
Clavicle Bone
Table of Contents
Introduction
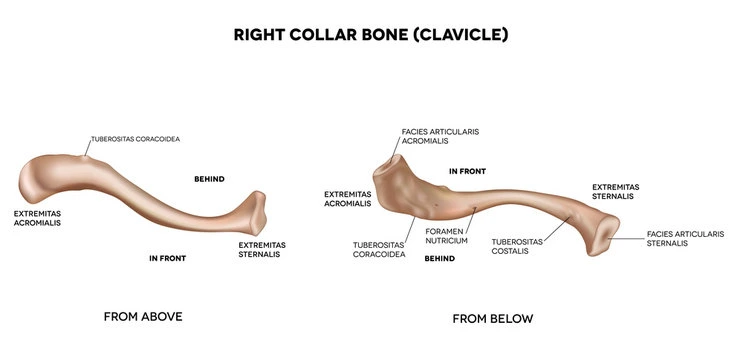
The clavicle (Latin a small legend) is a long bone. It keeps the shoulder so that the arm component can turn out from the chest.
The clavicle moves the important weight of the limb to the sternum. The bone includes a cylindrical part named the shaft, and two ends, lateral and medial.
Side determination
The side to which a clavicle belongs can live selected in the subsequent grades.
The lateral end is facedown, and the medial posterior exists big and quadrilateral.
The pole is a little curved so that it stands convex forwards in its medical two-thirds and concave forwards in its lateral one-third.
The inferior texture is grooved longitudinally in its center one-third.
Peculiarities of the clavicle
It is the greatest lengthy bone that fibs horizontally.
It is subcutaneous throughout.
It is the preferred bone to form ossifying.
It is the only long bone that has two preliminary middles of ossification.
It is the best long bone that calcifies in a membrane. There is no medullary cavity.
It is sometimes stuck by the median supraclavicular nerve.
It accepts the weight of the upper limb via lateral one-third via the coracoclavicular ligament and moves the significance of the upper limb to the axial skeleton via the medial two-thirds part.
Features
Shaft
The shaft is dividable into the lateral 1/3 and the medial 2/3.
The sideways one-third of the post is flattened from overhead downwards. It includes two boundaries, anterior and posterior.
The anterior border is concave forwards.
The posterior border is convex backward.
This part of the bone has two textures, superior and inferior.
The medial two-thirds of the post is rounded and is declared to maintain four surfaces.
The anterior surface is convex forwards.
The posterior surface is smooth.
The greatest surface is irregular in its medial part.
The nether character includes a rugged ovoid impression at the medial end.
The sideward half of this texture has a longitudinal subclavian trough.
The nutrient foramen tales at the sidewards rear of the track.
Sidewards 1/3: flattened in the area and thinner
consists of 2 boundaries: anterior and posterior and 2 characters: superior and inferior.
anterior border: concave forwards and delivers origin to the deltoid muscle.
posterior border: convex backward and delivers attachment to the trapezius muscle.
the superior surface: is subcutaneous. inferior surface: shows conoid tubercle and trapezoid ridge which gives attachment to the conoid ligament (medial part of the coracoclavicular ligament) and trapezoid ligament (lateral part of the coracoclavicular ligament) respectively.
Medial 2/3: circular in the province and more viscous
consists of 4 surfaces
anterior surface: convex forwards and provides origin to the pectoralis major.
posterior surface: concave backward and gives origin to sternohyoid muscle.
the superior surface: is rugged on its medial factor. the inferior surface: has an irregular ovoid image at the medial end for the costoclavicular ligament and shows a subclavian groove that delivers attachment to the subclavius muscle.
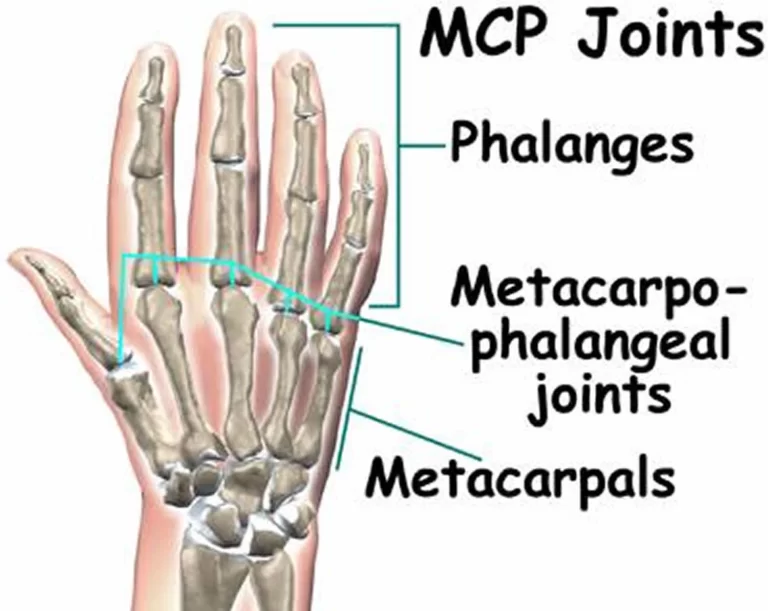
Lateral (Acromial) End:
communicates with the acromion process of the scapula to possess the acromioclavicular joint.
Medial (Sternal) End:
communicates with the clavicular crevice of the manubrium sternum to construct a sternoclavicular joint.
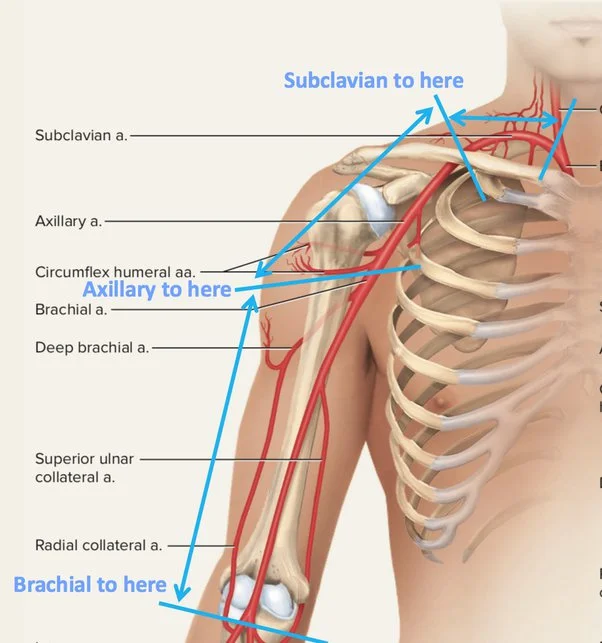
The third feature of the subclavian plates and the compartments of the brachial plexus pass behind the medial third of the shaft of the clavicle, separated only by the thin subclavius muscle. by the elements of a fractured clavicle. Posterior connections of the Sternal end of the clavicle. Behind the sternoclavicular joints fib the typical carotid artery on the left and the clavicle that’s the more bifurcation of the brachiocephalic route on the privilege.
The interior jugular vein lies undersized better laterally on either flank. these large receptacles stand isolated from bone by the strap muscles: the sternohyoid and sternothyroid. The lateral end is formed by intramembranous ossification while medially it is formed by endochondral ossification. It consists of a group of cancellous bones wrapped by a closed bone shell. The cancellous bone forms via two ossification centers, one medial and one lateral, which fuse later on the lateral or acromial (Greek peak of the shoulder) end is flattened from above downwards. It endures a factor that emits with the acromion procedure of the scapula to compose in the acromioclavicular joint. the medial or sternal ending is the verified quadrangular and articulates with the clavicular gap of the manubrium sternum from the joint.
sternoclavicular joint.
The articular surface grows to the deficient characteristic, for representation with the first costal cartilage.
Muscle attachments
In the end, the margin of the articular consistency for Its acromioclavicular joint delivers the wing to the common joint capsule. At the medial rear, the margin of the articular character for the sternum delivers attachment to the fibrous capsule of the sternoclavicular joint all around the articular disc posterosuperior. interclavicular ligament superiorly. lateral one-third of the shaft. The anterior boundary delivers conception to the deltoid muscle. The hindmost borderland supplies insertion to the trapezius muscle.
The conoid tubercle and trapezoid ridge give extension to the conoid and trapezoid portions of the coracoclavicular ligament and function of the medial two-thirds of the shaft. most of the anterior exterior furnishes the origin of the pectoralis major muscle. Half of the barbarian outstanding covered delivers conception to the clavicular head of the sternocleidomastoid. the oval impression on the interior surface at the medial end gives attachment to the costoclavicular ligament.
The subclavian is the furrow that gives insertion to the subclavius strength.
The margins of the trough provide affection to the clavipectoral fascia.
The rearward texture comparable to the medial end delivers the origin to the sternohyoid muscle.
The subclavian vessels and cords of the brachial network key towards the axilla lie between the nether surface of the clavicle and the upper surface of the 1 rib.
The Subclavius muscle functions as a protector.
The nutrient foramen transmits a component of the suprascapular route.
Ossification
The clavicle is the rather bone in the body to ossify. besides its medial end, it calcifies in the membrane. it calcifies from two primary middles and one secondary center. the two preliminary camps appear in the shaft between the fifth and sixth weeks of intrauterine life and fuse about the 45th day. the secondary center for the medial end appears during 15-17 years and fuses with the shaft during 21-22 years. occasionally, there may be a secondary center for the acromial end.
Clinical importance
Clavicle (Collar Bone) Fracture
Functions of the clavicle
To exchange forces from the upper limb to the axial skeleton. to act as a support keeping the arm free from the compartment, to depend associated principally on the trapezius to give an attachment for the muscle’s weakest point of the clavicle. The intersection of center 2/3 and sidewards 1/3 (the connection between 2 curvatures) is the most important pinpoint of the clavicle and hence is the most vulnerable part to fracture.
Cause of Clavicle fracture
Communication of strengths to the axial skeleton in downfalls on the shoulder or indicator may verify better unique than the stability of the bone at this site and this indirect force is the usual cause of fracture.
Clinical features of Clavicle fracture
When the fracture occurs, the trapezius is unable to support the weight of the arm so the characteristic picture of the patient with a fractured clavicle is that of a man assisting his sagging upper limb with his further hand. because the clavicle is directly under the skin and is not a leader with muscle, a fracture can smoothly be palpated, and frequently appear.
Anatomical Basis
Fractured lateral component: despairing (lowered removal by earnestness) and tightened medially (abducted by a twinge of the shoulder adductors, principally the teres major, latissimus dorsi, and pectoralis major) Fractured medial fragment: slight height by sternocleidomastoid Clavicle fracture in X-ray cleidocranial dysostosis.
The clavicles may stand congenitally absent or imperfectly materialized in infection-contacted cleidocranial dysostosis. In this situation, the shoulders decrease and can be corresponded anteriorly in a show of the chest. anatomical demonstration clavicle.
Summary
The clavicle is completed up of a medial two-thirds of the clavicle which exists circular in section and convex anteriorly, and a sidewards one-third which is flattened in compartment and convex posteriorly. medially it communicates with the manubrium at the sternoclavicular joint (this joint possessing an articular disc) and is also associated with, the first costal cartilage by the costoclavicular ligament.
FAQs
The clavicle, popularly understood as the collarbone, is a function of your shoulder. It is a principal bone that attaches the arm to the rest of the skeleton. Its processes comprise authorizing the free motion of the shoulder out from the body. Along with the rib cage, the clavicle supports protects the core from superficial concussion.
The anterior capsular ligament is more serious and more powerful than the posterior. The capsular ligaments connect particularly to the epiphysis of the medial clavicle; therefore the physis is extra-articular and sensitive to injury during injuries to the medial clavicle.
The clavicle provides consent to the shoulder girdle by acting as a support between the scapula and sternum. Due to its S-shape, the furthest end depicts a much larger rotation during constituent elevation than its internal end.
Genetic or developmental shorting of the clavicle is a distinctive and unattended disorder directing to a digressive function of the scapula. It demonstrates in preadolescence as irregular stance and maybe family. It renders the tiniest disability and simulated patients do not demand therapy.
The most powerless and temperate bone in the human is the clavicle or coupling bone. Because it is a tiny bone that manipulates horizontally the clavicle bone. passes your breastbone & collarbone, it is easy to break. Moistness creates up to 31% of the significance of your bones. Your bones are four times the moments more effective than a concrete pound for pound.

10 Comments