THE MULLIGAN MOBILIZATION TECHNIQUE : HANDS-ON MANUAL CONCEPT
THE MULLIGAN MOBILIZATION TECHNIQUE
Table of Contents
INTRODUCTION :
- Mulligan’s manual therapy technique at peripheral joints, namely mobilisation with movement (MWM), has been well documented in research for over a decade. The specific parameters of MWM prescription are relatively variable and generally ill defined. The purpose of this review was to critically evaluate the literature regarding MWM prescription at peripheral joints.
WHAT IS MOBILIZATION?
- The term “mobilization” is often used within the profession of Physiotherapy. Most often the term is used to describe a physical force that is applied to a pair of bones at their articulation (joint) in order to improve the ability of that joint to move.

ABOUT MULLIGAN CONCEPT:
> NAGS– Natural Apophyseal Glides.
> SNAGS – Sustained Natural Apophyseal Glides.
> MWMS– Mobilization with Movements.
> The concept of Mobilizations with movement (MWM) of the extremities and SNAGS (sustained natural apophyseal glides) of the spine were first coined by Brian R. Mulligan.
> Mobilization with movement (MWM) is the concurrent application of sustained accessory mobilization applied by a therapist and an active physiological movement to end range applied by the patient. Passive end-of-range overpressure, or stretching, is then delivered without pain as a barrier.

SOME KEY POINTS ABOUT MULLIGAN TECHNIQUE:
1. Mulligan techniques are often performed in weight-bearing
2. Mulligan techniques are generally sustained
3. Mulligan techniques are never performed through pain
4. Mulligan techniques must produce immediate improvements
> These attributes are partly what make Brian Mulligan’s methods so clinically effective.
COMMON INDICATION OF THIS CONCEPT:
- Pain of a non-inflammatory nature
- Acute pain from injury
- Loss of motion due to arthritic conditions
- Post-surgical conditions causing loss of pain-free movement, e.g. post scope conditions, spinal surgery
- Headaches due to neck problems
- Dizziness associated with neck problems
- Jaw or TMJ pain and movement restrictions
- Acute to chronic ankle sprains
- “Tennis elbow” or lateral elbow pain
PRINCIPLE OF MULLIGAN CONCEPT :
- While applying “MWMS” as an assessment, the therapist should look for a PILL response to use the same as a Treatment.
P- Pain-free.
I- Instant result.
LL- Long Lasting.
- If there is No PILL response, that technique should not be advocated.

- The second principle is CROCKS :
C- Contra-indications (No PILL response is a contraindication)
R – Repetitions (Only three reps on the day one)
O- Over pressure
C- Communications
K – Knowledge (of treatment planes and pathologies)
S- Sustain the mobilization throughout the movement.
TECHNIQUE :
- There is four technique used for pain relive :
1. NAGS
2. SNAGS
3. PMWM
4. SMWLMs
NAGS :
- NAGS involves a mid to end-range facet joint mobilisation applied anterocranially along the plane of treatment within the desired joint, combined with a small amount of manual traction. The purpose of this treatment is to increase movement within the spine, and decrease symptomatic pain.
- Sustained natural apophyseal glides (SNAGS) are a separate technique involving a combination of a sustained
- facet glide with active motion, which is then followed by overpressure.
- NAGs are used for cervical and upper thoracic spine.
- It consists of oscillatory mobilizations instead of sustained glide like SNAGs, and it can be applied to the facet joints between 2nd cervical and 3rd thoracic vertebrae.
- NAGs are mid range to end range facet joint mobilizations applied antero-superiorly along the treatment planes of the joint selected.
- Useful for grossly restricted spinal movement.
- NAGs for the treatment of choice in highly irritable conditions.

SNAGS :
- SNAGs can be applied to all the spinal joints, the rib cage and the sacroiliac joint.
- The therapist applies the appropriate accessory zygapophyseal glide while the patient performs the symptomatic movement.
- This must result in full range pain free movement.
- SNAGs are most successful when symptoms are provoked by a movement and are not multilevel.
They are not the choice in conditions that are highly irritable. - Although SNAGs are usually performed in weight bearing positions they can be adapted for use in non weight bearing positions.

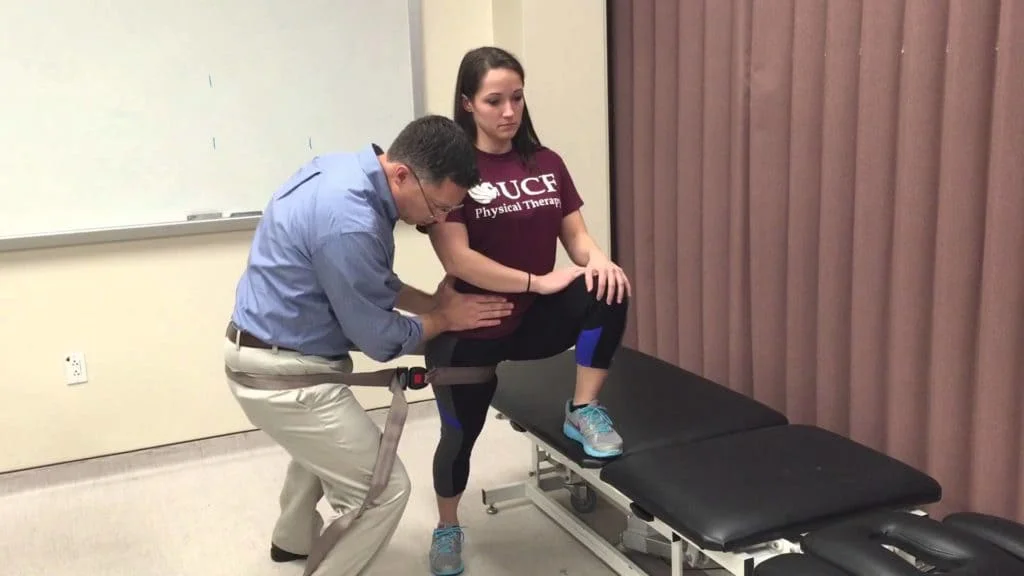
PMWM ( Peripheral MWM ):
- The use of mobilisations with movement (MWM) for peripheral joints has been developed by Mulligan. A mobilisation is applied parallel or at right angles to the restricted joint movement. If the applied mobilisation achieves immediate improvement in the functional movement and abolishes the pain the treatment involves sustaining the mobilisation while the patient performs the active movement repetitively. On reassessment of the joint function, the movement should remain improved without the mobilisation. Theories as to why these techniques provide rapid improvement in pain-free range are proposed, and the general principles of examination and treatment are outlined. Specific clinical examples demonstrate how MWM can be used in isolation or integrated with other manual approaches to improve the quality of joint intraarticular gliding, neurodynamics and the facilitation of correct muscle recruitment.
- Once the aggravating movement has been identified, an appropriate glide is chosen.
- Decision to use weight-bearing or Non-weight bearing movement depends upon the severity, irritability and nature of the condition.
- Once the glide has been chosen it must be sustained throughout the physiological movement until the joint returns to its original starting position.
- Mobilizations performed are always into resistance but without pain.
- Immediate relief of pain and improvement in range of motion (ROM) are expected.
- If this is not achieved, vary the glide parameters.

SMWLMs :
- Here a transverse pressure is applied to the side of the relevant spinous process as the patient concurrently moves the limb through the previously restricted range of movement.
- The assumption here is that the restriction of movement is of spinal origin of course.
- This does not necessarily imply neural compromise since spinal movement must occur when a limb moves beyond a certain point.
- Thus the technique addresses a spinal structural/ mechanical restriction, but this may have neural implications too.