Cervical Spine Fractures
Table of Contents
Introduction
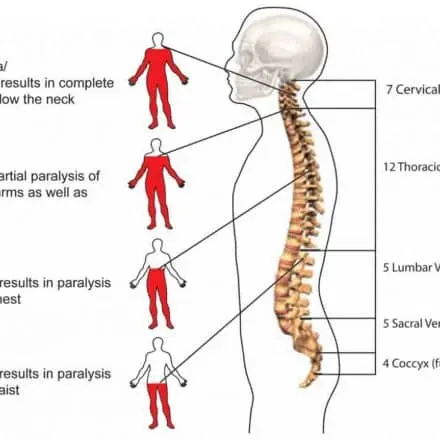
A cervical spine fracture, also known as a broken neck, is a severe injury involving the bones in the neck region. The cervical spine consists of seven vertebrae (C1 to C7) that provide support and protection for the spinal cord. When one or more of these vertebrae are fractured, it can lead to serious complications, including damage to the spinal cord, which may result in paralysis or even death.
The cervical spine is a dynamic structure that secures the nervous system of the whole body while keeping the range of movement for the head and neck. It comprises seven cervical vertebrae, which provide reinforcement to the head while permitting side flexion, rotation, flexion, and extension movement.
With a bone fracture reported to account for 56% of cervical spinal cord damages, cervical spine fractures are the main cause of immobility loss and mortality in trauma patients. Injury to the spinal cord could have severe outcomes as it is where the central nervous system combines between the brain and the body. Injury to the spinal cord at the cervical spine can cause whole-body paralysis from the head down, either temporarily or permanently. Depending on the degree of involvement, cervical spine fractures are divided into three distinct groups: C1, C2, and the sub-axial spine (C3 to C7).
Road traffic accidents falls, violence, and sports activities are the most familiar reasons for cervical fractures. We will be concentrating on cervical vertebra fractures in sports that involve physical contact. Sports requiring physical contact, which include American football, ice hockey, football, and rugby, carry a greater chance of cervical damage because events like head-spearing an opponent can induce a cervical fracture. Cervical fractures and injuries to the cervical spine vary depending on the sport and sex.
Pathophysiology
A fracture to the cervical spine can cause reduction(commonly caused by mild trauma in people who have a history of osteoporosis), burst fractures (vertebrae crushed in all directions), or a fracture-dislocation (from road traffic accidents or slips from heights). C1 fractures commonly happen because of axial loading. A combination of compression, hyperflexion, and hyperextension is the most typical reason for C2 fractures. High-impact trauma accidents are called to commonly result in sub-axial cervical spine fractures.
The most vulnerable clinical symptoms directly after fracture are the interruption of spinal cord vascular supply and hypotension or hypo-perfusion, causing hypovolemia, neurogenic shock, and bradycardia. These symptoms happen due to comprehensive bleeding and neurogenic shock resulting in spinal cord ischemia. The rupture of small blood vessels and capillaries facilitates the extravasation of leukocytes and red blood cells (RBCs). These extravasations of immune cells at the trauma area exert stress on the injured spinal tissues and further disrupt blood circulation, thus stimulating vasospasm. This state persists for up to 24 h. Happening of vascular ischemia, hypovolemia, and hyper-perfusion ultimately result in cell death and tissue destruction.
Epidemiology
According to the research, young men who play contact sports frequently suffer cervical fractures as a consequence of trauma. Nevertheless, there is little divide between the majority rates and the specifics of certain hazard factors. This can be because of the truth that examinations frequently used populations who were already revealed to trauma and were done on spinal trauma as a full instead of specifically cervical fractures.
Greatly of the literature agrees road traffic accidents are the most familiar reason, with the majority ranging from forty-eight to sixty-six percent. Contact sports trauma and falling from heights followed, ranging from fourteen to twenty-one percent, and cases of assault ranged from ten to fifteen percent. Despite not being as expected, the literature also recognized the event of specifically atlas fractures in the elderly, with this living primarily alongside other head and neck injuries. An investigation by Khanpara et al. Researchers discovered that closed fractures of C2 and C7 were the most common across all causes, and C1 and C2 fractures were particularly common. The incidence of cervical fractures increasing from 62.3 percent to 67.6 percent between 2005 and 2013 was also favorable.
Evaluation
Indications for cervical spine imaging include regional neck pain, deformity, edema, abnormal mental condition, head injury, or neurological deficiency. Computed tomography is the preferred imaging in acute spine injury as it is more susceptible to the detection of bony cervical spine injury when corresponding to plain radiographs (sensitivity of ninety-eight percent versus fifty-two percent). Additional evaluation of ligamentous structures of the spinal cord with MRI is necessary for determining spinal stability and in planning surgical treatment. Scoring techniques in dealing with cervical spinal cord injury that contains ligamentous, bony, and neurologic damage exist, a standard one is known as SLICS (Subaxial Cervical Spine Injury Classification System), and this can be operated to assist with the evaluation and recommendation of operative or nonsurgical management. A SLICS score of 1 to 3 is nonoperative, a score of 4 is not defined, and a score of 5 or higher is an operative indication. The scoring system is as follows:
Fracture Morphology
- No abnormality – 0
- Reduction of endplate disruption or vertebral body fracture – 1
- Burst – 2
- Distraction – 3
- Rotation or translocation – 4
Discoligamentous Complex
- Intact – 0
- Indeterminate – 1
- Disrupted – 2
Neurologic Status
- Intact – 0
- Root injury – 1
- Complete spinal cord injury – 2
- Incomplete spinal cord injury – 3
Continuous Cord Compression
- With neuro deficit -1
Symptoms of Cervical Spine Fractures
Among more youthful patients, cervical fractures are commonly the cause of high-impact trauma, whilst more geriatric patients can develop cervical fractures from low-impact trauma, particularly if underlying osteoporosis is exist.
Patients can present with neck pain, but this is not constantly the circumstance, particularly if there is contemporary(i.e. distracting) trauma.
There can be contrasting degrees of neurological involvement exist, counting on the level of spinal cord involvement (further discussed here). Alongside possible sensory and motor deficiencies, innervation to the diaphragm and vasomotor tone can even be involved.
Any damage to the vertebral artery from a cervical fracture (particularly in upper cervical fractures) may exist with a posterior circulation stroke.
Everybody with a cervical spine fracture will participate in just different symptoms, relying on the portion of the vertebrae which is involved, where the break has happened, and any other associated trauma, for example to neighboring muscles or ligaments.
Other common symptoms contain:
- Pain at the fracture place– on movement and when pressure is involved
- Decreased range of motion in the neck and nearby region
- Decreased muscle power in the neck muscles
- Decreased mobility
- Decreased balance
- The main problem with moving in the bed or standing up from sitting
Causes of Cervical Spine Fractures
Significant force is required to result in a cervical fracture. common causes of vehicle collisions and falls from a distance. Extreme, sudden twisting of the neck or an extreme direct hit to the head or neck region can lead to a cervical fracture.
Although high-impact injury is usually related to cervical fractures in the more youthful population, low-impact injury is more familiar in the old population. In an examination from Norway, the most typical result was falls from the height and the relative incidence of CS-fx raised particularly with age.
some other causes are given below:
- A football player “spears” a competitor with his head
- An ice hockey player is struck from the back and rams into the boards
- A gymnast ignores the elevated bar during a release move and drops
- A diver hits the base of a shallow pool
The spinal cord, which joins the brain and the body through the nervous system’s central nervous system, passes through the center of the vertebrae, thus any trauma to it can have serious consequences. Damage to the spinal cord is severe and can cause paralysis or death. Damage to the spinal cord at the cervical spine level can cause whole-body paralysis from the neck down, whether temporarily or permanently.
Diagnosis
- In the emergency room, a physician can be capable to rule out a spinal cord injury by investigation, examination of sensory function and motor function, and interrogative a few questions about the accident.
- Yet if the injured individual complains of neck pain, isn’t fully conscious, or has obvious signs of muscle weakening or neurological trauma, emergency diagnostic tests may be necessary.
These tests can contain:
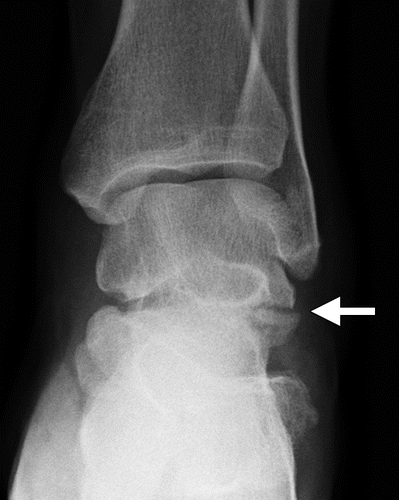
- X-rays. X-rays can expose vertebral (spinal column) problems, tumors, fractures, or degenerative changes in the spine.
- CT scan. A CT scan may deliver a more evident picture of anomalies noticed on an X-ray. This scan utilizes computers to form a series of cross-sectional pictures that can represent bone, disk, and different difficulties.
- MRI. MRI utilizes a powerful magnetic field and radio waves to create computer-generated pictures. This examination is useful for examining the spinal cord and placing herniated disks, blood clots, or other masses that may squeeze the spinal cord.
Some days after trauma, when some of the swellings may have reduced, your physician will perform a more comprehensive neurological exam to choose the level and fullness of your trauma. This concerns testing your muscle power and your capacity to sense light touch and pinprick feelings.
Differential Diagnosis
Differentials for patients presenting with cervical neck pain, with or without neurology, the following injury include
Jefferson Fracture
A Jefferson fracture is the eponymous title assigned to a burst fracture of the atlas. Occipital condyles are forced into the lateral masses of C1 as a result of the axial stress of the cervical spine. They are frequently related to head trauma and other contemporary cervical spinal trauma. These fractures are commonly not stable and account for about a third of all C1 fractures.
Hangman’s Fracture
A Hangman’s fracture, also representing a traumatic spondylolisthesis of the axis, defines a fracture via the pars interarticularis of C2 bilaterally, usually with subluxation of the C2 vertebra on C3. These are the outcomes of cervical hyperextension and distraction, that historically were the consequences of a noose. These fractures can be not stable; for example in case, operative fixation will be needed.
Odontoid Peg Fractures
Odontoid peg fractures are expected cervical fractures, most typical in more senior patients. Patients can offer following low-impact trauma, neck pain is standard. Those who survive might not have significant neurology due to the condition’s possibility of death, particularly when the odontoid has been displaced
other differential diagnoses are the following:
- Acute torticollis
- Cauda Equina
- Cervical strain
- Hanging injuries
- Neck trauma
- Septic shocks
- Spinal cord infections
- Spinal cord injuries
- Spinal cord neoplasms
- Vertebral artery dissection
Prevention
The prevalence of neck fractures caused by sports has gone down as a result of oversight changes and enhancements to athletic equipment. You can assist guard yourself and your family if you:
- Consistently wear a seat belt while you are driving or are a passenger in a car.
- Never dip in a shallow pool region, and be sure that young individuals are adequately supervised when swimming and diving.
- Wear the correct protective gear for your sport and follow all safety requirements, such as utilizing a spotter and appropriate cushioning matting.
- For aged people, conduct a home assessment to provide safe surroundings. Little modifications, like taping down rugs and placing assistive devices around toilets and showers or tubs, can assist decrease the threat of falls.
Immediate First Aid for Neck Injuries
It’s better to suppose there is a neck injury to anyone who has an impact, fall, or collision-kind of trauma.
Conscious patients can or can not have extreme neck pain. They can even have pain arising from the neck to the shoulders or arms, caused by the vertebra squeezing a nerve. There can be some bruising and swelling present at the back of the neck.
Any damage to the head or neck must be considered for a neck fracture. A cervical fracture is a very serious medical emergency that requires instantaneous treatment. Spine-associated injury can damage the spinal cord and could cause paralysis, so holding the neck still is crucial.
In cases where a cervical fracture is possible, the patient’s neck needs to be rested or immobilized (i.e., not moved) until aid arrives so that X-rays can be taken. The doctor will perform a complete neurological assessment to assess nerve function and may request additional radiographic studies, for example, MRI or computed tomography (CT), to specify the extent of the trauma.
Treatment of Cervical Spine Fractures
Treatment for a cracked neck ranges largely. A physician will base their determination on:
- which of the cervical vertebrae has cracked
- the severity of the fracture
- whether the bones have dislocated
- whether there is a spinal cord trauma
Potential treatment choices have:
Cervical braces
Physicians can treat a little compression fracture in one of the vertebrae with a cervical or neck brace. An individual can be required to wear the brace for various weeks or months. They may also require pain medication, either prescription or over-the-counter (OTC).
Traction
Cervical Traction concerns using a device that restricts the motion of the head and neck greater than a brace does. It can possess weights and pulleys to put the bones in the proper position.
A halo vest is a traction device that possesses a hard vest and a ring (halo) about the head. The vest part is associated with the halo with rods. Physicians attach the halo to the skull with particular screws.
Many proofs recommend that operating a halo vest can shorten an individual hospital stay and is slightly more costly than other treatment approaches.
Regardless, this method of treatment is controversial. It is an invasive technique that is not suitable for individual people, including older people and some individuals with obesity.
Surgery
If the fracture neck is extreme and using a brace or traction can not be adequate, a physician can suggest an operation. The operation may assist with dislocated bones in the neck, an extremely not stable neck, or if the trauma has resulted in fragments of bone breaking off.
After having an operation, a person can require physiotherapy and rehabilitation. This management can last for many months or longer to secure a complete recovery.
The treatment alternatives for individuals with a fracture of the cervical or dislocation are fewer and may be typed as conservative (nonsurgical) and surgical (operative). Early management of extreme fractures of the cervical and dislocations can concern skeletal traction and closed reduction, with metal pins set in the skull attached to a pulley, rope, and load. Nonsurgical interventions have brace (orthotic) intervention and pharmaceuticals. There are a number of distinct cervical orthoses accessible from soft collars to hard plastic cervical-thoracic orthoses to the halo vest immobilization technique (which involves pins attached to the skull and reinforced by a padded plastic vest).
Operative intervention repeatedly involves posterior (incision at the back of the neck ) cervical fusion (mending the spine bones together) and instrumentation (small metal screws and rods stabilizing the spine). Other choices have anterior ( incision at front of the neck) decompression and fusion, with or without instrumentation (metal plate and screws). Severely not stable fractures can need anterior and posterior neck operations.
The general purpose of treatment is to maintain or enhance the neurologic function, deliver stability, and reduce pain. If this purpose may be achieved with conservative (nonsurgical) indications, then that is commonly chosen. Yet, due to many cervical fractures and dislocations existing as more not stable and will not sufficiently recover by themselves, operative stabilization is regularly achieved. Operative decompression (removal of bone segment off of the spinal cord) can even be required to maximize a patient’s options for neurologic betterment and healing from a spinal cord trauma.
The all-around approaches and management recommendations for several kinds of cervical trauma are given below.
Atlanto-Occipital Dislocation (AOD)
- Early, all must be cautiously reduced by positioning, a halo vest. Nearly all require Occ-C2 PSF.
Occipital Condyle Fractures
- Type I and II Cervical orthosis or CT orthosis for six to eight weeks with occipital condyle splits from the occiput, utilized halo vest for eight to twelve weeks
- Type III No AO instability, utilized Cervical or CT orthosis for six to eight weeks minimal displacement, utilized halo vest AO instability (bilateral fractures), required Occ-C2 PSF
Atlanto-Axial (C1-C2) Instability (TAL Insufficiency)
- Cord at threat if greater than 5mm instability
- If greater than three attenuated, greater than 5 ruptured, greater than 7mm required operation
- If C1 fractures with greater than 7mm displacement of lateral masses, TAL is insufficient. Can use halo vest for ten to twelve weeks while C1 recovers, then do C1-C2 PSF.
- Can try Halo with youths.
Atlantoaxial Rotary Subluxation
- Reduction with halo traction. Treat depending on TAL insufficiency guidelines. Pain with fixed deformity in C1-C2 PSF.
Atlas (C1) Fracture
Mainly nonsurgical
- Bilateral posterior arch fracture and Burst or lat mass with greater than 2mm display Cervical orthosis ten to twelve weeks
- Burst or lateral mass fracture with 2-7 mm displacement Halo traction 5-10 lbs. seven days, then Halo vest for three months
- Burst or lateral mass fracture with greater than seven mm display Halo traction stryker frame for four to six weeks, then Halo vest for six to eight weeks
- Occasional C1-C2 fusion for AA instability
Odontoid (C2) Fracture
- Type I – Orthosis
- Type II – Smaller than 5mm displacement and ten degrees angulation immediate halo vest
- 5mm displacement or ten degrees angulation reduction with halo traction, then C1-C2 PSF or Anterior odontoid screw fixation, PSF with Magerl approached, or Occ-C2 PSF.
- Type III – Less than 5mm displaced 10-degree angles immediate halo vest greater than 5mm displaced or 10 degrees angle reduction with halo traction, then halo vest
Traumatic Spondylolisthesis of the Axis (C2)
- Type I – cervical orthosis three months (halo vest does not restrict toggle)
- Type II – Reduction with halo traction for four to six weeks, then halo vest. Occasionally C2 pedicle lag screws for the threat of bed rest, incapable to maintain reduction
- Type IIA – Three-month use of an immediate halo vest during image intensification in order to assist overall complete extension and compression.
- Type III: C2 decreases freely, followed by C2-3 PSF with a C2 pedicle lag screw.
Inspect MRI before Open reduction ACDF and then PCF if HNP is large.
Subaxial Fractures (C3-C7)
- DF – Closed reduction, then PCF. ACDF then PCF if HNP. Inspect MRI before Open reduction, and before to closed reduction in intact patients.
- CF – Stable with minutes kyphosis, stable posterior ligaments Cervical orthosis six to ten weeks Not stable with consequential kyphosis, canal compromise ACVF +/- PCF
- VC – Stable with min kyphosis, no canal comp cervical orthosis six to eight weeks Unstable kyphosis or canal compression ACVF
- CE – inspect for disc injury, may require ACDF if not stable.
- DE – ACDF if not stable.
- LF – ACDF vs PCF if not stable.
Although there are methods for treating cervical fractures and dislocations, the precise method of treatment ultimately relies on a variety of circumstances.
- kind and site of the fracture
- the severity of fracture and quantity of displacement
- exists of the spinal cord or nerve compression
- exists of neurologic dysfunction or spinal cord trauma
- patient’s age, medical condition, and related trauma
The clinician must carefully consider a patient’s trauma, and with the overall management approaches for cervical fractures in mind, individualize the management depending upon all of the above-mentioned factors.
Recovery time and tips
A cracked neck can need a person to remain in the hospital for many days or weeks. If an individual has an operation, they can have to stay in the hospital for a longer period.
If the fracture is little and the spinal cord is not broken, many individuals can wear a brace and, with a physician’s approval, heal at-house.
The subsequent guidance can assist individuals who are healing from a fractured neck at the house:
- Wear a neck brace or cervical collar specifically as recommended by the physician. This can contain wearing it all the time, comprising when sleeping.
- Take pain relief prescriptions as prescribed by a physician. Do not take more than they suggest.
- If the pain is not under control, contact a physician.
- Do not take OTC pain medicines in addition to prescription pain medicines unless a physician states to do so.
- Do strengthening exercises if a physician recommends them. Do not do other exercises or any activity that causes the pain to worsen.
- Follow physiotherapy sessions as suggested by a physician. Follow the therapist’s guidance for moving and strengthening the neck at the house.
- Utilize a pillow that is the appropriate height to support the neck and back in alignment.
- Get a physician’s permission prior to returning to work or other activities.
- Try involving a heating pad for up to twenty minutes at a period for additional pain relief. Repeat every two hours as required.
- Try using a cold pack every few hours to assist with swelling. Remove it if it gets excessively cold or feels not comfortable.
- Take care to prevent slips. Wear appropriate shoes when going outdoors, and use nonslip stockings or slippers inside. Terminate throw rugs or other trip dangers in the house.
- Do not drive until the physician tells you it is secure to do so. Even a little automobile accident can result in additional trauma to the neck, and rotating the head to drive can interrupt healing.
After healing from a fractured neck, take steps to help control another accident or damage. Some things that can assist reduce the risk of a fractured neck comprise:
- Constantly wear a seatbelt in the car.
- Wear a helmet and protect supplies during sports.
- Never dive into water that is less than twelve feet deep or if the depth of the water is not known.
- Wear a helmet when riding a motorcycle, bike, or skateboard, or during other identical activities.
- Use cushioning mats and spotters during acrobatics.
Physiotherapy in Cervical Spine Fractures
Your physician can have you see a physiotherapist who will prepare a neck-care protocol just for you. Your physiotherapist will assess your case to choose the most suitable way to help reduce your pain and allow your neck to move better. You will also be presented with methods to take care of your neck so you can prevent pain and prevent additional trauma to your neck.
Your First Visit to Physical Therapy
On your 1st visit, your physiotherapist will like to collect some more knowledge about the history of your neck situation. You may be provided a questionnaire that assists you inform about the day-to-day situations you are having with your neck. The knowledge you give will assist estimate the success of your management. You can also be requested to rate your pain on a scale of one to ten. This will allow your physiotherapist to measure how much pain you have now and how your pain altered once you’ve had management. To help identify the root of your pain and figure out what might be needed to help minimize it, your physiotherapist will ask you some more questions regarding your neck problem. Here are a few questions your therapist could pose to you:
- How long have you had neck pain?
- Where do you sense the pain?
- What causes the pain better or worse?
- How does your pain affect your ADL activities?
- Do you have other problems like headaches?
- Do you have radiating pain in your shoulder, arm, or hand?
- Do you have any abnormal sensations like numbness or tingling?
Physical Therapy Evaluation
Once all this knowledge has been collected, your neck condition will be assessed.
Posture or observation: Posture or observation: Your physiotherapist is going to start by looking at your posture to determine if your pain is caused by an alteration in posture. Imbalances in the position of your spine can cause stress to sore joints, nerves, and muscles. Postures used for a prolonged duration in childhood, with hobbies, or when functioning can impact the balance of muscle power and flexibility. Muscles that have been lengthened over time tend to be more fragile, while muscles that are set in shortened positions can start to dominate the weaker ones. This can put extra strain on regions around the neck that can lead to a problem or make a sore region worse. Helping you improve your posture can frequently make a big contrast in reducing pain.
Range of motion (ROM): Next, your physiotherapist will check the range of motion in your neck. This is a measurement of how distant you can move your neck in dissimilar directions. Neck movements contain flexing the neck frontward and rearward (flexion and extension), flexing to either side (side flexing ), and turning the neck to one side and the other (rotation). Measurements can also be taken of the upper back or movements of the shoulder. Your range of motion is written down to compare how much enhancement you are making with the management.
Neurological screen: Your physiotherapist can want to do some examinations to check the nerves of your neck. This portion of the evaluation examines your reflexes, sensation, and power in your neck, shoulders, and arms. The outcomes of these tests can help your physiotherapist understand which region of the neck can be resulting difficulties for you and may recommend the type of management to support your condition.
Manual assessment: You can be presented with a manual assessment of the muscles and joints of the neck. Your therapist will carefully take you in a position in your neck in multiple directions to make sure that the joints at each level of the neck are moving smoothly.
This will assist in the direction of treatment to the joint that is stiff (known as hypomobility) or where a joint can have been injured and is moving too much (known as hypermobility). Many of the movements you are going to observe are your physiotherapist testing the flexibility of the muscles surrounding your neck. This kind of assessment can assist guide your physiotherapist to understand where your pain is arriving from and which kind of management protocol will assist you the most.
Special tests: Other special tests can be executed if your physiotherapist thinks your neck pain is arising from other regions or causes. Another region that can be required to be observed contains:
- Thoracic outlet: This is where a bunch of nerves and vessels make their way out of the chest cavity and travel down the arm. Difficulties in this region can result in abnormal sensations like numbness, tingling, pain, or even coldness in the arm and hands.
- Temporomandibular joint (jaw): Difficulties here can result in headaches, pain in your upper neck region, and also result in spasms in the muscles of the neck.
- Thoracic spine: Difficulties starting in the upper back can contain joints and muscles of the thorax or even in the alignment of one or more ribs, which can result in pain radiating pain toward the neck and shoulder.
- Nerve tension: Nerves of the mid and lower neck travel down the arm to supply the arm and hand. Irritation or scarring around the covering of these nerves can lead to pain that radiates from the neck to the upper back region or also radiates into the arm. By engaging scarred or irritated regions across the nerve, a treatment called a”neural mobilization” can be utilized to free up movement in the nerve and reduce the soreness you sense.
- Ergonomics: Ergonomics is a method to notice where and how you do your job or hobby activities. Your physiotherapist can like to understand your ergonomics to evaluate if the method you do your ADL activities is producing your situation more worsen. Periodically also simple modifications of your hobby, ADL activity, or job place can make a significant difference in lessening the symptoms of the neck.
- Palpation: The assessment is generally complete with palpation. Palpation is when your physiotherapist senses the soft tissues near the neck. This is performed to inspect the skin for alterations in temperature or texture, which can indicate if you have inflammation or nerve irritation. Palpation is also used to figure out whether there are any difficult places or spasms in the muscles which surround the neck and upper back. This too can provide your physiotherapist with a better understating of which management protocol will assess you the most.
- Treatment plan: Once the assessment is finished, your physiotherapist will jointly together on a treatment protocol. The treatment protocol details the kinds of treatments that will be utilized for your situation. It provides an indication of how many visits you will require and how long you can require therapy sessions. It additionally involves the objective that you and your physiotherapist believe will be most beneficial in performing your assignments safely and with a minimum of soreness. Ultimately, it will contain a prognosis, which is how your therapist supposes the treatment will assist you to improve.
Physical Therapy Treatment
Controlling your pain and symptoms
- Relieving pain: Your therapist may select from one or more of the subsequent tools, or modalities, to assist control the symptoms you are having:
- Rest: Resting on your painful joints and muscles gives you quiet soreness and allows your neck to recover. If you are keeping pain with an activity or movement, it must be an indication that there is yet irritation going on. You must try to prevent all actions and activities that elevated your pain. In the initial phases of your situation, your physician or physiotherapist may like you to use a soft or hard neck collar to limit neck movement almost totally.
- Specific Rest: Specific rest facilitates the safe movement of the joints and muscles on either side of a hurting area while guarding the sore spot during the earlier recovery phase. Special exercises can be provided to facilitate the safe activity of the shoulders and upper back. If you’ve been recommending a collar, you will probably be advised to take it off some times a day so you can do some gentle and controlled movements.
- Positioning: The conclusions of the evaluation will provide your therapist with a clear picture of how to arrange your neck for the greatest level of comfort.
A special pillow familiar as a contour pillow, may be recommended to assist get your neck in the most relaxed position while sleeping or resting. A commercial neck roll, or even a rolled towel, can be slid beneath your pillow case so that when you lie back, the roll fills in and sustains the curve in your neck. Your physiotherapist might suggest other ways to rest your neck and head to help relieve arm pain resulting from your neck.
- Ice: Ice makes the blood vessels in the sore region become narrower, named vasoconstriction. This permits the reduction of inflammation that is inducing pain. A few methods placed ice on contain cold packs, ice bags, or ice massages. Cold packs or ice bags are commonly placed on the sore region for ten to fifteen minutes. Ice massage is performed by massaging an ice cube or ice cup on a sore place or tender point. It’s as simple and easy as freezing a small paper cup whole of water. Once the water is frozen, simply draw off the top inch of the cup and massage the bare ice on the sore place for three to five minutes, or until it senses numbness.
- Heat: Heat makes blood vessels get bigger, known as vasodilation. This action assets to flush away chemicals that are making your neck broken. It also helps to get in nutrients and oxygen which help the site recover. True heat, including a moist hot pack, a heating pad, or a warm shower or bath, is preferred to moisturizers that only provide a sense of heat. Hot packs are commonly put on the sore region for fifteen to twenty minutes. Special care should be carried out to make sure your skin does not overheat and burn. It’s also not a fair idea to rest with an electric hot pad at dark.
- Soft tissue mobilization or massage: Physiotherapists are qualified in multiple various conditions of massage and mobilization when treating the neck. Massage has been demonstrated to calm pain and spasm by allowing muscles to relax, obtaining a fresh circulation of oxygen and nutrient-rich blood, and washing the region of chemical irritants that come from inflammation. Soft tissue therapies can allow tight muscles to relax, getting them back to a normal length. This will assist you start to move with less pain and greater relief. Physiotherapists have special training in a type of various methods to mobilize or massage. These can contain slowly gentle strokes, known as effleurage. Myofascial release approaches help restore better movement by getting the thick layer of fascia below the skin and around muscles to “give”.Strain-counter-strain physiotherapy is particularly beneficial when painful spots have caused muscles to block movement. The treatment is commonly done in a way that the muscle is put in a special position, commonly where the muscle is contracted. The position is maintained prolonged sufficiently to “reset” the nerve input to the muscle. Another way to help soft tissues “move” is by the use of the muscle energy technique. Your physiotherapist will put your muscle in a particular position and then direct you to utilize your muscles against the therapist’s force. As you rest, your therapist will gradually “take up the slack”, delivering a stretch on the muscle.
- Joint mobilization: These are graded forces and movements that are performed by trained physiotherapists. Gently graded forces assist lubricate joint surfaces, lessening stiffness, and assisting you start moving with less pain. If discomfort is ignored, it can quickly become uncomfortable and turn into a “cycle of pain and muscle guarding.” To put it another way, the pain could cause your muscles to tighten in an effort to protect the injured joints, making it impossible for you to move your neck at all. in which your muscles try to protect the sore joints, keeping you from wanting to move your neck at all. When movement quits, your brain brings an uninterrupted discharge of pain sensation. Ouch! Because your muscles are trying to “protect” you from causing damage to the action, this ends up resulting in a cycle of even more pain and muscle spasms. By using gentle forces, or mobilizations, your physiotherapist will start to halt the flow of pain information, which assists muscles to relax. Once your muscles start to relax, you will start to feel other feelings than pain. More intensive types of mobilization may be used as your pain reduces to stretch the tissues around the joint and assist your neck to recover better movement.
- Traction: Sore joints and muscles in the neck frequently feel improved when a traction “pull” is utilized. Your physiotherapist will do a test at first to determine whether you can feel better with this kind of therapy. There are many different strategies to get traction. There are traction machines that enable you to rest comfortably with either a harness or cushion beneath your neck. The machine is set to pull on this halter or cushion for a definite quantity period of time and stress. Manual traction is some other way for your physiotherapist to set a graded pull on your neck. Additionally, you may be provided traction apparatus to use at home. The quantity of pull used is going to depend on your health. Early on, a gentle on or off pressure may be preferable to assist reduce pain, especially if there is arthritis pain. If a joint is significantly tight or uneasy, greater traction can help alleviate the pain.
Exercises
Strengthening your neck
Movement is also effective, even when your neck is even in pain. Cautious movements recommended by your physiotherapist can safely reduce pain by supplying nutrition and lubrication to impaired and sore regions. The movement of joints and muscles likewise signals the nervous system to obstruct incoming pain. Common movement exercises contain an active range of motion, in which you are facilitated to move your neck in directions that do not hurt. Your physiotherapist will assess which movements will be safest and most satisfactory for you. In some conditions, the pain will lessen with the addition of stress in one or another direction. Again, your physiotherapist will be required to decide which movements are best for your situation. Prevent movements that break or seem to irritate the soreness in your neck.
As your neck becomes get better, the exercises will be altered to concentrate on improving the general fitness of your neck. These changes will concentrate on exercises for:
- Flexibility
- Strength
- Coordination
- Aerobic conditioning
Exercises that improve flexibility support reduce pain and make it more comfortable to hold your neck and spine in a healthy position. Tight muscles resulting imbalances in spinal movements. This can make injury to these structures more possible. Flexibility exercises for the neck, chest, and upper shoulders can be useful in demonstrating safe movement. A slow and gradual progression of stretching exercises can improve flexibility in this region, ease pain, and reduce the chance of injury again.
The following phase of exercise concentrates on the power of the muscles that keep the neck. These muscles support and bring the spine into a secure place –and hold it there! Trained muscles can maintain your neck healthily by bringing it into a more suitable posture. A sequence of strengthening exercises, known as stabilization training, is a method to get a more useful balance in the muscles around your neck, chest, and upper back. These stabilization exercises are helpful in supporting your neck in safe places while you are performing or when you are doing other daily activities. Strengthening and stabilization exercises are easy to do at the house and don’t have to need any costly tools. By practicing these activities frequently, you will become relaxed retaining your neck in healthy places and postures with all your movements.
Powerful muscles require to be coordinated. As the power of the spinal muscles improves, it becomes necessary to prepare those muscles to work together. Learning any physical activity brings to practice. Muscles must be prepared so that the physical activity is under control. Muscles that are prepared to control the safe movement of the spine support decrease the chance of injury again. You will be prepared for exercises to assist train your neck, chest, and upper back muscles to work together in rescuing your spine.
Eventually, attention will be directed to advancing your general wellness. The word aerobic standards” with oxygen”. By utilizing oxygen as they work, muscles are sufficiently able to move continually, rather than in spurts. Wellness training permits the muscles to become more efficient at getting nutrients and oxygen from the blood. As the muscles use up the nutrients and oxygen, chemical waste products are constructed that can result in pain. Training also improves the ability of muscles to get rid of these waste products.
Exercise has other advantages as well. Strong exercise can result in chemicals known as endorphins being discharged into the blood. These chemical hormones work as natural pain relievers in decreasing your pain. It will be essential that you choose an aerobic activity you can enjoy and adhere to it!
Once your pain is maintained, your range of motion is enhanced, and your strength is producing, you will be progressed to a final home protocol. Your physiotherapist will give you many thoughts to assist take maintaining any more soreness at home. You will be given some methods to keep working on the range of motion and strength too. Before you are done with physiotherapy, more measurements will be brought to see how well you’re doing now corresponded to when you first began therapy.
Prevention and long-term self-care for the neck
Is this your first experience with neck trouble? Perhaps you’ve had continuing difficulties for multiple years. In either condition, your most satisfactory bet for preventing neck difficulties in the future is to get a handle on methods you can avoid additional neck pain or trauma. It is also useful to know how to take maintenance of your neck if pain hits again.
Posture: Using a healthy posture is like maintaining a security shield in front of forthcoming neck issues. Pain and trauma may be controlled. When your joints are placed in their secure position—or neutral posture—the body functions like a graceful device. It functions safely and even more constructively. When unstable postures are operated on, issues are more probable to happen. Prevention of neck pain and trauma has a lot to do with maintaining a balanced position of the spine and limb. When standing, this balance pursues a vertical line from ear to ankle. In a seated place, this line falls from the ear to the hip. A rule of thumb for the limbs is to keep them in their relaxed positions.
There are 3 natural curves in the spine. From a side view, the neck (cervical spine) curves barely inward. The mid-back (thoracic spine) curves just laterally. The low back (lumbar spine) curves are barely medial. Maintaining this relationship while standing, sitting, or moving is the foundation for healthy posture. When moving, flex the hips to prevent rounding or straightening the spine. This supports the spine’s safe during movements like lifting and walking.
For better sitting posture, sit with an adequate straight alignment of the spine by utilizing a satisfied chair planned to help the right posture. Prevent slouching by maintaining your low back against the back of the chair. Flexed the head forward strains the neck and impacts the nerves and arteries causing to the arms. Your shoulders must be comfortable, and the elbows, hips, and knees should be flexed at right angles (ninety degrees). Preventing stress to the back of the knees. Your foot must be maintained flat on the base or supported by a footrest.
Uncomfortable posture puts pressure on the body which can cause neck pain. Slumping with the spine or causing the head forward places the body out of alignment, forcing the limbs to be stretched and bent. Excess bending (flexion) or straightening (extension) of the spine increases the probability of damage. Symptoms of abnormal sensations like pain, tingling, or numbness in the arm or hand can even come from inadequate neck posture. The little inward curve of the neck balances the head on the spine. Prevent excessive postures, like staring up at the sky, or flexing your head down for prolonged periods of time when reading a book. Maintaining a balanced posture is a measure you can use to avoid additional trauma and pain in your neck.
Ergonomics: Ergonomics is observed in the method individuals do work. What does ergonomics have to do with the pain in your neck? It can have many things to do with it. It’s likely that even little modifications in the path you do your job or ADL activities can reduce the pain you sense now while avoiding additional neck injury or pain.
In many conditions, it is most suitable to have somebody prepared in ergonomics, like a physical or occupational therapist, check your job place and the way you do your job. The 1st step will be for them to ask you a few questions regarding your job, which creates good logic. Since you’re the one doing the job, you will have an expert idea regarding what appears to be performing, what could be performing differently, and what tasks seem to be leading the most issues for you. Once these queries are covered, the evaluator will like to watch you do the work tasks. A region that will be mentioned includes the postures you use, repetitions to complete the task, rest time between tasks, and the quantity of load you are dealing with. For office employees, the examiner will examine at the alignment of the computer monitors, seats, height of the desk, etc. Other regions that can be considered contain work heights, tools of the trade, lighting, and temperature. It’s also beneficial to look at your work postures and work tasks to notice if what you are doing can be done with less pressure and strain on your body.
When the workplace evaluation is complete, you or your superintendent will likely be given some suggestions—a few of these can even be ones you arrived up with! Ergonomics does not ever have to involve costly changes. Even minor modifications can make a massive difference in reducing your pain and preventing further problems.
Job Place Plans: These techniques are thoughts of how to work with more significant security and even more profitable productivity. Have you ever sensed pressure or anxiety at work? Chances are fair that you wouldn’t have pain or worry if you didn’t. The truth is that somebody is frequently known as one to do even more with more occasional resources. They are faced with more responsibility and more deadlines to get their tasks completed. The health of your neck can be at threat with this mounting stress. But scientists have allowed us to learn that there is a defense in the face of these mounting stresses. They have shown the significance of using the “Three R’s” to help ease tension and relieve neck pain at work:
- Rest: This contains taking regular breaks during job hours. It also suggests picking alternate movements to get your mind prepared for a new job task. Movements have deep breathing, walking, napping, or exercising.
- Relaxation: Take a weight off. Lie back. Turn down the lights, and hear to your favorite video or CD. Try to breathe gradually and deeply, permitting your abdomen to increase and drop rhythmically. Using visual imagery can even help in relaxation. Try to imagine each muscle resting one after another.
- Recovery: Our bodies require a chance to recover. Repeated and extended activities can be demanding on the body if it doesn’t get sufficient rest to recover. Recovery helps repair these sore and painful tissues across the way, maintaining their health.
Whether at work or at the house, you may use these thoughts to assist avoid neck pain and trauma. Here are a few extra tips to use at work to prevent stress and maintain your neck healthily:
- Be Relaxed. Attempt to work with your muscles relaxed. To stay calm, look relaxed.
- Pace Yourself. Maintain an even keel. Prevent sudden shifts in your workload. Attempt to prevent last-minute “panics” to encounter deadlines.
- Take a Break. Take a 30-40 second “microbreak” per 20 to 30 minutes to do a few deep breathing and some exercises. Take periodic minutes per hour to do some exercises, get a drink, or go bug a colleague. Utilize your lunch break to take a small rest or a walk.
- Altered Positions. Prevent holding your neck, trunk, or limbs still for a lengthy period of time. Plan methods to get the job done using various positions. Sit for a moment, then stand for a moment. Or simply readjust your technique to the task.
- Rotate Duties. Rotating or sharing your tasks can be a joy by offering a new work setting while giving your body a chance to heal.
- Prevent Caffeine and Tobacco. These can promote anxiety, lower blood circulation, and promote awareness of neck pain.
FAQ
A fracture of the neck can paralyze you or even consequence in death. If you fracture your neck, you will sense severe pain, swelling, and a loss of feeling in your arms and legs. You shouldn’t be moved, and you must go to the hospital correct away.
Fractures through the C2 dens can be typed as type I, II, or III. Type I is the avulsion of the tip of the dens, type II is a fracture via the base of the dens, and type III is a fracture expanding into the C2 vertebral body. Type I and III fractures must be managed in a rigid cervical collar or halo.
Most cervical spine fractures happen especially at 2 levels: one-third of injuries happen at the level of C2, and one-half of damages happen at the level of C6 or C7. Most fatal cervical spine trauma happens at upper cervical levels, at craniocervical junction C1 or C2
Operation frequently concerns a posterior (back of the neck incision) cervical fusion and healing of the spine bones together utilizing little metal screws and rods to stabilize the spine. Other alternatives contain anterior ( incision at front of the neck) decompression and fusion, with or without metal plates and screws.
Unfortunately, there’s no method to reverse back the damage to the spinal cord. But investigators are constantly working on the latest treatments, possessing prostheses and medications, that can encourage nerve cell rejuvenation or enhance the function of the nerves that stay later to a spinal cord trauma.
A physician can suggest a cervical spinal fusion operation to manage neck pain when nonoperative treatments do not support or are not suitable. Causes for operation can contain: To stabilize the neck and avoid further damage to the spinal cord later an accident or trauma.