

Tardy ulnar nerve palsy: Physiotherapy Treatment
Table of Contents
INTRODUCTION
Tardy ulnar nerve palsy is a chronic clinical condition characterized by a delayed onset ulnar neuropathy
after an injury to the elbow.
In 1878, Panas first described what is now often called tardy ulnar palsy, in which either prior trauma or osteoarthritis gradually caused damage to the ulnar nerve. Additional cases were reported over the ensuing decades, usually associated with trauma (eg, fractures in the elbow region) and typically occurring in the epicondylar groove. , Initially denoting time (ie, appearing years after trauma), the term came to have an anatomic connotation (eg, usually seen in or very near the epicondylar groove).
Typically, tardy ulnar nerve palsy occurs as a consequence of nonunion of pediatric lateral condyle fractures at the elbow, which eventually lead to a cubitus valgus deformity.
The clinical assessment includes obtaining a complete history, physical examination, nerve conduction tests, and elbow imaging studies.
Treatment of nerve palsy are Conservative Method Including Physiotherapy or Surgical – decompression, with or without corrective osteotomy, with overall success
What are the Causes Tardy ulnar nerve palsy?
- Nonunion of pediatric lateral condyle fractures at the elbow [ Cubitus valgus deformity ]
- Other childhood elbow trauma include;
- Supracondylar fractures [ cubitus varus ]
- Fractures of the medial condyle humerus
- Fracture of olecranon
- Fracture of redial head
- Monteggia fracture
Classification:
Primary and secondary ulnar neuritis resulting:
Simple contusion
- Recent fracture of the humerus, either in the medial epicondyle or in the supracondylar region
- Recent dislocation of the elbow joint
Tardy paralysis of the ulnar nerve due to involvement of the elbow region by :
- Old fracture
- Arthritis
- Congenital anomalies
- Old or recurrent dislocation
- Tumor
- Unknown factor
Which Symptoms are seen in Tardy ulnar nerve palsy?
- Discomfort localized to the medial elbow.
- Paresthesia or numbness in the ring and small fingers other hand.
- Decreased grip.
- Decreased pinch strength.
- Fatigue the hands with repetitive task movement
- Muscle paralysis or numbness in trady unlar nerve palsy is flexor carpi ulnaris, medial division flexor digitorum profundus
- 3rd and 4rd lumbrical muscles, hypothenar muscle [opponens digiti minimi, flexor digiti minimi
- abductor digiti minimi] ,interossei, adductor pollicis
This symptoms is increase in at night or with flexion of the elbow and talking on the telephone.
Physiotherapy Examination :
Observation: a. check the carrying angle because it is change due to cubitus varus and cubitus valgus [ mostly
typically between 5°and 15. ]
Check the intrinsic muscles of the hand [ Atrophy of muscle & particular, the first dorsal interosseous muscle atrophy ]
Check the fingers [Clawing of the small and ring fingers ]
Check the ROM [ shoulder , elbow , wrist , finger ]
Examination of sensory function [ static two-point discrimination and vibration test ]
Examination of moter function.
[hand grip , pinch strength, MMT of the flexor digitorum profundus, at the ringand little finger and of the intrinsic muscles of the hand ]
[Tinel’s sign and The elbow flexion-compression test]
For examination of muscle paralysis use the RD test:
In RD test use the ES machine with the current IG and SF
First of put the surface electrod after that use of the pen electrod apply current on moter ponit of muscle .
If the contraction occurs in muscle positive for current.
First check in IG current if IG current positive after that check the SF current.
If the SF current positive then the SD curve.
Diagnosis :
Imaging tests, such as a CT scan or MRI ].
Nerve conduction tests [ NCV test ]
Special test:
Froment’s sign:
It checks the adductor pollicis and first palmar interossei
For examination asked to patient hold an object [ like as piece of paper, book ]
Pen test
It is check the adductor pollicis brevis.
For examination asked to patient touch the pen.
Egawa test
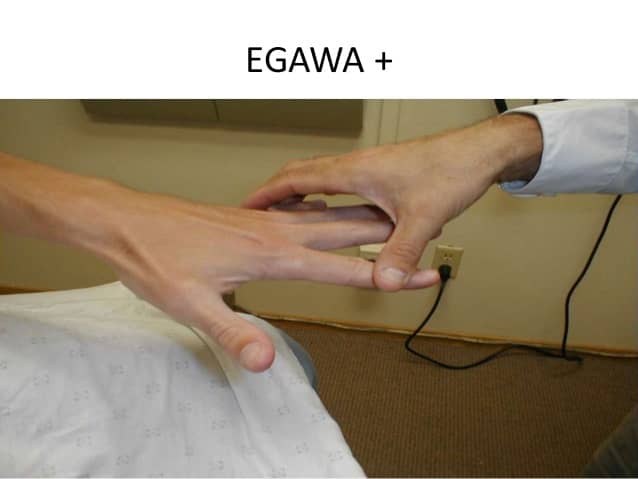
It checks the dorsal interossei
For examination asked to patient move the middle finger
Treatment
- Non-operative treatment is the first treatment option for mild-to-moderate cubital tunnel syndrome.
- Surgical treatment is recommended to correct the local bony deformity and/or to decompress the nerve.
- Supracondylar Osteotomy
- Every types of supracondylar osteotomy procedures have be en described for the treatment of tardy ulnar nerve palsy.
- Most popular procedures are the closing wedge osteotomy
Physiotherapy Treatment in Tardy ulnar nerve palsy :
Elbow ROM Exercise
Flexion Exercise:
Stand with your arm at your side.
Actively bend your elbow up as far as possible, then grasp your forearm or wrist with your other hand and gently add overpressure.
Hold the bent position of your elbow for five to 10 seconds, and then release the stretch by straightening your elbow.
Repeat the exercise 10 times.
Extension Exercise:
Sit in a chair with your elbow resting on a table. You may want to rest your upper arm on a pillow or folded towel for comfort.
Straighten your elbow out all the way, and then apply pressure to your forearm or wrist to add over pressure to the stretch.
Straighten your elbow out as far as you can with over pressure, and hold the stretch for five to 10 seconds.
Release the stretch and allow your elbow to bend a bit.
Repeat the exercise for 10 repetitions.
In starting pain free range exercise & strengthening exercise
Apply glide for the correct carrying angle.
[ humerus ulnar ulnar glide & humerus ulnar redial glide. ]
For sensory stimulation:
- Pinching
- Tapping
- Brushing
- Icing
Give to splint for clawing of a finger.
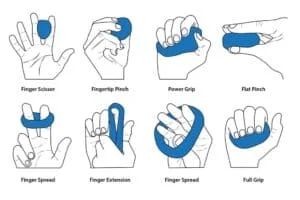
Grip strengthening exercise
Squeezing a Tennis or Racket Ball.
Standing Cable Row With a Towel.
Rubber-Band Exercise
Tip to tip, pad to pad, tip to pad exercise with use of paper, manual
Use the ES Machine for paresthesia of muscle.
- Expose the area of your body being treated.
- Your physiotherapist will apply electrodes to your hand.
- You will feel a slight tingling sensation.
- The sensation will be increased until it feels strong but comfortable.
Strengthening Exercise
Exercises for ulnar nerve entrapment at the elbow
- Start with your arm extended straight and your palm up.
- Curl your fingers inward.
- Bend your elbow, bringing your curled fist up toward your shoulder.
- Return to your starting position.
- Repeat the exercise 3 to 5 times, 2 to 3 times a day.
Exercises for ulnar nerve entrapment at the wrist
- Stand straight with your arms at your side.
- Raise the affected arm and rest your palm on your forehead.
- Hold your hand there for a few seconds and then bring your hand down slowly.
- Repeat the exercise a few times a day, gradually increasing the number of repetitions you do in each session.
Prevention tips:
- Using ergonomic strategies at work and at home
- Avoiding repetitive movements
- Avoiding movements that cause pain
- Treating underlying health conditions, such as diabetes or rheumatoid arthritis.

2 Comments