
Clavicle Fracture
Table of Contents
Introduction
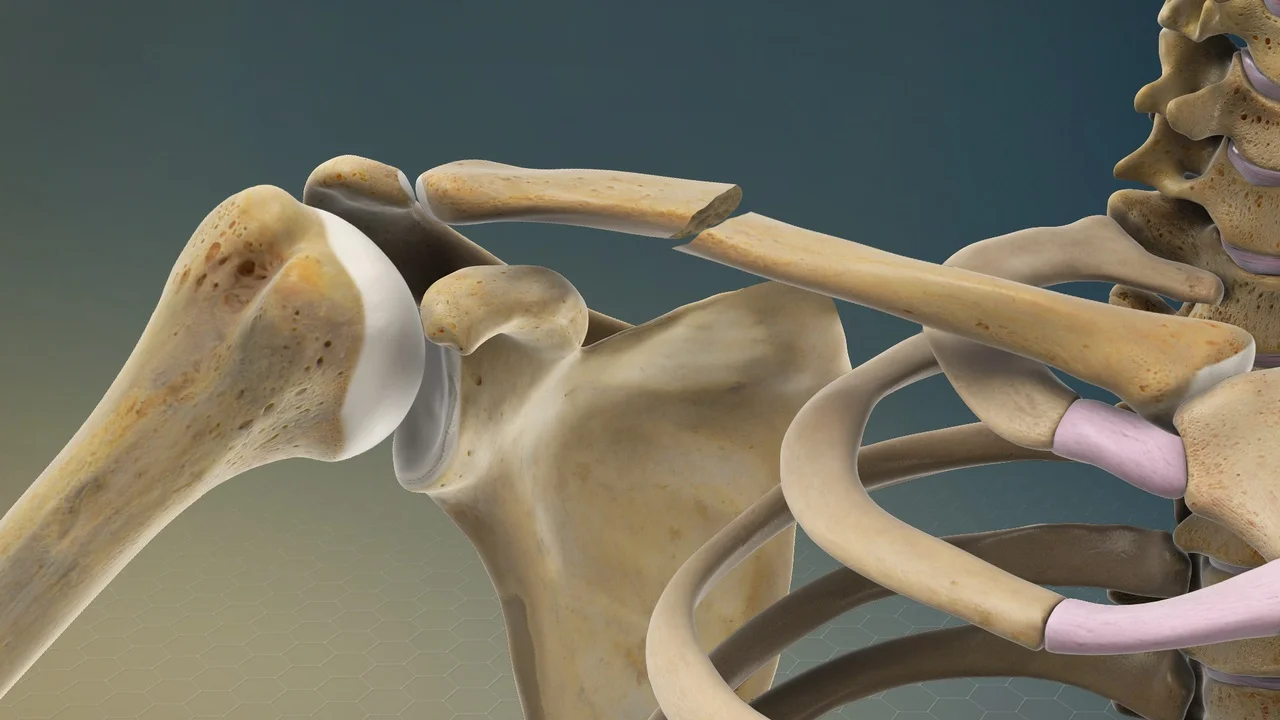
A clavicle fracture, also known as a broken collarbone, is a common type of fracture that involves a break in the clavicle bone. The clavicle is the bone that connects the shoulder blade (scapula) to the breastbone (sternum). Clavicle fractures often occur as a result of a fall onto the shoulder or an outstretched arm, direct trauma to the collarbone area, or during sports activities.
Clavicle fractures are very familiar injuries in adults (two-five percent) and children (ten to fifteen percent) and describe forty-four to sixty percent of all shoulder fractures. It is the most common fracture in happens in the children group. A fall onto the lateral shoulder most continually causes a clavicle fracture.
Radiographs verify the diagnosis and aid in further assessment and treatment. The vast majority of displaced or comminuted fractures might need operative fixation, although many other types of clavicle fractures can be managed conservatively.
Related Anatomy:
The clavicle is found subcutaneously between the sternum and the scapula, joining the arm to the body. Comparable to all the long bones that exist in the human body, the clavicle has medial and lateral both epiphysis but it does not have a well-defined medullary cavity.
The growth plates of the medial and lateral clavicular epiphyses don’t merge until the years of twenty-five age. Anomalous among long bones is the clavicle’s S-shaped double curve, which is convex medial aspect and concaves on the lateral aspect. This contouring helps the clavicle function as a support for the upper limb, while also saving and allowing the course of the axillary vessels and brachial plexus.
Cause of Clavicle Fracture
Younger people frequently sustain these injuries by the method of medium to high-energy mechanisms, for example, road traffic accidents or sports wounds, whereas geriatric people are more potential to sustain injuries due to the sequela of a low-impact fall.
A fall onto an extended hand is the commonest cause of clavicle fracture it has been found that the clavicle most continually fails in direct reduction from a force applied directly to the shoulder. In roughly more than eighty-five documented cases, a clavicle fracture was caused by a fall directly onto the lateral shoulder.
A clavicle fracture when force or stress results in it snapping. Typical causes are:
- Collisions (injury) when an arm is extended, for example during skiing, hockey, football, and other impact sports.
- Direct trauma to the clavicle, for example, in road traffic accidents.
- Falls onto the clavicle or an outstretched hand.
- Passing through the birth canal for a newborn.
Epidemiology
In an expected examination, the age- and sexes-specific incidence and features of clavicular fractures were analyzed between 1989 & 1990. The population at threat comprising of approximately 200,000 people aged fifteen or beyond in the county of Uppsala, Sweden. In 185 individuals, there were 187 clavicular fractures, with a total prevalence of 50 per 100,000 (men 71 per 100,000, women 30 per 100,000).
Males were particularly younger and sustained comminuted fractures more frequently than females. The fracture incidence declined with age in both sexes, although the decline was significant only in males. Vehicle accidents most repeatedly result in clavicular fractures in both sexes, whereas sports activities were particularly more expected in males. Right and left clavicles were near as repeatedly fractured, and a direct fall on the shoulder was the most regular cause of injury for both sexes. With roughly three out of four fractures happening through the middle section and one out of four through the acromial part of the clavicle, there was no difference in anatomical position between the sexes. 95 percent of patients suffered uncomplicated recovery, whereas 5 percent encountered non-union, which was evenly split between the acromial and middle portions of the clavicle.
Clavicle fractures describe 2 percent to 10 percent among all fractures.
- Impact one in thousand individuals per year
- Are the most common fractures during childhood
- Roughly two-thirds of all clavicle fractures happen in men.
- Include up to 10 percent of all sport-related fractures and have the third-longest return time to sport with as many as 20 percent of athletes with for example injuries failing to return to sport.
Classification of Clavicle Fracture
Fractures of the clavicle are generally defined using the Allman classification system, separating the clavicle into three groups depending on the area which was later revised by Neer(in which Group II was further classified into 3 kinds).
Group I: Fractures at the middle third or mid-shaft fractures (the most common site),
Group II: Fractures at the lower or lateral third. A typical place for un-union.
Group III: Fractures at the proximal or medial third.
Robinson’s type was more precise for various fracture kinds in the middle third, while Craig’s classification was bettered precise for fractures at the lateral third.
One of the most popular classification systems when assessing clavicular fractures is the Neer classification of clavicular fractures, along with the AO type system.
The classification system, fractures into five types communicates both the stability and treatment advice of the fracture concentrating on the relationship of the fracture to coracoclavicular ligaments and the acromioclavicular joint.
Type I
Considered a stable fracture needing non-surgical treatment
- The coracoclavicular ligaments are situated lateral to a small or non-displaced fracture line.
- trapezoid and conoid ligament intact
Type IIa
Considered an unstable fracture needing surgical treatment
- A fracture with an important medial part displacement is present medial towards the coracoclavicular ligament.
- conoid ligament unbroken
- trapezoid ligament unbroken
Type IIb
Considered an unstable fracture requiring operative treatment
- A torn conoid ligament and an intact trapezoid ligament arise from the fracture between the coracoclavicular ligaments.
- displacement of the medial clavicle
Type III
Considered a stable fracture needed non-surgical treatment
- intra-articular lower clavicular fracture spreading into the acromioclavicular joint
- conoid ligament unbroken
- trapezoid ligament unbroken
Type IV
Salter-Harris type I physeal fracture is considered a stable fracture needing nonsurgical treatment
- inner portion clavicle has displaced in the superior direction as the periosteal sleeve becomes avulsed from the inferior cortex
- conoid ligament unbroken
- trapezoid ligament unbroken
Type V
Considered an unstable stable fracture needing surgical treatment
- comminuted fracture with medial clavicle displacement
- inferior clavicle piece joined to the coracoclavicular ligament
- conoid ligament unbroken
- trapezoid ligament unbroken
History and Physical Examination
The patient can look at the following signs and symptoms:
- A patient can cradle the injured limb with the uninvolved arm.
- A patient can tell a snapping or cracking voice when the injury happens.
- The shoulder can be visibly contracted comparable to the other good side and can droop.
- Swelling, ecchymosis, and tenderness may be present around the clavicle.
- An abrasion over the clavicle may be noticed, indicating that the fracture was from a direct hit.
- Crepitus sensation that happens from the fracture ends rubbing against each other may be reported with gentle manipulation.
- A problem with breathing or decreased breath sounds on the involved side may indicate a pulmonary injury, for example, a pneumothorax.
- Palpation of the scapula and ribs can demonstrate a concurrent trauma.
- Severe dehydration and blanching of the skin at the fracture site can indicate an approaching open fracture, which most frequently requires operation stabilization.
- Nonuse of the arm on the involved side is a neonatal presentation.
- Correlated distal nerve dysfunction demonstrates a brachial plexus injury.
- Diminished pulses can mean a subclavian artery injury.
Diagnostic Procedures and Differential Diagnosis
A diagnosis can usually be completed by a patient’s H/O and physical assessment.
The differential diagnosis of a clavicle fracture possesses acromioclavicular joint injury, rib fracture, scapular fracture, shoulder dislocation, rotator cuff injury, and sternoclavicular joint injury.
Laboratory studies are contained in clavicle fractures according to the severity of trauma. With a presumed vascular injury, receive a full blood count (CBC) to check the hemoglobin and hematocrit values. If a pulmonary injury is presumed or determined, perform an arterial blood gas (ABG) test and get an expiration posteroanterior (PA) chest film. Additional imaging examinations that can be utilized in the assessment of a clavicle fracture have given below:
- Radiography of the clavicle and shoulder
- Computed tomography (CT) checking with 3-dimensional (3-D) reconstruction
- Arteriography
- Ultrasonography
Treatment of Clavicle Fracture
A clavicle fracture treatment is either operative or conservatively depending upon different aspects including the location (mid-shaft, distal, proximal), nature (displaced, undisplaced, comminuted) of the fracture, open versus closed injury, age, and neurovascular issues.
Clavicle fractures are often treated conservatively with immobilization with a splint followed by physiotherapy. For nondisplaced fractures, this still yields satisfactory results, but for displaced mid-shaft clavicle fractures, conservative treatment leads to a higher probability of re-injury, a hurried return to sport, and poor shoulder function. secondary to clavicular mal-union and contracture, with consequent thoracoscapular dyskinesia. Furthermore, conservative treatment of displaced lateral fractures in the athletic patient has been shown to result in increased rates of non-union and subsequent impairment of shoulder function.
So for the athletic person, the operative approach is frequently performed for displaced lateral fractures and is recommended for mid-shaft fractures that are totally displaced, shortened to greater than two centimeters, or comminuted.
It’s essential to follow your healthcare provider’s recommendations for treatment, rehabilitation exercises, and follow-up appointments to ensure proper healing and minimize complications.
Surgical Treatment
Surgery may be considered for more severe clavicle fractures, especially if the bone fragments are significantly displaced or if there is an open fracture (bone piercing through the skin). Surgical treatment often involves realigning the bone fragments and using plates, screws, or other fixation devices to hold them in place during the healing process.
Surgical treatment of clavicular fractures is indicated for;
- Excessive displacement caused by comminution causes the skin limb to angle and tent enough compromising its integrity and that does not respond to closed reduction.
- Symptomatic nonunion-like shoulder girdle impairment neurovascular complication.
- Neurovascular complication or compromise that is created or that fails to reverse later to the closed reduction of the fracture.
- Open fracture.
- Type II distal clavicular fracture (displaced).
- Multiple injuries, when the mobility of the patients is desirable and closed approaches of immobilization are impracticable or not indicated.
- Floating shoulder.
- Difficulty bearing closed immobilization for example neurological difficulties of Parkinsonism, and seizure conditions.
- Cosmetic reasons.
- Comparative indications have shortening of > fifteen to twenty mm and displacement > the width of the clavicle.
The operative method includes:
- Internal fixation with plates and screws. ( most typical)
- Intramedullary (IM) fixation.
For intramedullary nails, periodic metalwork removal was necessary; yet, plate fixation in midshaft displaced fractures was not recommended. On the other hand, frequent discarding of metalwork was successful for cerclage wire, tension band wire, “hook” plate, and screw fixation but not for “un-ACJ-spanning” plate and suture fixation in displaced lateral clavicle fracture. These stabilization approaches are essential for lateral clavicle fractures because they work on the acromioclavicular joint along with additional ligaments that could be damaged during fracture.
Recovery time for a clavicle fracture can vary depending on the individual and the severity of the fracture. Generally, it takes around 6 to 12 weeks for the bone to heal, but it may take longer for a complete recovery and return to normal activities, especially for athletes or individuals with physically demanding jobs.
Physical Therapy or Rehabilitation
The main objective of rehabilitation is to enhance and restore the role of the shoulder for ADLs activity, and vocational, and sports conditioning. Rehabilitation programs may vary a minor in the 1st some weeks depending upon the preliminary treatment method which is conservative vs operation.
Rehabilitation for Conservative Management
Fracture recovery can bring more time in nonoperative therapy. Conservatively treated fractures of the clavicular midshaft commonly connect between eighteen and twenty-eight weeks afterward to the damage. So routine follow-up needs to be done to check whether the fracture place is correctly unioned or not. So rehabilitation protocol can also vary depending on particular co-morbidities.
The POLICE protocol which is also detailed below in the context of clavicle fracture, can be utilized for recent undisplaced clavicle fractures in the initial stages (two to four weeks).
Protection:
Up until the clinical union is finished, the patient’s shoulder is immobilized in a splint or figure-of-eight brace. In order to prevent or minimize secondary fracture shortening while the fracture is healing, a figure-of-eight brace is typically utilized. But it is related to more discomfort and pain possessing compression of the nerve with temporary brachial plexus palsies and restriction of venous blood return.
And numerous studies came to the conclusion that there are no distinctions between these two methods for treating clavicle fractures in terms of time to healing or the frequency of nonunion. So a splint is usually used and immobilization in the internal rotation is usually suggested for two-four weeks. Wear the splint as much as possible time, except for exercises and personal hygiene. Patients choose to wear them at night or not but they need to be cautious.
During violent coughing, sneezing also patients require to take warning (as respiratory excursions may result in clavicle movement) by preventing it as much as possible and also understanding active-assisted coughing techniques if required.
Optimal loading
It is necessary to understand the phase of bone recovery in demand to proceed with optimal loading.
Bone recovery during the same day of injury to the first week:
- Stability at the place of fracture: None
- The phase of Bone recovery: Inflammatory phase and there is no callus noticed on the X-ray.
Bone recovery during the 2nd week :
- Stability at the fracture area: minimal amount
- Stage of bone recovery: earlier reparative phase and some amount of callus formation are noticed in the X-ray.
Therapy or Guidance for one-two weeks Post injury:
- Use of arm splints noted above ( require to use most of the time).
- Self-mobilization of the elbow and wrist out of the sling is needed several times a day to prevent stiffening of the elbow and wrist.
- Do not raise your elbow beyond shoulder height as this can be hurting.
- The range of movement of the shoulder must commonly be determined to pendulum activities for the first one-two week.
- Correct postural habits and neck range of movement are introduced.
Bone recovery from three to six weeks post-trauma:
- Stability: Callus formation is created and the fracture site becomes stable.
- Stage of bone recovery: Reparative stage and fracture line seem less pronounced in the X-ray.
Therapy or Advice for three to six weeks post-trauma:
- Reduce the use of an arm splint (use during non-dependent position).
- Initiate normal light simple ADLs activity with the arm and shoulder.
- Shoulder active-assisted to active range of motion in a single plane with no more > than ninety degrees is recommended within the 1st six weeks.
- Scapular mobilization exercises are performed.
- Isometric exercises of the Shoulder with tolerable resistance are started within 4-6 weeks.
- Prevent heavy lifting for the complete six weeks.
- Gradual advancement of cardiovascular changelessness exercise can be begun using fast walking and static bicycle.
Recovery of the bone from six to eight weeks post-trauma:
Fracture becomes stable by this time
The phase of fracture recovery is a reparative phase and the bridging callus is noticed clearly.
After eight weeks the remodeling phase begins and the fracture line is less distinct.
Therapy or Guidance for six-twelve weeks Post-injury:
- Free active and active assisted range of movement of the shoulder in all planes is commonly permitted after six weeks with passive range of movement as tolerable.
- Advanced resistive exercises (isotonic) for scapular stabilizers, biceps, triceps, and rotator cuff are prescribed after six weeks.
- Weight-bearing must be prevented until clinical fracture.
- Sporting activities and work, demanding weight-bearing and the help of the arm, are commonly stopped until the patient is free of pain with radiographic signs of progressing fracture consolidation, usually after six to twelve weeks.
Therapy or Guidance for six-twelve weeks and beyond:
- Begin a more aggressive strengthening protocol, cardiovascular changelessness training as bearable, and advanced sports-specific training is introduced.
- Return to specific sports is determined by the physiotherapist through functional testing specific to the patient’s demands according to which progressive sport-specific training is planned.
- Advanced activities comprising muscle endurance exercises(upper body ergometer) and cardiovascular changelessness training (treadmill, cycling) can be defined.
- Contact sports should be prevented for three to four months. Recovery for full-contact sports requires the athlete must show radiographic proof of bony healing, no tenderness when touched, a full range of movement, and adequate shoulder power.
- Rehabilitation After Postoperative Treatment
Rehabilitation After Postoperative Treatment
- The primary choice is open reduction internal fixation with a plate or locking reduction plate & screws of mid-third clavicle fractures to supply a more hard fixation and enable immediate after-operative mobilization. operative treatment permits the bone to recover faster than that conservative choice. So the time of immobilization is more transient corresponding to conservative treatment and mobilization and strengthening exercises can be defined earlier than that of conservative management. A similar progression of exercise can be defined as conservative treatment but progression can be made before.
Return to Sports
Several individuals with a recent clavicle fracture will resume sports activity, with approximately four-fifths of all patients able to resume their pre-trauma level of athletic activity, according to the Systematic assessment conducted by Robertson and Wood in 2016.
The studies have reported that return to sports is between 6 to 12 weeks postoperatively and 3-4 months for those who are managed conservatively.
Displaced mid-shaft fractures contain conservatively established lowered return rates and increased return periods to sports than those treated operatively. Displaced mid-shaft fractures treated with conservative management can result in refracture (around half of the cases) and delayed operative intervention ( over a quarter of the cases). About the chosen operative technique for mid-shaft fractures, both plate fixation and IM nail demonstrated near-complete return rates and similar return times. Surgical rehabilitation for displaced lateral clavicle fractures is standardized and has been shown to boost return rates and shorten healing times. Due to the protection of ACJ function, non-ACJ-spanning plate fixation and open suture fixation seem to give greater athletic results than other fixations. The value of a mid-shaft fracture is more significant than that of a lateral clavicle fracture due to lateral clavicle fractures are more complicated.
FAQ
Several clavicle fractures can be treated by wearing a splint to keep the arm in an immobilization position and prevent moving while the bone heals. With few clavicle fractures, regardless, the fragments of bone move far out of place when the damage happens. For these more complicated fractures, operations can be required to realign the collarbone.
use extra pillows at night to maintain yourself more upright if you find resting uneasy. apply ice packs and analgesics if pain and swelling persist while your arm is in a sling. As soon as it’s comfortable, regularly move your elbow, hand, and fingers.
Clavicle fracture repair or open reduction and internal fixation (ORIF) puts the bones back in their initial position and permits them to recover in a normal alignment. A surgical procedure understood as open reduction and internal fixation is a proven successful approach to treating fractures of the clavicle.
Several broken collarbones recover without a problem. Difficulties, when they happen, might include Nerve or blood vessel injury. Rarely, the jagged ends of a cracked collarbone can damage nearby nerves and blood vessels.
Several clavicle fractures are able to be successfully treated non-operatively with a sling and rehabilitation; yet, some displaced and more complex clavicle fractures are usually treated with surgery.
The operation commonly takes between 45-90 minutes. Usually, this process is done as a daycare operation, where you go home the same day as the operation. What to anticipate during the recovery of a Clavicle Fracture: While the bone recovers commonly within two to three months, healing takes much extended.
Lie on your back, maintaining a wand with both hands. Your palms should face down as you keep the wand.
Keep your elbows extended, and slowly raise your arms over your head until you feel a stretch in your shoulders, upper back, and chest.
Maintain for 15 to 30 seconds.
Repeat two to four times.



3 Comments