
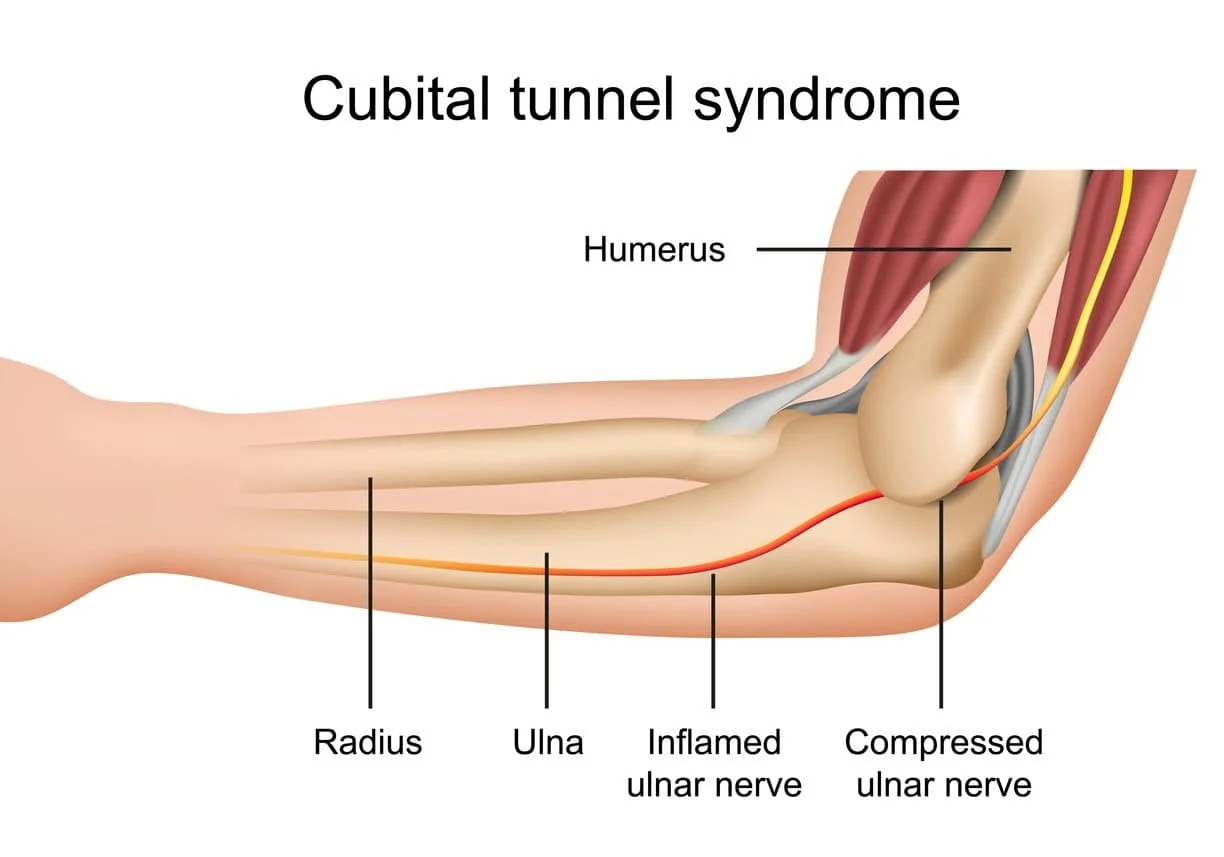
Cubital Tunnel Syndrome
Cubital Tunnel Syndrome is a condition that involves pressure or stretching of the ulnar nerve (also known as the “funny bone” nerve), which can cause numbness or tingling in the ring and small fingers, pain in the forearm, and/or weakness in the hand. When Ulnar nerve passes through “funny bone” in the elbow creates sometimes extra pressure in the nerve nad creates related symptoms.
The most common place for compression of the nerve is behind the inside part of the elbow. Ulnar nerve compression at the elbow is called “cubital tunnel syndrome.” It is the second most common peripheral nerve compression syndrome in the human body.
Diagnosis is mostly done by symptoms and signs and sometimes require nerve conduction studies also called NCV Test. In most cases, Cubital tunnel syndrome can be managed with conservative treatments and Physiotherapy Exercise. But in more severe cases may require surgery to reduce pressure on the affected nerve.
Table of Contents
Which are the common Causes of Cubital Tunnel Syndrome ?
There are a few causes of this ulnar nerve compression. These may include:
- Pressure: The nerve has little padding over it. Direct pressure (like leaning the arm on an arm rest) can press the nerve, causing the arm and hand — especially the ring and small fingers — to “fall asleep.”
- Stretching: Keeping the elbow bent for a long time can stretch the nerve behind the elbow. This can happen during sleep.
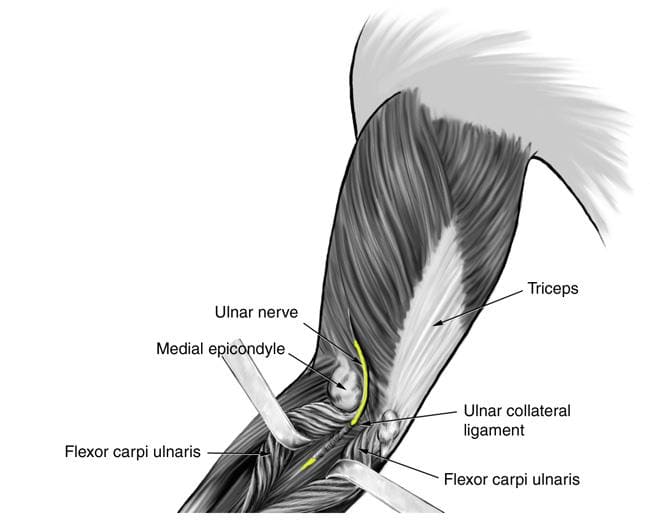
- Anatomy: Sometimes, the ulnar nerve does not stay in its place and snaps back and forth over a bony bump as the elbow is moved. Repeated snapping can irritate the nerve. Sometimes, the soft tissues over the nerve become thicker or there is an “extra” muscle over the nerve that can keep it from working correctly.
- Arthritis, bone spurs, and previous fractures or dislocations of the elbow can also cause cubital tunnel syndrome.
- Noncancerous fatty tumors (lipomas)
- Bone tumors
- Severe Inflammation of surrounding tissue
- In many cases, the cause is not known (Idiopathic).
- In some people, the nerve slides out from behind the medial epicondyle when the elbow is bent. Over time, this sliding back and forth may irritate the nerve.
- Leaning on your elbow for long periods of time can put pressure on the nerve.
- Fluid buildup in the elbow can cause swelling that may compress the nerve.
- A direct blow to the inside of the elbow can cause pain, electric shock sensation, and numbness in the little and ring fingers. This is commonly called “hitting your funny bone.”
What are the symptoms of cubital tunnel syndrome?
The following are the few most common symptoms are as per below :
- numbness, pain, and weakness in the arm, forearm, and fingers.
- weakened or reduced grip.
- waking at night from pain or numbness in the hands or fingers, especially the pinky and ring fingers.
- difficulty bending and straightening the fingers.
- difficulty manipulating things with the hands or fingers.
- muscle loss at the base of the small fingers.
- Weak grip and clumsiness due to muscle weakness in the affected arm and hand.
- Aching pain on the inside of the elbow.
Medical History and Physical Examination :
Your doctor will discuss your medical history and general health. He or she may also ask about your work, your activities, and what medications you are taking.
- The presenting complaint is typically one of “pins and needles” in the forearm and the hand.
- Tap over the nerve at the funny bone. If the nerve is irritated, this can cause a shock into the little finger and ring finger (Tinel’s sign) — although this can happen when the nerve is normal as well.
- Check whether the ulnar nerve slides out of normal position when you bend your elbow.
- Move your neck, shoulder, elbow, and wrist to see if different positions cause symptoms.
- Check for feeling and strength in your hand and fingers.
- A reduced or complete loss of sensation on the palmar and dorsal sides of the little finger and the medial part of the ring finger in advanced cases.
- Stress tests like sustained elbow flexion for one minute or compression of the ulnar nerve at the cubital tunnel region may also be positive, causing paresthesia along with the distribution of the ulnar nerve, but the diagnostic value of these tests are poor.
- Motor functions are less common and usually shows in severe cases where Patients may complain of weakness in the hand and frequent dropping of objects.(mild weakness of the interosseous muscles to severe atrophy of the hand intrinsics and weakness of the handgrip.)
- Froment’s sign can be positive, showing weakness of adductor pollicis, which is supplied by the ulnar nerve.
Differential Diagnosis :
- Lesions in the Guyon (ulnar) canal.
- Cervical spondylosis.
- Brachial plexus injuries.
- Thoracic outlet syndrome.
- Syringomyelia.
- Pancoast tumors.
- Motor neuron disease.
- Carpal tunnel syndrome.
- Polyneuropathy.
DIAGNOSIS:
- Tests
- X-rays. These imaging tests provide detailed pictures of dense structures, like bone. Most causes of compression of the ulnar nerve cannot be seen on an x-ray. However, your doctor may take x-rays of your elbow or wrist to look for bone spurs, arthritis, or other places that the bone may be compressing the nerve.
- NCV Test : Nerve conduction studies. These tests can determine how well the nerve is working and help identify where it is being compressed. Nerves are like “electrical cables” that travel through your body carrying messages between your brain and muscles. When a nerve is not working well, it takes longer for it to conduct. During a nerve conduction test, the nerve is stimulated in one place and the time it takes for there to be a response is measured. Several places along the nerve will be tested and the area where the response takes too long is likely to be the place where the nerve is compressed.
- Nerve conduction studies can also determine whether the compression is also causing muscle damage. During the test, small needles are put into some of the muscles that the ulnar nerve controls. Muscle damage is a sign of more severe nerve compression.
Prognosis (Outcome):
- Mostly half the patients achieve an improvement in their symptoms with conservative management and Physiotherapy Treatment.
TREATMENT:
Nonsurgical Treatment:
1) Medical treatment:
- NSAIDs : Nonsteroidal anti-inflammatory medicines. If your symptoms have just started, your doctor may recommend an anti-inflammatory medicine, such as ibuprofen, to help reduce swelling around the nerve.
- Although steroids, such as cortisone, are very effective anti-inflammatory medicines, steroid injections are generally not used because there is a risk of damage to the nerve
- Bracing or splinting.Your doctor may prescribe a padded brace or splint to wear at night to keep your elbow in a straight position.
- Physiotherapy Treatment : Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
2)Physiotherapy treatment:
Exercise 1:
- Extend the arm straight out in front of the body with a straightened elbow, as much as is comfortable, with the palm facing up.
- Slowly and gently curl the fingers towards the palms then slowly and gently bend them down, away from the body.
- Slowly and gently bend the elbow, as much as is comfortable, and then slowly release back.
Exercise 2:
- Extend the arm straight out in front of the body with a straightened elbow, as much as is comfortable, with the palm facing up.
- Slowly and gently begin to bend the elbow towards the body while at the same time gently twisting the wrist backward, away from the body.
- If steps 1 and 2 are comfortable, then keeping the wrist bent back, slowly and gently bend the elbow, as much as is comfortable, then slowly release it.
Exercise 3:
- Stand, sit, or lie down and extend the arm out straight alongside the body with a slightly clenched fist.
- Slowly and gently bend the elbow, bringing the fist towards the body, as far as comfortable, and then slowly release.
Exercise 4:
- Stand with the elbow bent so that the forearm runs parallel to the body.
- Slowly and gently twist the palms upwards to face the ceiling and then downwards to face the floor.
- Range-of-motion exercises. Your physiotherapist will show you specific exercises to help return full length to the muscles of the arm that have shortened due to protective posturing, and to maintain the normal length of those that have remained unaffected.
- Muscle strengthening exercises. Improving strength in the surrounding muscles can help reduce pain and improve functional ability.
- Nerve gliding exercises. Nerves have the ability to be stretched, just like muscles or joints. Nerve tissue is the strongest, longest tissue in the body and the one most sensitive to stretching. In cubital tunnel syndrome, the nerve can become tight or trapped; these exercises are an effective means of promoting blood flow to the ulnar nerve and gently stretching it.
Ergonomic training:
- Your physiotherapist will teach you ways to avoid positions and postures that compress or put a prolonged stretch on the ulnar nerve. You may need to learn how to modify work and self-care activities to prevent further nerve irritation.
- Bracing or splinting. Your doctor may prescribe a padded brace or splint to wear at night to keep your elbow in a straight position.
- Nerve gliding exercises. -Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
If Nonsurgical methods have not improved your condition :
Surgical Treatment:
Your doctor may recommend surgery to take pressure off of the nerve if:
- Nonsurgical methods have not improved your condition
- The ulnar nerve is very compressed
- Nerve compression has caused muscle weakness or damage
- There are a few surgical procedures that will relieve pressure on the ulnar nerve at the elbow. Your orthopaedic surgeon will talk with you about the option that would be best for you.
- These procedures are most often done on an outpatient basis, but some patients do best with an overnight stay at the hospital.
Cubital tunnel release:
- In this operation, the ligament “roof” of the cubital tunnel is cut and divided. This increases the size of the tunnel and reduced the pressure on the nerve.
- After the procedure, the ligament begins to heal and new tissue grows across the division. The new growth heals the ligament, and allows more space for the ulnar nerve to slide through.
- Cubital tunnel release tends to work best when the nerve compression is mild or moderate and the nerve does not slide out from behind the bony ridge of the medial epicondyle when the elbow is bent.
Ulnar nerve anterior transposition.
- In many cases, the nerve is moved from its place behind the medial epicondyle to a new place in front of it. Moving the nerve to the front of the medial epicondyle prevents it from getting caught on the bony ridge and stretching when you bend your elbow. This procedure is called an anterior transposition of the ulnar nerve.
- The nerve can be moved to lie under the skin and fat but on top of the muscle (subcutaneous transposition), or within the muscle (interamuscular transposition), or under the muscle (sub-muscular transposition).
Medial epicondylectomy:
- Another option to release the nerve is to remove part of the medial epicondyle. Like ulnar nerve transposition, this technique also prevents the nerve from getting caught on the boney ridge and stretching when your elbow is bent.
COMPLICATION:
- Infection.
- Nerve damage.
- Elbow instability.
- Elbow flexion contracture.
- Pain at the site of scar.
- Blood vessel or nerve damage
- Loss of sensation or fine motor coordination
PREVENTIVE MEASURES :
- Keep your arms flexible and strong.
- Don’t rest only
- our elbows, especially on a hard surface.
- Warm up before exercising or using your arms for sports or other repetitive movements.
Initially, the easiest way to get relief from Cubital tunnel syndrome is to avoid actions that irritate the symptoms, such AS:
- sleeping with the elbow bent
- holding a phone for a long time
- typing for extended periods
- holding a book or tablet up for a long time
- sitting with the arms on an armrest for a long while
- leaning on the elbow
- driving for a long time
- driving with the arm resting on an open window
Additional home treatment to try can include the following:
- Rest the arm and elbow when possible.
- Apply ice compresses wrapped in a cloth or towel to the area for 10 to 15 minutes several times daily.
- Loosely wrap the impacted forearm with padding, such as a cloth, towel, or pillow, or wear an elbow split at night to prevent the elbow from bending.
- anti-inflammatory medications, such as aspirin and other non-steroidal anti-inflammatory drugs or NSAIDs.
- Adjust computer or writing workspaces so that the chair is not lower than the tabletop.
- Wear an elbow pad during the day to give protection.
- Avoid clothing or sports equipment that compresses or restricts the elbow.






8 Comments