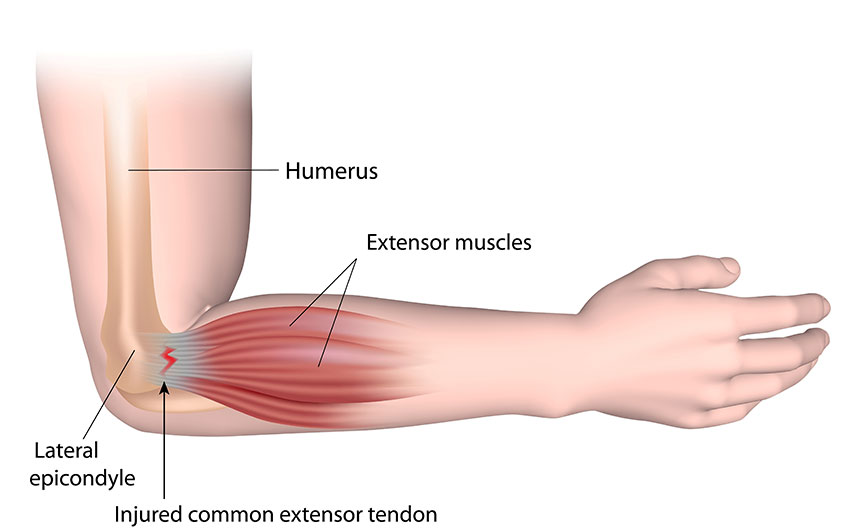
- Lateral epicondylitis is also called tennis elbow and involves inflammation of the common extensor origin at the lateral epicondyle of the humerus.
- Repetitive extension movements at the wrist cause pain.
Medial epicondylitis
- Medial epicondylitis or golfer’s elbow is an inflammation of the common flexor origin at the medial epicondyle of the humerus.
- Repetitive flexion movements at the wrist cause an overuse of pain at the site.
Cubital tunnel syndrome
- Cubital tunnel syndrome is caused by compression of the nerve as it passes in a groove behind the medial epicondyle of the humerus or cubital tunnel.
- Paresthesias in the distribution of the ulnar nerve are the chief complaint.
Pronator syndrome
- Compression neuropathy of the median nerve as it passes between the two heads of the pronator teres muscle.
- The syndrome can cause paresthesias in the distribution of the median nerve distal to the compression and may lead to weakness in the flexor pollicis longus, the flexor digitorum profundus laterally, and the pronator quadratus.
Olecranon bursitis

- Olecranon bursitis or student’s elbow is an inflammation of the olecranon bursa at the proximal aspect of the posterior ulna.
- It can be caused by trauma, infection, prolonged pressure, or other conditions. The bursa is swollen and is often painful.
Throwing injuries
- Also called “baseball pitcher’s elbow,” these types of injuries are due to excessive use of the elbow when a baseball is thrown.
- Other sports that involve similar mechanisms produce similar injuries that involve elbow structures such as tendon detachments and other tissue injuries, often seen in children who pitch in Little League.
- Radial nerve compression: Pinching or compression of the radial nerve that passes through the elbow joint
- Ulnar nerve compression (or entrapment): Pinching or compression of the nerve by swelling or displacement
little league elbow
- A form of overuse syndrome marked by tension being placed on the medial structures of the elbow and, possibly, compression forces being placed on the lateral structures.
- Long-term consequences include abnormal growth of the medial epicondyle and avulsion of the medial epicondyle.
- It is seen in adolescent baseball players, esp. in pitchers.
- In order to help prevent this condition, Little League Baseball regulations limit the number of pitches a player can throw per week.
nursemaid’s elbow
- Subluxation of the head of the radius with entrapment of the annular ligament in the radiohumeral joint, esp. in a young child after being lifted by the hand or wrist.
- The condition is acutely painful, and the child will not willingly use the affected arm.
Treatment
The subluxation can be readily reduced with closed manipulation.
Synonym: radial head subluxation
tennis elbow
First Steps of Treatment
- If you have suffered an elbow injury or have elbow pain, there are a few things you should do to start treatment right away.
- First, you should check in with your doctor to rule out any serious injury to your elbow’s ligaments or bones.
- The last thing you want is to treat a serious elbow fracture like a minor strain.
- After an elbow injury, you may benefit from using the R.I.C.E. method to help control the inflammation process.
- The RICE Principle – stands for rest, ice, compression, and elevation.
- Rest your elbow, apply an ice pack, and elevate your arm to minimize the swelling.
- Some physiotherapists are now advocating the P.O.L.I.C.E. principle of injury management.
- This stands for protection, optimal loading, ice, compression, and elevation.
- This principle takes out the rest and adds some protection to your joint while still allowing for some motion to your elbow as it heals.
- You may benefit from a gentle range of motion exercises for your elbow after an injury.
- Visit your physiotherapist for a complete assessment to see which exercises you should do to get your elbow moving.
- After a ligament injury to your elbow, you may also benefit from strengthening exercises for your forearm and wrist to help provide muscular support to your elbow.
- Again, your PT can prescribe the correct exercises for your condition.



30 Comments