
Atlanto-occipital joint
Table of Contents
What is atlanto-occipital joint?
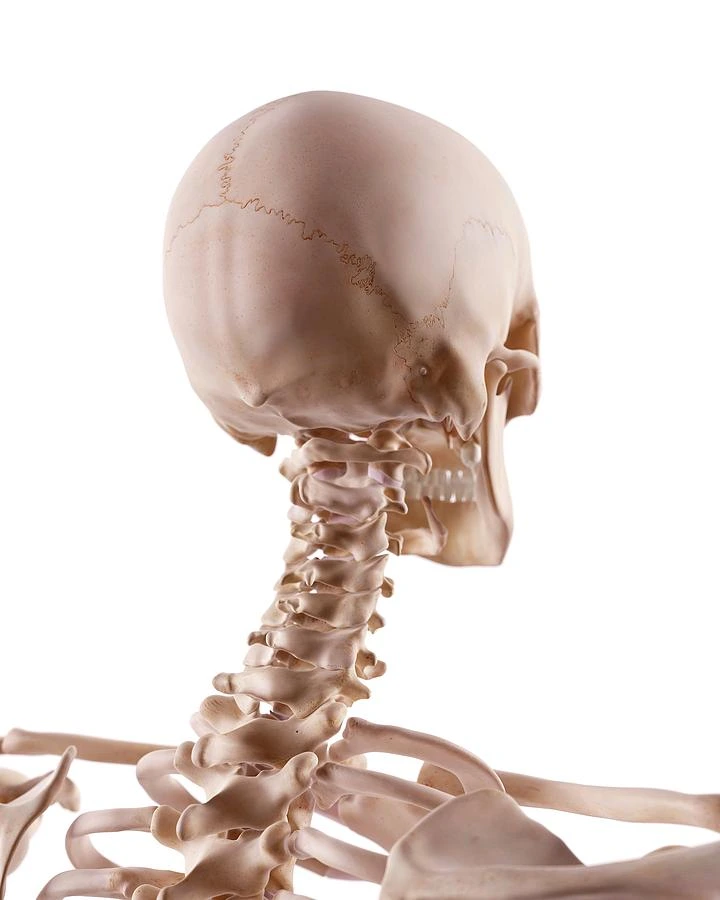
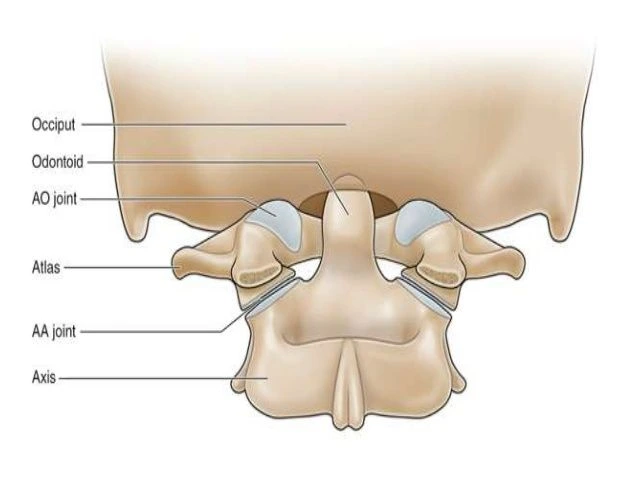
This joint [ atlantooccipital joint ] is a paired symmetrical articulation between the base of the skull & the cervical spine. This joint is also known as the C0-C1 joint. Along with the atlantoaxial joint & it makes up a group named the craniovertebral joints.
The primary movement of the atlantooccipital joint is flexion-extension. This action allows nodding of the head, as seen when indicating permission (the “yes” movement). Functionally, these 2 ellipsoid joints (condyloid joint) accomplish their actions simultaneously and thus can be mechanically evaluated as a single joint.
The upper cervical spine area is designed to allow for significant movement, at the sacrifice of stability. The stability of the joint in the craniocervical region is mainly maintained by the articular surfaces, ligaments, fibrous capsules, & surrounding muscles.
Articular surfaces
The atlantooccipital joint is the synovial joint manifestation between the occipital bone & atlas (the first cervical vertebra). These articular surfaces are elliptical or oval, with the concave articular aspects of the C1 vertebra articulating with the convex surfaces of the occipital bone, and there is no intervertebral disc between the occiput and C1. All the articular surfaces are lined with hyaline cartilage, and the first cervical vertebra houses the inferior articular facets.
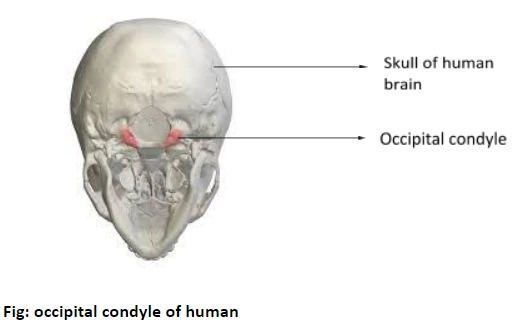
These facets are situated on the superior part of the vertebra’s lateral mass. They are oval-shaped, concave, and tilted slightly medially. The 2 long axes run obliquely in the anteromedial path & encounter at the midline just anterior to the atlas. The superior articular parts are situated on the inferior portion of the occipital bone, in the area of the occipitalcondyles. These 2 rounded bumps are elliptical, convex, and elongated on both their long & short axes. The condyles are directed anteromedially & encountered directly lateral to the anterior 1/2 of the foramen magnum.
Ligaments and joint capsule
Each atlantooccipital joint is surrounded by a loose, thin articular capsule. This capsule is formed of fibrous tissue and lined with a synovial membrane. It connects to the margins of the articular facets. Capsular thickenings can be recorded on their posterior and lateral parts.
Many ligaments cross the atlantooccipital joint & participate in its stability.
These are :
- Ligamentum nuchae
- Apical ligament
- Alar ligament
- Lateral atlantooccipital ligament
- Lateral atlantooccipital ligament
- Anterior atlantooccipital membrane and ligament
- Posterior atlantooccipital membrane
- Tectorial membrane
Of these, two primarily attach to the occipital bone with the atlas and therefore are considered the predominant ligaments of the atlantooccipital joint.
These are the:
- Anterior atlantooccipital ligament (and membrane)
- Posterior atlantooccipital membrane
Anterior atlanto-occiptal membrane ( ligament)
The anterior atlantooccipital membrane is a dense bar of fibrous tissue that lengthens from the anterior border of the foramen magnum to the upper edge of the anterior angle of the atlas. Medially, it is strengthened by the anterior longitudinal ligament as the anterior atlantooccipital membrane, and laterally it corresponds with the joint capsule of the atlantooccipital joint.
Posterior atlantooccipital membrane
The posterior atlantooccipital ligament ( membrane ) is a thin ligament that covers the posterior part of the atlantooccipital joint. It runs from the posterior margin of the foramen magnum superiorly to the upper border of the posterior arch of the atlas, inferiorly. Its lateral margins correspond with the posteromedial joint capsule along its route. The proximity of the posterior atlantooccipital membrane to the C1 nerve & vertebral artery is an essential clinical landmark.
Innervation
This joint [ atlantooccipital joint ] is innervated by the anterior rami of the spinal nerve [ C1 ].
Blood supply
This joint [ atlantooccipital joint ] receives blood from an anastomosis developed by the deep vertebral, cervical, & occipital, arteries.
Movements
Being an ellipsoid joint, the atlantooccipital joint permits motion in 2 degrees of freedom. However, the principal motion available at the atlantooccipital joint is that of flexion and extension. This is because of the shape of the atlantal sockets, and adequately deep to control extreme translation of the occipital condyles & permit the atlantooccipital joint to provide some strength.
Flexion and extension activities occur in the anteroposterior plane, around a transverse axis. In flexion, the convex occipital condyles simultaneously roll forwards and glide posteriorly over the concave aspects of the atlas. Thus moving the occipital bone out from the posterior arch of the atlas. This permits a forward tilting, or downwards nod, of the head to occur such as that noticed when indicating approval (the “yes” movement). Flexion action is restricted to around 5 to 10 degrees by the fibrous tissues around the joint [ posterior atlantooccipital membrane, joint capsules, and ligamentum nuchae ] and the posterior suboccipital muscles.
During extension, contrasting movements occur. The condyles of the occipital are rolled backward & slide anteriorly on the atlantal parts, and closing the stretch between the occipital bone & the posterior arch of the atlas. Approximation of the occipital bone, the atlas, & the axis specifies the extension ( ROM ) range of motion to around 10 degrees.
Lateral flexion is not an effective movement at the atlantooccipital joint, in terms of a range of motion ( ROM ). Some studies determine lateral flexion of the upper cervical spine to approximately 5 to 8° on each side. Likewise, lateral flexion in the upper cervical spine is both a corresponding motion & a double-joint action. The coupled movement suggests that lateral flexion occurs together with a small degree of contralateral rotation. The double-joint activity suggests that activity occurs in more than one joint at the same time. Thus the integrated moves to accomplish upper cervical spine lateral flexion are as follows; a small degree of contralateral slide occurs at the occipital condyles, at the same time one occipital condyle moves relatively anteriorly while the other moves in a posterior direction, alongside these activities the second vertebra is rotated (relatively) against the 3rd cervical vertebra, producing an overall range of motion ( ROM ) for upper cervical spine lateral flexion of 5 to 8 degree.
Muscles acting on the atlantooccipital joint
The postvertebral & anterior neck muscles act on the atlantooccipital joint, contributing to the movement of the cervical spine.
The primary flexors of the head on the neck are the rectus capitis anterior & longus capitis muscles.
The major extensor muscles are:
- Rectus capitis posterior major
- Rectus capitis posterior minor
- Obliquus superior capitis
- Semispinalis capitis
- Splenius capitis
- Trapezius muscle
However, the identical muscles involved in these moves can vary, depending on the initial position of the head. When the person is in a supine position and required a strong action to lift the head & flex it forward on the neck. In this circumstance, the anterior neck muscles work as the prime movers. This contains the sternocleidomastoid, longus capitis, and rectus capitis muscles. When the head is in a comfortable place, and not needed the same strength as the weight of the head can move the head into a flexed position. In this case the posterior muscles of the back & neck act to prevent the forward bend exercise. These involve the trapezius, splenius capitis, longissimus capitis, semispinalis capitis, and suboccipital muscles.
Similarly, an extension of the head from an upright position is maintained by the anterior neck muscles [ e.g. sternocleidomastoid and longus capitis ], which act against the weight of the head. When in a prone position, prime movers are required to lift the head into extension. These involve rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis superior, semispinalis capitis, splenius capitis muscles, and the cervical region of the trapezius.
Lateral flexion of the head occurs via concurrent movements of the anterior & posterior neck muscles.
These involve:
- Rectus capitis lateralis
- Trapezius
- Splenius capitis
- Semispinalis capitis
- Sternocleidomastoid
- Obliquus capitis superior
- Rectus capitis posterior minor muscles
The correlated motion of rotation is supported by
- Obliquus capitis superior
- Rectus capitis posterior minor
- Splenius capitis
- Sternocleidomastoid
Clinical relations
Dislocation: Dislocation of the atlantooccipital [ AOD ] joint is a potentially fatal craniocervical damage. It can result from a high-speed effect such as a motor vehicle accident.
According to the recommendation of the occipital dislocation, AOD is categorized into 3 types;
- Anterior displacement
- Posterior displacement
- Longitudinal distraction.
Dislocation is accompanied by damage to the associated ligaments. The severity of the injury relies primarily on the degree of dislocation. Stage I & II represent none / minimal displacement with adequate preservation of the surrounding ligaments. Stage III is highly unstable damage with severe dislocation. Stage III may be associated with damage to the cervical region of the spinal cord. This can be fatal. Survivors of this type of injury may suffer from neurological impairments, including lower cranial nerve deficits, unilateral or bilateral muscle deficiency, or even paralysis of all four limbs [ quadriplegia ].
FAQ
The most unique characteristic of this bone is a strong odontoid process, the dens. DEFINITION: The atlantooccipital joint consists of a pair of condyloid joints. The atlantooccipital joints are synovial socket type of joint and the sockets are superficial in babyhood and deepen with age.
As a result, the atlas is dislocated from the axis & compresses the spinal cord with a fatal result. Fractures of the dens produce about 40% of axis fractures. When the transverse ligaments of the atlas rupture the dens are set free resulting in atlantoaxial subluxation or incomplete dislocation of the medial-atlanto axial joint.
There are 2 joints unique to the cervical spine – the atlantoaxial (x3) and atlantooccipital joints (x2). The atlantoaxial joints are formed by the articulation between the atlas and the axis: Lateral atlantoaxial joints (x2) – are formed by the articulation between the inferior facets of the lateral groups of C1 & the superior aspects of C2.
The Traynelis category of atlantooccipital dislocations describes damages of the atlantooccipital joint according to the displacement of the occipital condyles comparative to the atlas: type II: longitudinal distraction (superior-inferior displacement).


One Comment