
Cubitus Varus Deformity:
Table of Contents
What is Cubitus Varus Deformity?
Cubitus varus deformity is a condition in which the forearm is bent towards the body, causing the hand to turn inward. This can occur due to a congenital abnormality, injury, or bone development issues. Treatment options range from physical therapy to surgery, depending on the severity of the condition.
INTRODUCTION:
- Cubitus varus (varus means a deformity of a limb in which part of it is deviated towards the midline of the body) is a common deformity in which the extended forearm is deviated towards midline of the body.
- cubitus varus is the most common complication following a Supracondylar Humerus fracture.
- originally, causes of cubitus varus was thought to occur because of growth disturbance of distal humeral epiphysis.
- cubitus varus produces a cosmetic deformity but little function deficit.
- during reduction, a small amount of medial or lateral displacement or small amount of anterior or posterior angulation may be tolerated, but any malrotation is not acceptable.
- rotation is verified under flouro w/ AP view, lateral view, & oblique views.
- if reduction is not be obtained, there may be soft-tissue interposition which mandates open reduction.
- Supracondylar fracture of the humerus is one of the most talked about and often encountered injury (only after clavicle and both bone forearm fracture) in pediatric age group with a male predominance accounting for 16% of all pediatric fractures and 60% of all pediatric elbow fractures, classically occurring as a result of fall on an outstretched hand.
- Immediate complications associated with it are limb threatening (by virtue of involving neurovascular structures) whereas late complications are a serious concern to functional status of the patient.
- Due to the above reasons they require a strict vigilance and a proper management protocol. In pediatric age group the more common age of presentation is 5-7 years (90% cases). Extension type injury is more common than flexion type. It is frequently found in the non-dominant extremity. The flexion type is common in elderly children. Certain studies have reported up to 30% incidence of open fractures in this subset of patient.

DEFINITION:
- Cubitus varus deformity may occur after both pediatric supracondylar and lateral condyle fractures. Although simply termed “cubitus varus,” the deformity is a combination of varus, extension, and internal rotation.
- Indications for corrective osteotomy and timing of surgery have not been well established in the pediatric population.Pediatric cubitus varus has traditionally been considered a cosmetic problems with very few, if any, functional deficits or pain.
- Although it is well reported in the adult orthopedic literature that cubitus varus following a pediatric distal humerus fracture or congenital deformity can lead to posterolateral rotatory instability (PLRI),ulnar neuropathy,snapping triceps,progressive varus of the ulna,and elbow joint malalignment as an adult.Children with cubitus varus typically have minimal loss motion although the arc of motion may be altered to increased hyper extension and decreased elbow flexion.
- Increased susceptibility to lateral condyle fractures has been suggested with cubitus varus deformity.Remodeling of the very young, skeletally immature elbow may restore loss of elbow flexion.In contrast to children, adults with cubitus varus typically present with symptomatic complaints of lateral elbow pain and recurrent instability that do not become apparent until decades after the development of the cubitus varus.
ANATOMY:
Bone
- In children, the supracondylar region consists of a weak, thin bone located in the distal humerus.
- This area is bordered posteriorly by olecranon fossa, anteriorly by coronoid fossa and on both sides by respective supracondylar ridges.
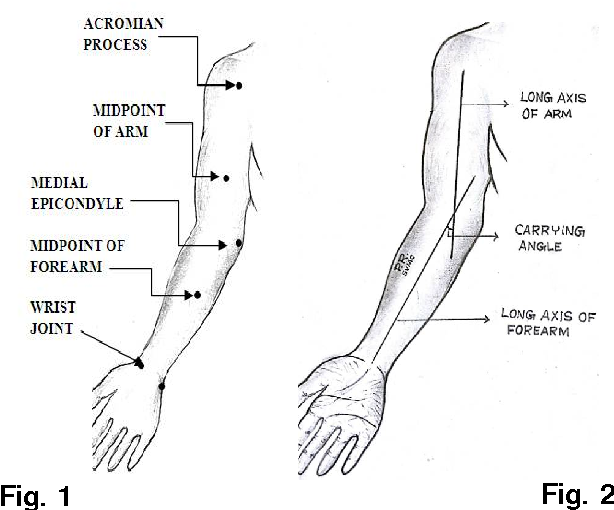
- The medial and lateral supracondylar ridges end into respective condyles and epicondyles. The trochlea is normally tilted 4° valgus in males and 8° valgus in females (carrying angle).
- The trochlea is also 3-8° externally rotated, resulting in external rotation of the arm when is flexed to 90°.
Soft tissue structures
- Both supracondylar ridges, condyles and epicondyles give rise to attachment of various muscles which are responsible for the displacement and rotation of distal fragment.
- Neurovascular structures lie in proximity to supracondylar region.
- Brachial artery which commonly gets involved in supracondylar fracture of humerus lies along the antero-medial aspect of distal humerus just superficial to the brachialis muscle.
- Major neurological structures of the upper limb (median, radial and ulnar nerves) are also in close relation with supracondylar region.
PATHOANATOMY:
- The ossification process of distal humerus occurs at different ages. The first to appear is capitulum at 1 year of age.
- The radial head and medial epicondyle begins to ossify at 4-5 years of age, followed by trochlea and olecranon epiphysis at 8-9 years of age.
- The lateral condyle is generally the last to appear at approximately 10 years of age. The supracondylar area undergoes remodeling between 6 to 7 years of age and is typically thinner with a more slender cortex, predisposing this area to fracture.
- As elbow forced into extension, the olecranon serves as a fulcrum and focuses the stress on the distal humerus causing fracture.
BIOMECHANICS:
- Varus malalignment of the upper extremity leads to medial displacement of the mechanical axis of the upper extremity.
- With repetitive varus forces on the elbow from activities of daily living, such as pushing up from a sitting position, the lateral collateral ligament complex experiences increased tensile forces and becomes attenuated, leading to further medial displacement of the mechanical axis.
- A biomechanical demonstrated that increased cubitus varus deformity does indeed lead to increased LUCL strain and increased ulno-humeral widening even in the presence of an intact LUCL.
- The triceps is displaced medially in cubitus varus, and this displaced triceps force vector leads to an external rotation (supination) moment arm on the ulna.
- Chronic medial triceps forces on the olecranon lead to medial elongation of the olecranon and external rotation of the ulna, which is the first stage of PLRI.
- Because of both of these biomechanical alterations, continued LUCL attenuation and olecranon external rotation eventually leads to radial head subluxation and eventually dislocation with frank PLRI.
MORPHOLOGY:
- Three-dimensional computed tomography scans have verified that morphological changes in the elbow joint do occur in elbows with cubitus varus. When compared with the contra lateral, uninjured elbow, elbows with cubitus varus show trochlear overgrowth posteriorly, leading to increased internal rotation of the posterior joint line of the distal humerus.
- The proximal ulna accommodates the trochlear overgrowth, with a lateral shift of the convex part of the trochlear notch and a longer articular surface from anterior to posterior.
- The ulna shifts to a more distal and medial position accompanied by increased external rotation and flexion when compared with the contra lateral ulna.
- In addition, the lateral aspect of the capitellum overgrows distally and diameter of the radial head enlarges, although not enough to lead to increased cubitus varus.
- It is hypothesized that the medial over pull of the triceps leads to these bony morphological changes, although it is possible that this may also be a sequel of physeal trauma to the elbow.
- Tardy ulnar nerve palsy with anterior dislocation of the nerve has also been reported in conjunction with cubitus varus.It is thought that the internal rotation deformity of the distal humerus in conjunction with distal fibrosis and entrapment of the nerve affects the position and stability of the nerve; in these cases, ulnar nerve transposition is recommended in conjunction with corrective osteotomy.
- Similarly, snapping of the medial portion of the triceps may occur from the medial displacement of the triceps as well as the internal rotation of the distal humerus.
SURGICAL CORRECTION:
There are multiple reported techniques for the correction of cubitus varus:
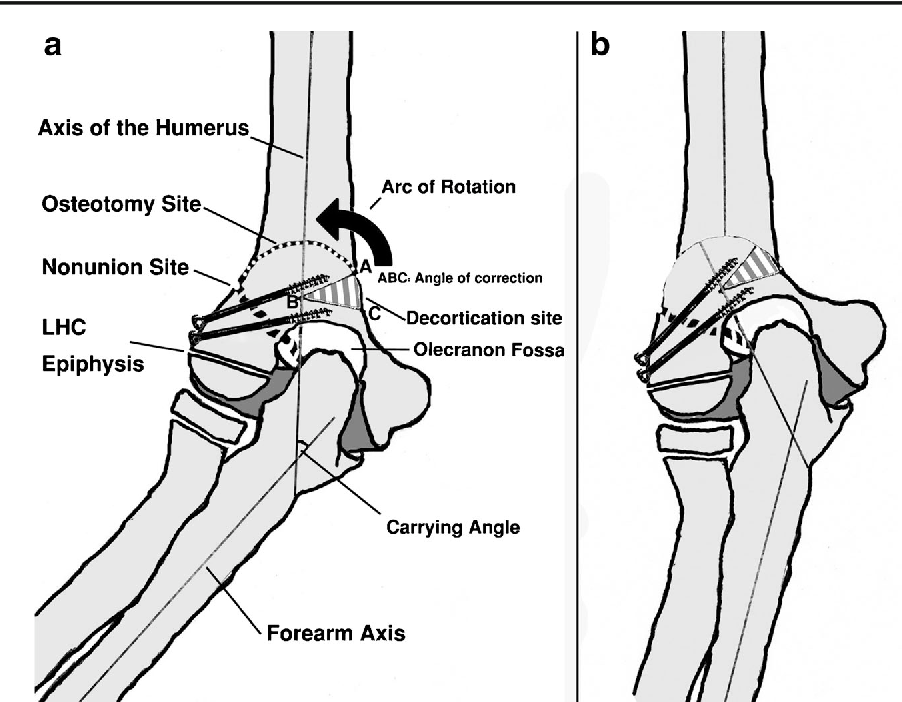
1)the lateral closing wedge osteotomy.
2)step-cut osteotomy.
3)dome osteotomy.
4)external fixation with distraction osteogenesis.
5) computer-aided multi planar osteotomy.
- Corrective osteotomy in the distal humerus is a less technically demanding surgery in the pediatric population when compared with adolescents and adults.
Treatment of Cubitus varus deformity:
Advice and Exercises During the Immobilization Period:
- Normally elbow is immobilized for 3 weeks so, during that period, adjacent joints ( Shoulder joint and wrist joint, and hand) should be kept moving actively or active-assisted exercises frequently during the day.
- The elbow shouldn’t be moved and the use of an arm sling should be proper.
- Postural training( sitting upright with a relaxed shoulder and retraction of the scapula) should be taught.
1-2 Weeks After Removal of Cast:
- Hot fermentation can be used to ease joint stiffness.
- Gentle soft tissue release can be done in the arm and forearm musculature.
- Gentle active and active-assisted exercises using a wand and be taught in pain-free limit- frequently in a day.
- Isometric exercises for arm and forearm musculature can be addressed.
- Educate parents and children to use the affected hand to use in daily activities like brushing, writing, eating, dressing, etc.
- Avoid weight lifting and pushing activities.
Advice and Exercise After 2 Weeks of Cast Removal:
- Progressive and interactive range of motion exercises and strengthening exercises should be addressed.
- eg: passing a ball, dressing and undressing clothes.
PHYSIOTHERAPY MANAGEMENT:
- To achieve painless and full mobility of the elbow joint.
- To enhance the healing process.
- To strengthen the affected musculature.
- To improve the overall functional abilities of children.
Outcome measures that can be used to compare and evaluate the outcome of treatment are:
- Numerical pain rating scale (NPRS)/ Faces Pain Scale
- Range of motion- Goniometry
- Manual muscle testing ( MMT)
PHYSIOTHERAPY TREATMENT:
- Background: Physiotherapeutic intervention in a phasic manner has been in practice after orthopedic surgeries. graded physiotherapy has great value in reducing post-surgical inflammation pain and improving mobility .this work is done towards presenting the data regarding the post-surgical condition of corrective osteotomy for cubital varus on the left side the treatment techniques were chosen on the basis of phasic evaluation and post-treatment evaluation was done in order to check the prognosis in terms of inflammation, pain and ROM .several exercise therapeutic techniques and electro therapeutic techniques have been selected periodically on a basis of pre-treatment assessment. In this data presentation electro therapeutic techniques like,faradism under tension for correction of deformity, TENS, ULTRASOUND, and PARAFFIN WAX BATH (pain relief and extensibility) were the treatment modalities selected.
- Method: Treatment techniques were selected based on the evaluation in every particular session. faradism under pressure, Paraffin wax bath, TENS, muscle energy techniques, cyriax deep friction massage, and ultrasound therapy modalities were used selectively.
- Results: Faradism under tension, Paraffin wax bath, TENS, muscle energy techniques, cyriax deep friction massage and ultrasound therapy modalities were used selectively with a range of movement exercises in four phases, and evaluation was done in every session. each phase was of 3 days at the end of 12 days re evaluation was done and found that there was a marked decrease in pain, inflammation, and increased range of motion.
- Conclusion: After the selective physiotherapy approaches there was a reduction of pain, and edema, and the range of motion was improved. graded physio-therapeutic intervention is important to most orthopedic post-operative conditions in reducing pain, decreasing inflammation, and increasing mobility.
- Keywords: CYRIAX deep friction massage, faradism under tension, muscle energy techniques.
- TOOLS: Inch tape, goniometer




One Comment