

Elbow Pain: Physiotherapy Treatment
Table of Contents
What is an Elbow Pain?
- Elbow pain is often caused by overuse. Many sports, hobbies and jobs require repetitive hand, wrist or arm movements.
- Elbow pain may occasionally be due to arthritis, but in general, your elbow joint is much less prone to wear-and-tear damage than are many other joints.
- Elbow pain is most often the result of tendinitis, which can affect the inner or outer elbow. Treatment includes ice, rest, and medication for inflammation.
- Elbow pain has many other causes including arthritis and bursitis. Funny bone sensation is irritation of a nerve at the elbow that causes numbness and tingling of the inner elbow, forearm as well as little and ring fingers.
- Bacteria can infect the skin of a scraped (abraded) elbow to cause pain.
DEFINITION:
- Elbow pain usually isn’t serious, but because you use your elbow in so many ways, elbow pain can be very frustrating. Your elbow is a complex joint; it allows you to both extend and flex, as well as rotate your hand and forearm. Since most movements are a combination of these actions, you may sometimes find it difficult to describe exactly which movement brings on the pain.
ANATOMY OF ELBOW JOINT:
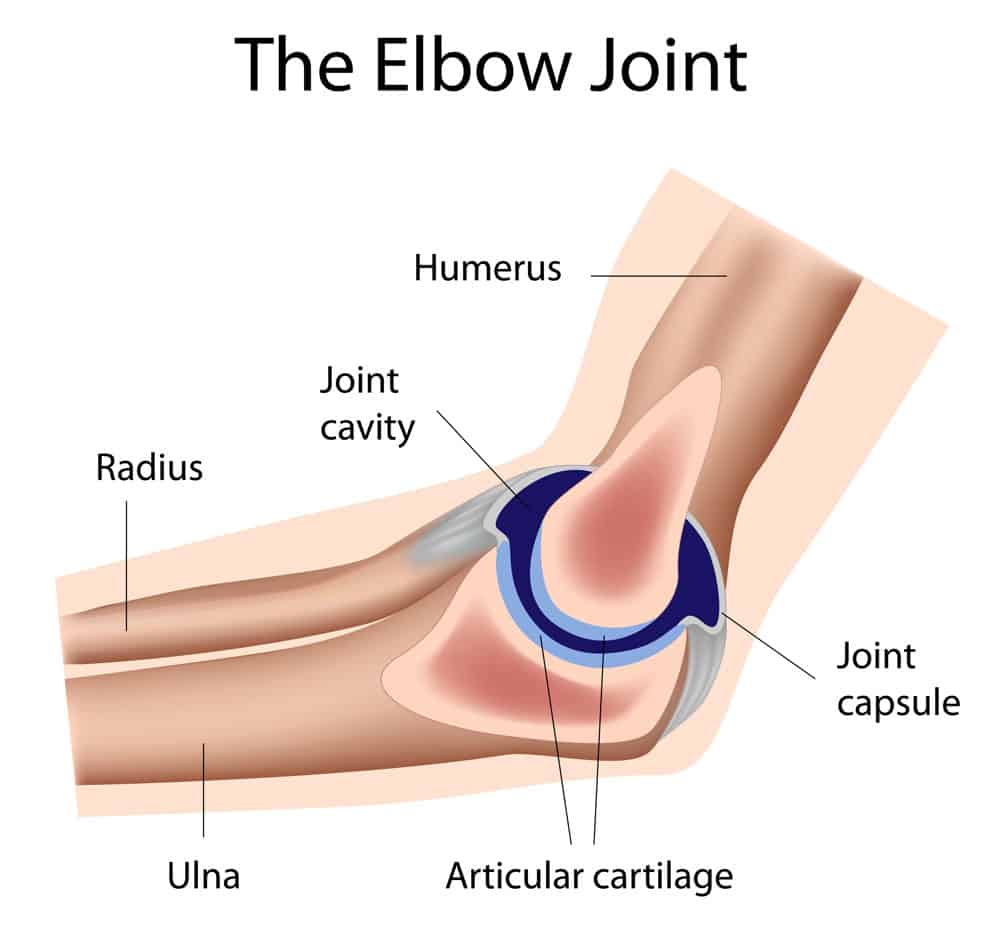
- The elbow joint is a synovial joint found in the upper limb between the arm and the forearm. It is the point of articulation of three bones: the humerus of the arm and the radius and the ulna of the forearm.
- The elbow joint is classified structurally as a synovial joint.
- It is also classified structurally as a compound joint, as there are two articulations in the joint. Synovial joints, also called diarthroses, are free movable joints. The articular surfaces of the bones at these joints are separated from each other by a layer of hyaline cartilage. Smooth movement at these joints is provided by a highly viscous synovial fluid, which acts as a lubricant.
- A fibrous capsule encloses the joint, and is lined internally by a synovial membrane. Synovial joints can be further categorized based on function. The elbow joint is functionally a hinge joint, allowing movement in only one plane (uni axial).
OSTEOLOGY:
There are three bones that comprise the elbow joint:
-the humerus
-the radius
-the ulna.
These bones give rise to two joints
- 1)Humeroulnar joint
- 2)Humeroradial Joint
- Humeroulnar joint is the joint between the trochlea on the medial aspect of the distal end of the humerus and the trochlear notch on the proximal ulna.
- Humeroradial joint is the joint between the capitulum on the lateral aspect of the distal end of the humerus with the head of the radius.
- The humeroulnar and the humeroradial joints are the joints that give the elbow its characteristic hinge like properties. The rounded surfaces of the trochlea and capitulum of the humerus rotate against the concave surfaces of the trochlear notch of the ulna and head of the radius.
- At the elbow joint, the proximal ends of the radius and ulna articulate with each other at the proximal radio ulnar joint.
- This joint, however, is considered to be a separate articulation than those forming the elbow joint itself. The proximal radio ulnar joint is the articulation between the circumferential head of the radius and a fibro-osseous ring formed by the radial groove of the ulna and the annular ligament that hold the head of the radius in this groove. The proximal radio ulnar joint is functionally a pivot joint, allowing a rotational movement of the radius on the ulna.
LIGAMENTS OF THE ELBOW JOINT:
- There are a collection of ligaments that connect the bones forming the elbow joint to each other, contributing to the stability of the joint. The humeroulnar and the humeroradial joints each have a ligament connecting the two bones involved in the articulation: the ulnar collateral and the radial collateral ligaments.
- The ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid process of the ulna. It is triangular in shape and is composed of three parts: an anterior, a posterior, and an inferior band.
- The radial collateral ligament has a low attachment to the lateral epicondyle of the humerus. The distal fibres blend with the annular ligament that encloses the head of the radius, as well as with the fibers of the supinator and the extensor carpi radialis brevis muscles.
- The annular ligament also reinforces the joint by holding the radius and ulna together at their proximal articulation. The quadrate ligament is also present at this joint, and maintains constant tension during pronation and supination movements of the forearm.
BLOOD SUPPLY AND INNERVATION:
- The blood supply to the elbow joint is derived from a number of periarticular anastamoses that are formed by the collateral and recurrent branches of the brachial, profunda brachii, radial and ulnar arteries. Proximal to the elbow joint, the brachial artery, the largest in the arm, gives off two branches, a superior and inferior ulnar collateral artery. The profunda brachii gives off a radial collateral and a middle collateral artery. These pass towards the joint contributing to the anastomotic loop supplying the joint.
- Distal to the elbow joint, the radial artery gives off the radial recurrent artery, and the ulnar artery gives off the anterior and posterior ulnar recurrent arteries. These arteries ascend towards the elbow joint, anastamosing with the branches from the brachial and profunda brachii arteries in the arm.
MOVEMENTS:
- As the elbow joint is a hinge joint, movement is in only one plane. The movements at the elbow joint involve movement of the forearm at the elbow joint. Flexion of the forearm at the elbow joint involves decreasing the angle between the forearm and the arm at the elbow joint. Extension involves increasing the angle between the arm and forearm. These movements are performed by two groups of muscles in the arm: the anterior compartment and the posterior compartment of the arm.
Flexion
Most of the muscles producing flexion are found in the anterior compartment of the arm. There are two muscles in this compartment that produce flexion at the elbow joint:
- Biceps Brachii originates as two heads. The tendon of the long head originates from the supra glenoid tubercle of the scapula. It passes through the joint capsule of the shoulder joint and through the bicipital groove on the anterior surface of the humerus. The short head of the biceps brachii muscle originates from the coracoid process of the scapula. These heads join together to form the biceps brachii muscle belly. The muscle inserts via a single tendon onto the radial tuberosity distal to the elbow joint. In the forearm, there is a continuation of this tendon as a flattened connective tissue sheath, the bicipital aponeurosis. This aponeurosis blends with the deep fascia in the anterior forearm.
- Brachialis originates from the distal half of the anterior surface of the humerus, as well as from the intermuscular septa on either side of the anterior compartment. It is located deep to the biceps brachii muscle. It forms a singular tendon that inserts onto the tuberosity of the ulna.
- Both the biceps brachii and brachialis muscles are innervated by the Musculocutaneous nerve.
- While the biceps brachii and the brachialis muscles are the main flexors of the elbow joint, the brachioradialis muscle is also involved in flexion of the forearm at this joint.
- Brachioradialis originates for the lateral aspect of the distal humerus above the lateral epicondyle. It inserts onto the lateral aspect of the distal radius. Although this muscle is primarily in the forearm, it crosses the elbow joint so therefore it acts on the elbow joint. It is innervated by the radial nerve.
Extension
- Extension of the forearm at the elbow joint is the increase of the angle at the elbow to bring the forearm back to the anatomical position from a flexed position. There is one muscle involved in extension, the triceps brachii muscle. It is the only muscle in the posterior compartment of the arm.
- Triceps Brachii originates as three heads. The long head originates from the infra glenoid tubercle of the scapula, the lateral head originates from the lateral aspect of the humerus above the radial groove, and the medial head originates from the medial aspect of the humerus below the level of the radial groove. The three heads converge on a single tendon that inserts onto the olecranon of the ulna. It is supplied by the radial nerve, which passes down through the arm in the radial groove between the lateral and medial heads of the muscle.
- While flexion and extension are the only movements that can occur at the elbow joint itself, movement is also afforded at the proximal radioulnar joint, which contributes to the elbow joint. Movements at this joint are called pronation and supination. These are rotational movements that occur when the distal end of the radius moves over the distal end of the ulna by rotating the radius in the pivot joint formed by the circular head of the radius, the radial groove of the ulna, and the annular ligament.
- Pronation and supination are easily visualized when the elbow is flexed at 90°. Supination is where the palm of the hand is facing upwards; pronation is a rotation of the forearm so that the palm is facing downwards. In the anatomical position, the forearm is in the supine position. Pronation in the anatomical position is the movement of the forearm so that the palm is facing posteriorly.
What are the Common Causes of Elbow Pain?
- Most cases of elbow pain are due to strained or inflamed soft tissues such as tendons or ligaments.
- These tend to get better after a few days with simple self-care you can do at home.
- Sometimes elbow pain may be caused by a medical condition.
- A number of things can cause stiffness in your elbow, including arthritis (arth-rye-tus). Arthritis simply means a joint that is painful and swollen, and there are a number of types of arthritis.
- Stiffness can happen due to problems with the elbow joint itself or with the muscles, covering of the joint, or ligaments.
- In some situations, such as after an injury or operation, soft tissue can form into scar tissue. This can cause elbow stiffness.
- Occasionally, the elbow may lock in a fixed position. This is often short-lived but may be due to a loose bit of bone or cartilage in the joint.
Common causes of elbow pain include:
- Broken arm
- Bursitis (joint inflammation)
- Dislocated elbow
- Golfer’s elbow
- Osteoarthritis (disease causing the breakdown of joints)
- Osteochondritis dissecans
- Rheumatoid arthritis (inflammatory joint disease)
- Sprains
- Stress fractures
- Tendinitis
- Tennis elbow
- Throwing injuries
- Trapped nerves
Lateral Epicondylitis:-Lateral epicondylitis, also called tennis elbow, is the most common cause of elbow pain and refers to inflammation of the tendon that attaches the elbow bone to the forearm muscles used to extend the wrist and fingers. People who repetitively use their forearm muscles, such as tennis players, weightlifters, painters, and plumbers, are especially prone to developing lateral epicondylitis.
- Typically, the elbow pain from lateral epicondylitis is burning, comes on gradually, and worsens with activities that involve the use of the forearm extensor muscles like turning a wrench, mixing dough when baking, or holding a tennis racquet. Difficulties gripping objects is another potential symptoms of lateral epicondylitis.
Medial Epicondylitis:-Similar to lateral epicondylitis, medial epicondylitis (“golfer’s elbow”) causes discomfort around the joint. However, the symptoms of medial epicondylitis are located on the inner side of the elbow and are due to inflammation of the tendon that connects the elbow bone to the forearm muscles used to flex the wrist and fingers. Repetitive, forceful gripping (for example, of a golf club, racquet, or heavy tool) is often what triggers medial epicondylitis. Forearm weakness may also occur.
Olecranon Bursitis: The olecranon bursa is a fluid-filled sac located between the tip of the elbow bone and the skin. When a patient has olecranon bursitis, they usually have swelling and tenderness behind the joint over the bony prominence called the olecranon. If the swelling gets big enough, a person may not be able to fully move his or her elbow.
- Acute (“sudden”) olecranon bursitis usually develops as a result of gout, infection, or trauma to the elbow.3? With an infected bursa, redness and warmth develops over the tip of the elbow. Some people develop a fever.
- Chronic bursitis, meaning the condition develops slowly over time, is usually due to repetitive overuse (for example, prolonged pressure on the elbows) or inflammatory arthritis (for example, rheumatoid arthritis).
Biceps and Triceps Tendonitis:-The biceps tendon is a tough, fibrous tissue that connects the biceps muscle to the front of the elbow bone, while the triceps tendon connects the triceps muscle to the back of the elbow bone.
- Biceps tendonitis is most commonly caused by repetitive biceps muscle activity (for example, lifting heavy boxes) and causes an aching pain in front of the elbow. On the other hand, triceps tendonitis (less common than biceps tendonitis) causes an aching pain at the back of the elbow and is most commonly caused by people who repetitively extend their elbow against resistance (for example, weightlifters).
- If a biceps or triceps tendon ruptures, a sudden, severe pain, along with a snapping or popping sensation, may be felt. Swelling and bruising may also occur near the elbow and forearm, and a visible lump may form on the upper arm.
Cubital Tunnel Syndrome:-Your ulnar nerve travels from your neck to your hand. Sometimes, the nerve becomes compressed as it wraps around the inside of the elbow. This condition is called cubital tunnel syndrome. Along with an aching pain in the inside of the elbow, cubital tunnel syndrome often causes numbness and tingling of the fifth (“pinky”) and fourth (“ring”) fingers.
Sometimes people report shooting pain along the forearm, as well as a weak grip.
Radial Tunnel Syndrome:-Radial tunnel syndrome is an uncommon condition that results from radial nerve compression. The radial nerve travels down the arm and controls the triceps muscle and the wrist extensor muscles (located at the back of the upper arm and forearm, respectively). Most often, this diagnosis is considered in people who engage in repetitive rotation of the forearm muscles (for example, carpenters or mechanics).
Besides a vague pain located within the forearm that comes on gradually, a person with radial tunnel syndrome may experience numbness over the back of the hand that may extend up the back of the forearm.
Elbow Fractures:-Broken bones can occur around the elbow after injuries such as a fall on the elbow or an outstretched hand, or a direct blow to the elbow, such as from a car accident.
The most common elbow fractures are olecranon fractures and radial head fractures. Symptoms of an elbow fracture include a sudden, severe pain in the elbow and forearm, along with swelling, possible numbness and tingling in the hand, and/or an inability to straighten the arm.
Elbow Dislocation: An elbow dislocation is not common and usually occurs when a person falls onto an outstretched hand. When the hand makes contact with the ground, the force of the fall is transmitted to the elbow, which can rotate or twist it out of its socket. In other words, the bones of the elbow—the upper arm bone (humerus) and two bones from the forearm (radius and ulna)—are separated from their normal alignment.
Along with significant elbow pain, a dislocation often causes visible elbow deformity, swelling, and bruising around the joint. Some people also experience numbness and tingling of the hand.
How to Diagnose Elbow Pain?
- Physical examination and medical history
- X-rays
- CT scan
- MRI scan
- Electromyography (EMG)
- Biopsy of bursa fluid
Treatment of The Elbow Pain
- Changing how you move
- The first thing to do if you have elbow pain is to change, or possibly stop, any movements that might be causing your symptoms or making them worse. Flare-ups of some conditions, where the symptoms become suddenly worse, can be eased by avoiding bending the elbow into certain positions.
- Drugs to reduce pain
- Painkillers, such as paracetamol may help to ease pain. You should use them as and when you need them, but it’s best to take them before the pain becomes very bad.
- Non-steroidal anti-inflammatory drugs (NSAIDs) are a group of drugs that can help ease pain, swelling and stiffness. A common NSAID is ibuprofen, which you can buy at chemists and supermarkets.
- If you have stomach problems after using pain relief or NSAIDs, you should stop taking the tablets and see your doctor. There are also anti-inflammatory creams or gels you can rub onto your elbow, which don’t cause stomach problems.
- Splints
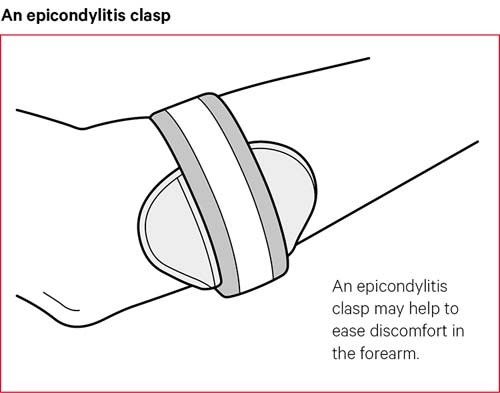
- For some conditions, such as tennis elbow, using a splint to support your elbow may ease the strain when you’re doing certain activities that cause it to flare up. They’re available from chemists, sports shops and physiotherapists. They’re also known as epicondylitis clasps. Ask a healthcare professional or a pharmacist if a splint would help you, and when and how you should wear it.
- Heat or ice packs
- Placing a heat or ice pack to your elbow for 10 to 15 minutes every few hours can ease pain and stiffness. You can use a reusable pad, a microwavable wheat bag or a hot water bottle. A bag of frozen peas can also be helpful if you don’t have an ice pack.
- Make sure you don’t put either a heat or an ice pack directly onto your skin, as this could burn or irritate it. You should wrap them in something like a tea towel first.
- Heat encourages blood to flow to a part of the body, and this can ease stiffness, encourage recovery of damaged tissue, and relieve pain. Don’t apply heat to your elbow if it’s swollen or if you’ve just injured it, as this can make it worse.
- Ice reduces blood flow to part of the body, and this can reduce swelling.
- Exercises
- To prevent your elbow joint stiffening and your arm muscles weakening it’s best not to rest for more than a few days. Start some gentle exercise as soon as the pain begins to ease. Simple exercises can help restore your range of movement, maintain your strength and ease stiffness.
- We have some examples of simple stretching and strengthening exercises.
- Start by exercising very gently and gradually build up the amount you do. It’s normal to feel muscle ache after exercise but stop if you get any joint pain that doesn’t go away quickly.
Home Remedies for Elbow Pain
Home Remedies vary depending on the elbow disorder and symptoms you experience. Most elbow disorders require conservative treatment. Surgery is a last resort if your symptoms don’t improve.
- Your treatment options include:
- ice
- rest
- non steroidal anti-inflammatory drugs (NSAIDs)
- Physiotherapy
- braces or immobilization
- steroid injections
- elbow padding
PHYSIOTHERAPY TREATMENT:
- Physiotherapy may be useful to help build up the strength in your elbow and prevent the condition returning.
- Physiotherapists are trained specialists who can help people with an injury or long-term health condition be active and independent.
- Your physiotherapist will help you keep up or regain flexibility in your elbow through exercise. You should stretch out your elbow at least once a day and do general range-of-movement exercises. Your physiotherapist might also recommend biceps and triceps strengthening exercises with light weights or resistance bands.
- An occupational therapist can identify movements that may be causing discomfort. They can look at activities you find difficult and see if there’s another way you can do them so you can maintain daily living and working skills.
- Exercises for pain relief.
1) Fist clench:
- Equipment needed: table and towel
- Poor grip strength is a common symptom of tennis elbow. Improving grip strength by building the muscles of the forearm can help improve ability to perform daily activity.
- Muscles worked: long flexor tendons of the fingers and thumb
- Sit at a table with your forearm resting on the table.
- Hold a rolled up towel or small ball in your hand.
- Squeeze the towel in your hand and hold for 10 seconds.
- Release and repeat 10 times. Switch and do the other arm.
2) Supination with a dumbbell:
- The supinator muscle is a large muscle of the forearm that attaches into the elbow. It’s responsible for turning the palm upward and is often involved in movements that can cause tennis elbow.
- Equipment needed: table and 2-pound dumbbell
- Muscles worked: supinator muscle
- Sit in a chair holding a 2-pound dumbbell vertically in your hand with your elbow resting on your knee.
- Let the weight of the dumbbell help rotate the arm outward, turning the palm up.
- Rotate the hand back the other direction until your palm is facing downward.
- Repeat 20 times on each side.
- Try to isolate the movement to your lower arm, keeping your upper arm and elbow still.
3) Wrist extension:
- The wrist ex tensors are a group of muscles that are responsible for bending the wrist, like during the hand signal for stop. These small muscles that connect into the elbow are often subject to overuse, especially during racquet sports.
- Equipment needed: table and 2-pound dumbbell
- Muscles worked: wrist ex tensors
- Sit in a chair holding a 2-pound dumbbell in your hand with your palm facing down, resting your elbow comfortably on your knee.
- Keeping your palm facing down, extend your wrist by curling it towards your body. If this is too challenging, do the movement with no weight.
- Return to starting position and repeat 10 times on each side.
- Try to isolate the movement to the wrist, keeping the rest of the arm still.
4) Wrist flexion:
- The wrist flexors are a group of muscles that work opposite the wrist extensors. These small muscles that connect into the elbow are also subject to overuse, leading to pain and inflammation.
- Equipment needed: table and 2-pound dumbbell
- Muscles worked: wrist flexors
- Sit in a chair holding a 2-pound dumbbell in your hand with your palm facing up and elbow resting comfortably on your knee.
- Keeping your palm facing up, flex your wrist by curling it towards your body.
- Return to starting position and repeat 10 times on each side.
- Try to isolate the movement to the wrist, keeping the rest of the arm still.
5) Towel twist:
- Equipment needed: hand towel.
- Muscles worked: wrist extensors, wrist flexors.
- Sit in a chair holding a towel with both hands, shoulders relaxed.
- Twist the towel with both hands in opposite directions as if you are wringing out water.
- Repeat 10 times then repeat another 10 times in the other direction.

12 Comments