

Snapping Triceps Syndrome
Table of Contents
What is Snapping Triceps Syndrome?
Snapping triceps syndrome, also known as triceps tendon subluxation, is a condition characterized by the snapping or popping sensation in the back of the elbow during certain movements. It occurs when the triceps tendon, which connects the triceps muscle to the ulna bone in the forearm, temporarily slips out of its normal position.
The triceps muscle extends the elbow joint. In snapping triceps syndrome, the tendon may shift out of its groove and move either medially (towards the midline of the body) or laterally (away from the midline) during arm movement. This abnormal movement can result in a snapping sensation, often accompanied by pain and discomfort.
The elbow joint is a complex hinge joint that connects the upper arm (humerus) to the forearm bones (radius and trochlear). The triceps muscles are divided into three parts: the long head, the lateral head, and the medial head. In general, the three muscles combine to produce one large tendon that attaches to the tip of the elbow. Some people, however, have an extra tendon from the muscle’s inside or medial side.
Snapping elbow should be known as snapping triceps syndrome. When you bend your elbow, you can snap your triceps. The inside of the triceps will snap against the inside of the elbow during elbow flexion. Snapping is more probable if there is an extra tendon from the medial triceps. If this snapping occurs regularly, pain develops inside the elbow, resulting in elbow pain. Furthermore, the ulnar nerve is adjacent to the snapping muscle, generating pins and needles and numbness on the outside of the hand.
Anatomy of Elbow:
As the name suggests, the triceps muscle is divided into three different parts: the lateral, long, and medial heads. A fourth, medial head of the triceps muscle has also been described in rare situations. The three leaders work together to form a single tendon distally.
The lateral head develops from three locations on the humerus. The long head arises from the scapula’s infra glenoid tuberosity, while the medial head arises from the posterior humerus distal to the spiral groove.
Proximally, the triceps inserts with both tendon and muscle. The tendinous segment that inserts on the olecranon is referred to as the proper part. The expansion inserts at four places: the posterior crest of the ulna medially, the fascia of the extensor carpi ulnaris origin laterally, the antebrachial fascia distally, and the anconeus insertion deeply.
The site of the transition between the muscular and tendinous insertions of the medial head is important in the snapping triceps since the distance between the medial border of the triceps muscle and the medial epicondyle becomes less with a more distal transition. A tiny gap between the medial edge of the triceps and the medial epicondyle predisposes to triceps snapping. This is an important factor during a clinical evaluation. The fourth, medial head of the triceps muscle and an aberrant musculotendinous component of the triceps in the ulnar groove have also been described as likely anatomical explanations of snapping triceps syndrome.
The ulnar nerve consists of nerve roots C8-T1. From the middle of the humerus, the ulnar nerve passes posterior to the intermuscular septum and anterior to the medial head of the triceps. The nerve enters the cubital tunnel at the elbow, which is formed by the medial epicondyle and the cubital tunnel retinaculum. The ulnar nerve connects the medial edge of the triceps to the medial epicondyle. A shallow groove or lacking the cubital tunnel retinaculum are two possible anatomical responses of an ulnar nerve dislocation.
What are the Causes of Snapping Triceps Syndrome?
There are numerous probable causes, some of them are as follows:
- Instability of the medial side of the elbow: This can be caused by a subluxation of the ulnar nerve or the triceps tendons.
- Instability of lateral ligaments: This consists of the annular ligament, meniscus, and synovial plica injury.
What are the Symptoms of a Snapping Triceps Syndrome?
Snapping the triceps elbow is frequently accompanied by visible symptoms that resemble a variety of other elbow conditions.
Some of the symptoms are as follows:
- The most noticeable symptom is a snapping or popping sound and sensation that occurs with the movement of the elbow joint. It can occur during actions such as bending or extending the elbow.
- Snapping the triceps elbow can cause pain on the inside of the elbow, which can vary in intensity. The discomfort is usually limited to the inside of the elbow, where the ulnar nerve runs.
- Pins and needles or numbness in the little and ring fingers. This happens because ulnar nerve snapping or subluxation can produce transient nerve compression or discomfort.
- Individuals can notice weakness or a loss in grip strength in some circumstances. This could be due to nerve compression impairing the function of muscles innervated by the ulnar nerve.
- Inflammation around the ulnar nerve can cause localized swelling, tenderness, or redness on the inside of the elbow joint.
How is a Snapping Triceps Syndrome Diagnosed?
Given the enigmatic nature of snapping triceps syndrome, the necessary evaluation might include one or more of the following:
Physical examination and medical history: Inform your doctor about any potential activities that may have caused an injury, such as trauma, exercise, or sports. A physical examination, such as the elbow flexion test, can also be done to assess the extent of injury in the impacted area.
Arthroscopy: Arthroscopy includes inserting a small camera into the elbow joint to examine the condition of the affected elbow joint.
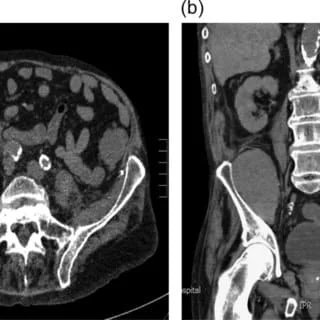
Imaging studies: Magnetic resonance imaging, dynamic ultrasound, and even computed tomography may also be utilized to help identify snapping triceps syndrome. Magnetic resonance imaging could be performed in extension and flexion if possible. In some situations, it may demonstrate inflammation of the triceps medial head or edema of the medial epicondyle. Ultrasound is frequently more accessible, and its dynamic features outperform magnetic resonance imaging. It is best to conduct the ultrasonic examination while actively extending against resistance.
Differential diagnosis: Compression of the ulnar nerve in the cubital tunnel, or a prominent medial head of the triceps, can produce symptoms similar to snapping triceps syndrome, including medial-sided elbow pain and paresthesias. Ulnar nerve symptoms can occur along with snapping triceps syndrome, however, the ulnar nerve does not snap in the much more common ulnar nerve compression.
Golfer’s elbow, also known as medial epicondylitis, is another common disease that causes pain on the medial side of the elbow. Ulnar nerve symptoms, like those seen in snapping triceps syndrome, can occur in a patient with medial epicondylitis. The major pathology, however, is located at the insertion of the flexor-pronator group rather than the medial triceps. Although distal triceps rupture is uncommon, it should be considered in the differential diagnosis. Patients frequently have a history of a single snap. There is pain and edema, but most importantly, there is a lack of complete active extension and a palpable deformity.
Treatment of Snapping Triceps Syndrome
Treatment for snapping triceps syndrome typically involves a combination of conservative measures and, in severe cases, surgical intervention. The initial management may include:
Rest and activity modification: Avoiding activities that provoke symptoms and giving the elbow adequate rest can help reduce irritation and promote healing.
Physical therapy: Strengthening exercises for the triceps muscle, stretching, and range of motion exercises may be prescribed to improve muscle balance and stability around the elbow joint.
Nonsteroidal anti-inflammatory drugs (NSAIDs): Over-the-counter medications like ibuprofen or naproxen can help alleviate pain and reduce inflammation.
Surgical Treatment:
Arthroscopic surgery: Elbow arthroscopy is frequently used to treat this disease. An anterior transposition of the ulnar nerve, excising the plica (tissue excision), or loosening capsule tissues are all surgical options.
Post-operative Treatment:
- You must get out of the sling as soon as possible following surgery to move your elbow. Bend and straighten your elbow as much as you can, then hold it there for 10 seconds. Do 10 repetitions of this, 10 times per day (100 reps).
- You can start by rotating your forearm so that your palm faces the ceiling, then the other way so that your palm faces the floor while keeping your elbow firmly by your side. These are known as pronation and supination exercises. However, do not press this movement with the other hand or if there is pain until 4 weeks after surgery.
- At this time, please do not lift anything heavier than a cup of tea.
- Early mobility is vital to avoid stiffening your elbow or to reduce any pre-existing stiffness as fast as possible.
- Although early movement may be difficult or painful, you must try to move it.
- You should be removed from the sling over the next three days and out of it entirely by the end of the first week after surgery.
- At 4 weeks after surgery, you can begin passive supination and pronation exercises, as well as strengthening exercises, with your therapist.
Non-Surgical Treatment:
Physiotherapy Treatment:
- Increase joint mobility
- Reduce muscular tightness
- Soft tissue mobilization
- Joint mobilization
- Instrument-assisted soft tissue mobilization (IASTM)
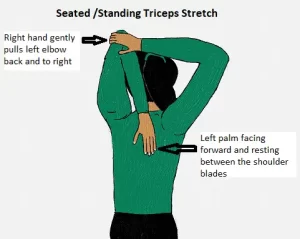
Stretch tight muscles: Triceps Stretch
Place your arm up and fully bend your elbow, as long as the movement is painless. On the back of your upper arm, you should feel a stretching sensation. Use your other hand to keep this position.
Hold for 30 seconds, repeat 2-3 times. 2-3xday.
Strengthen the muscles: Wrist lift, palm up
Grip a lightweight, such as a small dumbbell, bend the elbow at a right angle, stretch the hand outwards, palm up, bend the wrist up towards the body, hold for 5 seconds, then slowly release.
Perform two more sets of ten repetitions.

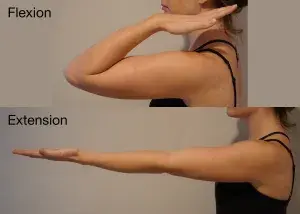
Increase your range of motion:
Flexion: Bend the elbow without using the opposite hand.
Hold for 3 seconds. Rep 10 times more. 3 times each day
Extension: Straight the elbow without using the opposite hand.
Hold for 3 seconds. Rep 10 times more. 3 times each day
Therapeutic methods such as ultrasound, electrical stimulation, heat or cold therapy, or laser therapy may be used to assist relieve pain and inflammation and promote tissue healing.
Summary:
Triceps snapping is a rather uncommon ailment. Recognizing snapping triceps syndrome is critical, beginning with understanding the condition’s indications and symptoms. The patient will complain of painful snapping or, in rare cases, only ulnar nerve symptoms. There is virtually little published data on this condition. Although a clinical examination will define the diagnosis and subsequent course of treatment, dynamic ultrasonography is likely the quickest and least expensive imaging modality to unbiasedly document a snapping triceps. Ulnar neuropathy, medial epicondylitis, and distal triceps rupture should all be ruled out when evaluating the reason for a snapping triceps.
A conservative treatment plan of 3 to 6 months is indicated. This should include anti-inflammatory medications as well as the cessation of any activities that cause snapping. If conservative treatment is ineffective, surgery is the best alternative. The snapping part of the medial triceps is removed during surgery. Surgery produces good to outstanding results in well-chosen patients.
Snapping triceps should be considered in the differential diagnosis of medial elbow pain, especially if ulnar nerve dislocation is present or suspected.
FAQs:
Can snapping triceps syndrome be prevented?
While some causes of snapping triceps syndrome may not be preventable, there are a few steps you can take to potentially reduce the risk or severity of symptoms. These include maintaining good muscle strength and flexibility around the elbow joint, practicing proper ergonomics and body mechanics during activities, and avoiding repetitive or excessive stress on the elbow.
Is snapping triceps syndrome a serious condition?
In most cases, snapping triceps syndrome is not a serious condition and can be managed with conservative treatments. However, if the snapping is accompanied by severe pain, locking of the joint, or if you have difficulty using your arm, it’s important to seek medical attention as it could indicate a more significant issue.
What are the treatment options for snapping triceps syndrome?
Treatment for snapping triceps syndrome depends on the underlying cause. Conservative measures often include rest, activity modification, ice, non-steroidal anti-inflammatory drugs (NSAIDs), and physical therapy to address muscle imbalances and improve joint stability. A splint or brace may be recommended. If conservative treatments fail to alleviate symptoms, or if there is a structural problem, surgical intervention may be considered.



One Comment