15 Best Foot Drop Exercises: How to Strengthen Your Foot and Ankle
Foot drop exercises play a crucial role in the management and recovery of this condition, as they help strengthen the muscles and improve nerve function in the lower limbs.
In this guide, we will explore a range of exercises designed to address foot drop and enhance mobility, ultimately improving the quality of life for individuals dealing with this condition.
Table of Contents
Introduction
Foot drop, also known as drop foot, is a medical condition characterized by difficulty lifting the front part of the foot. It may be caused by a number of underlying factors, including neurological disorders, muscle weakness, and nerve injury. Foot drop can lead to tripping, stumbling, and difficulty walking, which can impact one’s mobility and quality of life.
Fortunately, there are exercises and rehabilitation techniques designed to help manage and improve the symptoms of foot drop. These exercises aim to strengthen the muscles involved in lifting the foot and improve flexibility and coordination.
When performed regularly under the guidance of a healthcare professional, these exercises can be a valuable part of a comprehensive treatment plan for individuals with foot drop. In this guide, we will explore a range of exercises and stretches tailored to address foot drop, enhancing strength, mobility, and overall function in the affected foot and ankle.
What is a Foot Drop?
A disorder that makes it difficult to lift the front of the foot and toes is known as foot drop. It frequently causes problems walking since the person is more likely to fall if their foot drags or their toes stay on the ground. Fortunately, there are a variety of techniques for regaining foot strength and mobility, and one of the greatest ones involves performing foot drop exercises.
In certain circumstances, the symptoms of foot drop can be relieved by performing particular exercises that strengthen the muscles in the foot, ankle, and lower leg. Exercise is a powerful strategy to prevent foot drop after a stroke or brain injury because it may stimulate and reorganize the brain. Exercises are crucial for preventing injury, increasing balance and gait, enhancing range of motion, and reducing muscular stiffness.
You might work with a physical therapist to treat foot drop, who will assist you in beginning to strengthen your foot, leg, and ankle muscles. Since recovery from foot drop might take time, your physical therapist will probably advise you to keep performing strengthening exercises on your own at home.
You can start walking normally again by restoring normal function by strengthening the weaker muscles.
Please speak with a healthcare professional before starting any workout regimen. If any of the following activities hurt your body or cause you discomfort, please stop right once. For guidance and safety, working with a qualified specialist is recommended.
Why Does the Foot Drop occur?
Foot drop is brought on by a lack of strength or paralysis on one side of the body, typically due to a brain or nerve disorder. Foot drop can also occur when the nerves in your leg are damaged.
Foot drop is frequently brought on by a variety of factors, including but not restricted to:
- Stroke
- Neck or spinal cord injury
- Sciatica
- Damage to the peroneal (lower leg) nerve
- Transverse myelitis
- Multiple sclerosis
Treatment:
Orthotics:
There are numerous types of orthotics available, including braces and splints. While some are worn within the shoes, others are worn close to the knee or around the ankle.
Lightweight orthoses, which come in molded plastic and softer materials with elastic qualities to avoid foot drop, help support the ankle joint. Traditional spring-loaded braces can also be installed on shoes to stop foot drop during walking.
Ankle foot orthosis:
Ankle-foot orthoses are one common type of device (AFO). It supports the lower leg by keeping the foot at a 90-degree angle to it. Even while it may help with gait improvement, you might need to have a larger shoe to fit the brace. Additionally, using an AFO for extended periods of time may cause discomfort.
When surgery is not necessary or when recovering from surgery or neurologic conditions, an AFO may be utilized for foot drop. An AFO is specifically designed to give toe dorsiflexion during the swing phase, ankle stability during stance (medial or lateral), and pushoff stimulation (if needed) during the late stance phase. An AFO may be beneficial, only when the patient’s foot can reach plantigrade position when patient is standing. Any equinus contracture precludes successful use.
The most popular AFO for foot drops is made of polypropylene and it fits inside a shoe. It offers stiff immobilization if trimmed to fit in front of the malleoli. When ankle spasticity or instability is an issue, as it often is in individuals with stroke or upper motor neuron illnesses, this device is used.
If the AFO fits posterior to the malleoli (posterior leaf spring type), plantarflexion at heel striking is permitted and pushoff puts the foot back in neutral for the swing phase. In cases of moderate or flaccid spastic equinovarus deformity, this assists with dorsiflexion. Another option is to utilize a shoe-clasp orthosis, which fastens straight to the shoe’s heel counter.
From the study it is suggested that anterior AFOs are associated with less energy costs of walking and higher levels of perceived comfort than posterior AFOs are and thus may allow people with foot drop to walk at longer distances while using less physical effort
A simple “L” shaped foot-up ankle support (ankle-foot orthoses) can be the only treatment needed for certain individuals. An alternative technique involves encircling the patient’s ankle with a cuff and inserting a topside spring and hook beneath their shoelaces. As the patient walks, the hook attaches to the ankle cuff and raises the shoe.
Functional electrical stimulation:
Utilizing electrical currents to stimulate nerves innervating extremities afflicted by paralysis due to spinal cord injury (SCI), head injury, stroke, and other neurological illnesses is known as functional electrical stimulation or FES. The main purpose of FES is to help disabled individuals regain their function. The term neuromuscular electrical stimulation (NMES) is occasionally used to describe it.
The peroneal nerve, which raises the foot with each step, is stimulated in the most recent treatments. Many people with foot drop who have had strokes or multiple sclerosis have found success with it. Instead of wearing a brace or splint, people with foot drop frequently prefer to use compensatory techniques like steppage gait or hip hiking.
When foot drop is caused by hemiplegia, peroneal nerve stimulation offers the potential advantages over an AFO since it may be customized for each patient and offers active gait correction. The common peroneal nerve is stimulated electrically for a brief period of time between the popliteal fossa and the fibular head. The injured limb’s heel contains a switch that controls this burst. When the foot is raised and comes into touch with the ground, the stimulator is triggered. Dorsiflexion and eversion are attained during the swing phase of gait as a result.
Electrically stimulation with walking can also help lessen foot drop symptoms. Another name for this treatment is FES, or functional electrical stimulation. Wearing small devices near the knee allows for the appropriate mobility of the muscle by responding to leg movement and providing modest electrical stimulation.
A nerve stimulator may be implanted or external and radiofrequency-activated. In research by Chae et al., electrical stimulation was helpful in about 2% of stroke patients who had spastic hemiplegia. This technique has the potential to improve gait quality and speed as well as aid in motor relearning.
In research by Kluding et al., foot drop was treated with an AFO versus a foot-drop stimulator (FDS) in 197 individuals who had suffered a stroke around three months prior. They found that although gait speed and functional outcomes improved significantly with both methods, user satisfaction was higher with the FDS; they also emphasized that early therapy can have a lasting positive impact.
FES is given to the lower limbs to address foot drop and enhance functional walking in stroke patients. Patients have profited from them by having faster gaits, stronger muscles, and other improvements.
For patients with drop foot caused by a stroke, both AFO and FES treatment significantly improved gait.
How Can Physical Therapy Help?
Foot drop, also known as drop foot, is a condition that makes it difficult for you to elevate your toes and the top of your foot up toward the shin. This movement is termed dorsiflexion which is crucial for balance and appropriate gait.
In order to move the muscles, the brain must communicate with your muscles to inform them when to contract and relax. Foot drop can occur when a brain injury or stroke impairs the parts of the brain that produce these signals. Foot drop, however, can also be brought on by injury to the nerve roots coming from the lumbar spine (more precisely, L4-L5) or to the muscles or nerves in the lower leg that directly conduct dorsiflexion.
Exercises for foot drop assist in rewiring the brain and strengthening the local muscles to enhance your capacity to transmit your brain the proper signals for moving your foot. Neuroplasticity, a rewiring process, is essential for recovering from foot drops.
The brain receives the stimulation it needs to recover the skill of dorsiflexion through regular practice of therapeutic exercises and movement retraining.
Most physical therapists give their patients a sheet of foot drop exercises to do on their own at home in order to give the brain the repetition it requires.
Now that you are aware of the significance of foot drop exercises, heal, let’s start exercise.
1. Ankle Plantar Flexion
- Put both of your legs out in front of you while lying on the ground.
- Take a resistance band, and encircle your foot’s sole with it.
- In your hands, hold the two ends.
- Point your toes slowly before going back to where you were.
- Do ten times in total
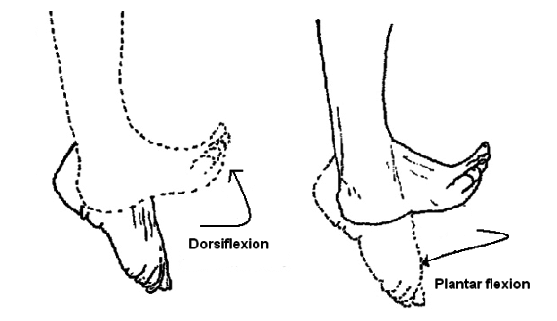
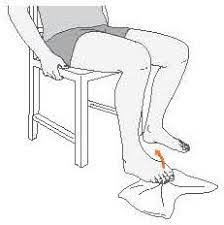
2. Ankle Dorsiflexion
Ankle dorsiflexion is an important motion that enables the foot to rise toward the shin. It is essential for appropriate walking because it aids in clearing the foot during the swing portion of the gait cycle.
- Perform this passive foot drop exercise. with the injured leg still crossed over the other leg,
- Next, dorsiflex your foot using the arm that is unaffected.
- This exercise is a great place to start since it mimics the movement that persons with foot drop struggle with.
- You can also wrap a towel or belt over your foot to do the exercise if you have trouble getting into this posture or getting your hand to your foot.
Anyone who is having trouble moving only very slightly should start with this passive movement. Additionally, it will lessen the likelihood that your foot and ankle muscles may stiffen up from immobility.
Ankle dorsiflexion is frequently impaired in those with foot drop, making it difficult to lift the foot and toes off the ground while walking.
Here are several different approaches:
a. Towel scrunch:
- Place your feet level with the floor while sitting in a chair.
- A little towel should be placed on the floor in front of your feet.
- Only your toes should be used to scrunch the towel in your direction.
- Once you’ve pulled the towel as far as you can, hold the contraction for a few seconds.
- Release and then repeat 10-15 times
- Do two or three sets of towel crunches.
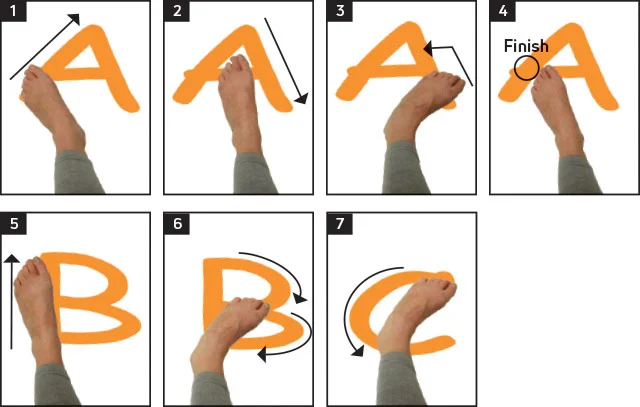
b. Ankle Alphabet
- Either sit in a chair or lay on your back.
- Keep your knee straight while you extend one leg in front of you.
- By imaging big toe as a pen, start writing the alphabet in the air.
- Each letter of the alphabet can be drawn by moving your ankle and foot.
- The exercise should be done carefully and gently.
- Put the other foot down and repeat.
- For each foot, try to finish the entire alphabet.
c. Heel-toe strides
- Find an area that is open and safe to take a few steps.
- Start walking on the heel while lifting your toe off the ground.
- Step carefully and slowly, paying attention to maintaining your balance.
- After taking a few steps, begin walking on your toes with your heels up.
- For several rounds, alternate between heel and toe walks.
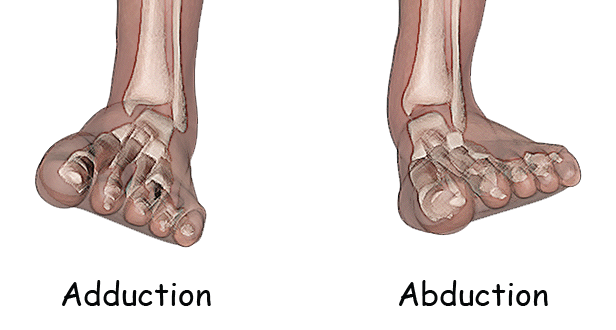
3. Ankle Adduction or Abduction
Cross the injured leg over the other leg for a great passive foot drop exercise. The front portion of the foot should then be moved from side to side using the unaffected hand. Keep your attention on starting every motion with your ankle.
Patients with extremely restricted movement benefit greatly from passive exercises for foot drop. If you are already moving, then you can increase the difficulty by performing the exercise without using your hands (this is known as “active exercise”).
4. Assisted Toe Raises
The maneuver that requires the most skill when doing foot drop is toe raising. It’s acceptable if you find this movement challenging. Thankfully, you may use this passive activity to encourage neuroplasticity and reorganize the brain.
- First, put your affected foot on top of your non-affected foot.
- Next, raise your foot using your unaffected foot.
- To assist the brain become more active, make slow, deliberate motions.
- You can do this passively by keeping your foot entirely relaxed, or actively by actively trying to dorsiflex with the assistance of your other foot.
- Lift your foot up and down ten or more times while performing this exercise.

5. Toe Raise “Negatives”
In a “negative” exercise, the eccentric portion of a movement is emphasized. With the prior toe raise exercise, the eccentric component of is lowering the foot back down.
We will solely focus on the eccentric portion of the action during this exercise.
As same the toe raise exercise, begin by raising your affected foot into a flexed position with the toes facing your shin. This time, though, try to lower your foot as gradually as you can rather than immediately doing so.
Because it does need some foot control, this maneuver is more difficult. Do this exercise 10 times.
6. Heel Raises
Toe raises are the reverse of this vigorous foot drop exercise. Even though it might not seem to be assisting with foot drop, this will help train the nearby muscles.
- To begin, place your feet flat on the floor and perform heel lifts.
- Then, raise your heels off the ground while pointing your toes.
- By forcefully pressing through your first and second toes, try to maintain appropriate neutral foot alignment while making sure your ankles don’t move outward during the heel lifts.
- The muscles in your calf and lower back of your leg should be active.
- Do ten times total.
7. Ankle eversion
- Put your affected foot flat on the ground to begin this active foot drop exercise.
- Then, extend your toes and the outer edge of your foot before relaxing back down.
- Avoid compensating with your leg by placing your attention on separating the movement from your foot and ankle.
- Do ten times in total.
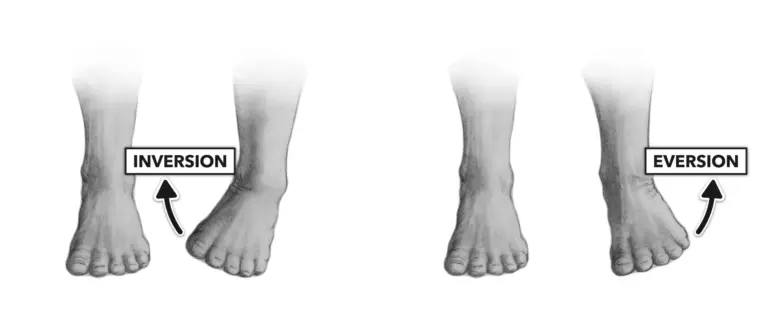
8. Ankle Inversion
- For ankle inversion, start with the same posture, then lift your toes and the inside border of your foot toward your body’s midline before relaxing back down.
- Do Ten times in total.
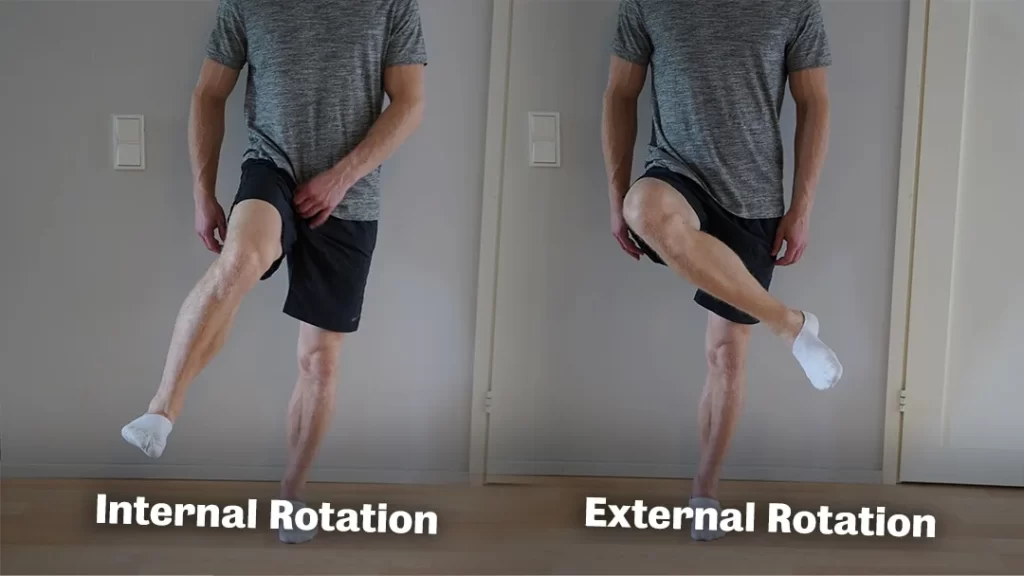
9. Hip external and internal rotation:
This exercise helps with foot drop because increased tone (stiffness) in the leg can also affect the foot, even though it mostly works the upper leg and hip.
- Starting exercise in a seated position, to perform this lower-limb workout.
- Next, externally rotate your hips while kicking your affected leg inward toward your midline. After that, kick your injured leg outward (hip internal rotation) as though you were kicking a ball to the side. Repetition is necessary.
This exercise reduces foot drop because it increases leg mobility, which trickles down to the feet.
10. Hip Rotation Slides
These exercises are designed to strengthen the hip muscles and increase hip mobility, which can help to compensate for the absence of foot dorsiflexion. To conduct hip rotation slides for foot drop, follow these instructions:
- Start by placing your feet level on the ground while sitting on the edges of a chair or other solid surface.
- Maintain your posture upright during the workout, by keeping your back straight and contracting your abdominal muscles.
- Begin with one leg at a time. Lift the injured leg off the ground just a little bit while keeping the foot relaxed.
- Slowly rotate your hip inward, as if you were trying to bring your knee towards the opposing leg. Movement should be gentle and controlled.
- After a few seconds of holding the inward rotation, progressively twist your hip outward, pulling your knee away from the leg on the other.
- About 10 to 15 times, alternate the hip’s inside and outward rotation.
- Perform the same exercise on the opposite leg also.
On each leg, carry out two to three sets of hip rotation slides. As you get skilled at the exercise, progressively increase the amount of repetitions.
Advice:
- As you get stronger and more flexible, start with simple movements and progressively increase the range of motion.
- Avoid any motions that hurt or make you uncomfortable. The activity should be difficult but not painful.
- Concentrate on contracting the hip muscles, instead of depending simply on momentum during the rotation,
- By gently guiding the knee inward and outward, you may help in the action with your hands.
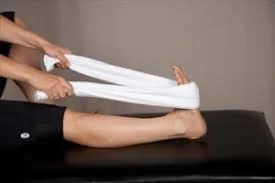
11. Towel Stretch
- Put both of your legs out in front of you while lying on the ground.
- Wrap a towel or exercise band around the affected foot and hold onto the ends with the hands.
- Draw the band or towel closer to your body.
- Hold for a minute. then take a 30-second break.
- Do 3 Repetition.
12. Heel to toe rocks
- Stand in front of a wall, table, chair, or other substantial object that you may lean against for support.
- As you lean forward, stand up on your toes.
- For five seconds, maintain this posture.
- Next, lean back on your heels while lifting your toes off the ground.
- Take a 5-second hold.
- Do it 6 times.

13. Marble Pickup
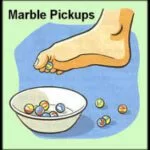
- Put your feet flat on the ground while sitting in a chair.
- Put a bowl in front of you on the floor, along with 20 marbles.
- Pick up each marble with the toes of the affected foot and put it in the bowl.
- Continue until all of the marbles have been collected.
14. Ball lift
- Place your feet flat on the floor while sitting on a chair.
- Place a little, tennis-ball-sized object on the ground in front of you.
- You can slowly lift the item while holding it between your feet by spreading your legs.
- Hold for five seconds, then release progressively. Do 10 times a day.
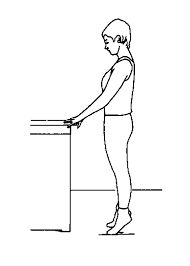
15. Single-Legged Stance
Another excellent exercise for foot drop is standing on one foot because it requires ankle eversion and tests your overall ankle stability. Patients with foot drop who are strong and stable enough can attempt to stand for 15 seconds on their affected leg at a time.
Patients with foot drop can practice single-leg stance to improve several critical areas:
- Balance and Stability: The exercise tests the patient’s ability to balance on one leg, which aids in building stability-related muscles. Falling can be avoided and confidence is increased when performing daily tasks with improved balance.
2. Strengthening the affected Leg: To maintain balance when standing on one leg, the muscles in the affected leg and ankle are used. These muscles, which may have deteriorated as a result of foot drop, can be strengthened with regular practice.

Here is a single-leg stance practice to do:
- For support, hold a firm chair or countertop.
- Keep the chair or tabletop within reach while facing it.
- With the knee bent to a comfortable position, raise one foot off the ground.
- Depending on the patient’s comfort and capacity, the non-standing leg may be kept straight, slightly raised, or bowed.
- Maintaining balance while keeping your core muscles active is your primary focus.
- Do not tilt or lean to one side.
- Beginning with a short period of balance, progressively extend it as your strength increases.
- If necessary, you can lightly touch the chair or countertop for support, but as you develop stability, attempt to gradually reduce your reliance on it.
FAQs
What is the first sign of a foot drop?
Being unable to lift the front of your foot is the primary indicator of foot drop.
What actually causes foot drop?
Foot drop occurs when the muscles that lift your foot are weak or paralyzed, making it impossible for you to raise the front portion of your foot. Damage to the peroneal nerve frequently causes this symptom.
Can exercise be used to correct foot drop?
Exercise can help you build up your leg muscles and keep your knee and ankle joints mobile. Gait difficulties brought on by foot drop could be helped by these exercises. Exercises that stretch the muscles are essential to avoiding calf and heel tightness.
Is physical therapy available for foot drop?
Yes, physical treatment for foot drop has a lot of advantages.
Physical therapy can assist in preserving the range of motion in your ankle and knee joints as well as the strength of your calf muscles. In order to help individuals with abnormal gaits walk more effectively and increase stability, a physical therapist can also offer gait training.
How long does it take for foot drops to recover?
Depending on the precise cause and the degree of damage to the related nerves, the time it takes to heal from drop foot can vary. Recovery from nerve damage may only take three months, whereas MS-related neuron loss may require up to twelve months.