
Scapular Dyskinesia
Table of Contents
What is a Scapular dyskinesia?
- Scapular dyskinesia is an alteration of normal static or dynamic position or motion of the scapula during coupled scapulo-humeral movements that alter the scapulohumeral rhythm
- Scapular Dyskinesia is attributed to the loss of normal scapular mechanics, motion, and physiology. Scapular winging is a clinical observation where any part of the scapular departs excessively from the thorax soon after movement begins and persists in its disconnect trends throughout the arm movement. Scapular dyskinesia is considered an impairment with a causative origin
Cause of scapular dyskinesia
- 100% gleno humreal instabiity
- 60% rotator cuff pathology
- acromi clavicular separation
- labral injury
- clavicle fracture
- Weakness in scapular muscles, imbalance, tightness, or( infrequently) detachment of the muscles that control the scapula
- Injuries to the nerves that supply the muscles
- Injuries to the bone that support the scapula or injuries within the shoulder joint
Common signs and symptoms
Pain and or tenderness around the scapula when using the arm over the head or carrying heavy objects with the arm at the side.
Snapping or popping sensation around the scapula with shoulder movements
Loss of strength along with shoulder and arm use.
Asymmetrical posture(affected side generally sits lower)
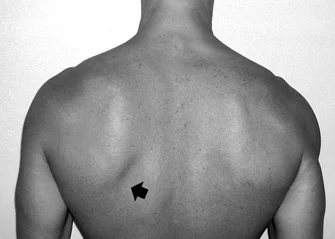
Winging of the scapula
Insecurity of the shoulder( feels like it moves out of place)
Scapula anatomy for scapular dyskinesia
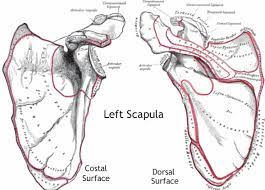
The scapula is a convoluted triangular bone on the posterior thoracic cage between the levels of the T2 vertebra and the T7 vertebra. It is composed of:
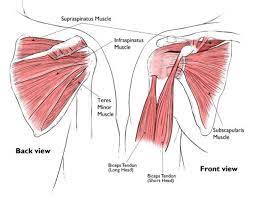
- The Anterior (costal) surface Has a concave surface that provides a bond for the subscapularis and the serratus anterior. The Coracoid process arises from the superior lateral anterior surface. This is a “finger-like” prominence where Pectoralis Minor, Biceps Brachi (Short Head), and Coracobrachialis attach. At the superior aspect of the anterior surface is attached to the Omohyoid bone, one of the strap muscles
- The Lateral surface consists of the glenoid fossa, the scapula portion of the glenohumeral joint. the Supraglenoid and Infraglenoid tubercles are also located which contribute attachment for the Long head of Biceps Brachii and Triceps Brachii, respectively
- The Posterior surface Consists of the boney structures of the spine, acromion, supraspinous fossa, and infraspinous fossa. The spine and acromion consist of the attachment of the trapezius and deltoid, although the supraspinous and infraspinous fossae serve as attachments for supraspinatus and infraspinatus, respectively. The inferior lateral posterior surface also contributes connection for Teres Minor, Teres Major, and Latissimus Dorsi
- The Medial Surface contributes bond for Levator Scapulae, Rhomboid Minor, and Rhomboid Major
- furthermore the various muscle attachments, there are two articulating joints. First is the acromioclavicular joint, promoted by the Trapezoid and Conoid ligaments connecting to the coracoid process and the acromioclavicular joint capsule which associate the acromioclavicular ligament. The clavicle serves three roles:
- Supports the arm, carries the humerus away from the thorax
- Protects the cervicoaxillary canal
- constitute as a means of force transfer from the core to the arm
- The second joint is the glenohumeral joint which is stabilized by four anterior ligaments, the superior, middle, and inferior glenohumeral ligaments, and the coracohumeral ligament. Posterior stability is approved by the posterior capsule.
- furthermore the articulating joints, there is the articulation between the scapula and thorax to recognize. Although no boney articulation appears, it is allowing a vast degree of “gliding” movement in a 3-dimensional plane. The role of the scapular and its muscular connections is to dynamically control the position of the glenoid to allow optimal biomechanical movement at the glenohumeral movement joint.
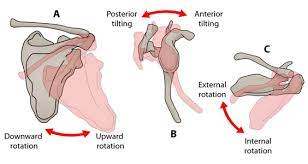
- Typical movement of the scapula appears in the sagittal, coronal, and transverse planes. The primary movements consist of two translations: superior/inferior, and protraction/ retraction, along with three rotations: upward/downward, internal/external, and anterior/posterior. Upward rotation is primary and posterior tilt is secondary during normal overhead UE elevation with internal/external rotation being minimal until 100°.
- A review of the normal ratio of glenohumeral (GH) to scapulothoracic (ST) motion under three-dimensional analysis found that the ratio of GH to ST motion changes from 7.3: 1 in the first 30° of elevation to 0.78: 1which is between 90 degrees and 150°. a ratio of 4.4:1 during the early phase and 1.7:1 within 80 to 140° of shoulder elevation.
- the SICK refers to the syndrome associated with scapular dyskinesia. “SICK” Scapula Syndrome is attributed to Scapular Malpositioning, Inferior medial border prominence, Coracoid process pain, malposition, and DysKinesia of the scapular movement. It’s an overuse Syndrome. The scapula is protracted and is in an anteriorly tilted position secondary to the tight pectoralis minor or short head of the biceps at the insertion to the coracoid process. the Coracoid process tenderness is an essential prediction of scapular dysfunction, which is secondary to constant traction from tightness at the tendon’s insertion. dysrhythmia is definite as initial or excessive scapular elevation, shrugging on arm elevation, rapid downward rotation during lower the arm, or a non-smooth or faltering motion during elevation, shrugging, and downward rotation actions.
Scapular biomechanics for scapular dyskinesia
- The scapula serves four biomechanical roles:
- It is the mid part of the rotation of the humerus.
- It is the mainstay of the humerus onto the thoracic wall.
- It keeps the acromion process from obstructing the movement of the humerus both in the abduction and in flexion, thus there is no impingement.
- It is aided by the forces transmitted from the core muscle to the arm.
- addicted to the scapula’s integral part of the upper arm’s kinematic chain, the scapular position and thus
- the glenoid position dictates the degrees of freedom within each plane of shoulder movement
- The scapular movement about humeral abduction and the reciprocal muscle routes that affect it.
- Elevation/Depression
- Protraction/retraction
- Internal/external rotation
- Superior/inferior rotation
- Anterior/posterior tilt
- Analysis of the fundamental shoulder movements of the shoulder, flexion, and abduction has been determined by a comprehensive appreciation of the movement stages involved. It is understood that for these movements to occur, the glenohumeral joint and the scapulothoracic articulation move in harmony. the first 30 degrees of flexion and 60 degrees of abduction of the humerus, the scapula explores to find a position of stability to optimize the power of flexion and abduction movements. In some cases, either the scapula would remain fixed with the glenohumeral joint being the principal area of movement or the scapula would translate medially or laterally to assist the glenohumeral motion. In the early degrees of movement, the movement of the scapula was person-specific, with variation seen. The optimal position that the scapula found was labeled the setting phase. Once flexion or abduction exceeded 30 degrees and 60 degrees levels, the behavior of the scapula was much more smooth, with a ratio of movement between the glenohumeral and scapulothoracic angle of 2:1, for an instant 15 degrees extension of the humerus, 10 degrees would exist at the glenohumeral joint, 5 degrees at the scapulothoracic.
- a less variable pattern of scapular movement, with the major factor being upward rotation, followed by posterior tilt and external rotation. the upper and lower trapezius along with the serratus anterior is the muscles that mostly affect scapular movement and cause dyskinesia. When the scapula biomechanics are considered in the anatomy of scapular dyskinesia, it becomes evident that the combination of movements, planes, and muscles includes there is a broad bundle of combinations that could lead to abnormal movement function
Classification of scapular dysfunction.
- Type I or Inferior dysfunction: The primary external visual feature is the prominence of the inferior angle as a result of the anterior tilting of the scapula in the sagittal plane. Inferior pattern appearance is better vocalized while in the hands-on-hips position or during eccentric lowering from overhead elevation. the Type 1 pattern is most commonly found in patients with rotator cuff dysfunction.
- Type 2 or Medial dysfunction: The primary external visual feature is the prominence of the entire medial scapular border due to the internal rotation of the scapula in the transverse plane. Type 1, the Type 2 scapular dysfunction becomes more evident in the hands-on-hips position and during active eccentric lowering from overhead. Medial pattern dysfunction most often happens in patients with glenohumeral joint instability.
- Type 3 or Superior dysfunction: identify by excessive and early elevation of the scapula during upper extremity elevation. This pattern has been attributed to compensatory shoulder hiking or shrug and is most often seen in patients with rotator cuff dysfunction and deltoid-rotator cuff force couple imbalances
Scapular pathophysiology for scapular dyskinesia
Shoulder-related causes of scapular dyskinesia
- Shoulder-related pathologies are the most common origin of the trouble. Almost all shoulder pathologies are accompanied by a degree of dyskinesia. The most common pathologies that are accomplished with some form of scapular dyskinesis are (1) acromioclavicular instability, (2) shoulder impingement, (3) rotator cuff injuries, (4) glenoid labrum injuries, (5) clavicle fracture and (6) nerve-related. The most common feature of all above mention pathologies is the disturbance of the scapulohumeral rhythm
- Shoulder impingement is accomplished with greater scapular protraction in the resting positions, greater posterior tilt during the abduction, and greater internal rotation during plane elevation. Furthermore, the scapula shows few upward rotations when the scapular plane is elevated.
- The scapula has a different achievement pattern in shoulder instability, with decreased rotation when the arm is elevated, but an increased internal circuit when the scapular plane is raised.
- In a frozen shoulder, the scapula externally rotates earlier at a greater degree compared to a normal scapula. But show that the increased mobility of the scapula is a redeeming structure
- the scapulohumeral rhythm can be assigned either by an inappropriate pattern of muscle activation too slow or too fast or an inappropriate force of muscle contraction too strong or too weak. Many muscles acting in different directions influence the scapula, and the timing and force of muscle activity dictate its movement.
- Fatigue is an important determinant of muscle performance. with elevating fatigue determinant the scapulohumeral rhythm is less effective. It would be delightful if the same experimental setup were extended to more convoluted activities, involving more muscles. 1) muscle fatigue following real-life movements, 2) which muscles were more susceptible to fatigue, and 3) if muscles assume dominance once the synergists are fatigued. Another muscle complication, like the stiffness of the latissimus dorsi, has been reported to affect the rotation of the scapula, pulling the bone superiorly
- The trapezius and the serratus anterior muscles have been associated with the development of dyskinesia in both shoulder impingement and shoulder instability. In impingement, the upper and lower trapezius along with the serratus anterior have altered their activation pattern, with the trapezius showing a greater strength of activation compared to the serratus anterior.
- Rotator cuff arthropathy promotes the elevated action from the rotator cuff muscles, supraspinatus, infraspinatus, and upper trapezius when compared to symptomatic patients
- The soft tissues that surround the shoulder have been associated with the development of diverse scapular mechanics. Namely, both pectoral muscles major and minor and the glenohumeral capsule have been clarified as important factors. The tightness of the muscles of the pectoral region encourages the anterior translation of the shoulder girdle and consequently the scapula. Furthermore, stiffness of the posterior aspect of the glenohumeral capsule shows a diverse resting scapular position, further anteriorly compared to normal individuals, a similar pattern to shoulder impingement
Diagnostic Procedures for scapular dyskinesia
Evaluate the presence or absence of dyskinesia
- classification of dysfunction Type 1, 2, or 3 or Scapular Dyskinesis Test. It is approved to perform forward flexion/arm elevation with maximum elevation 3-5 times to reproduce dyskinesia. If the examiner isn’t sure about the presence of dyskinesia a 3-5 pound weight is added to each hand and the examiner is asked to perform 10 reps of arm elevation in flexion Scapular dyskinesia is more detachable in the descent phase of arm motion, prominence of the medial border reveal a positive dyskinesia test.
Symptom-altering tests.

- Scapular retraction test’: This test examined the rotator cuff strength in scapular dyskinesia. Baseline active range of motion and pain are examined. if This test is positive the pain is decreased as the therapist assists active elevation by applying a posterior tilt and external rotation motion to the scapula. This function may be used with other tests such as Neer’s, Hawkin’s-Kennedy, and Jobe’s relocation.

- Scapular assistance test’: This test is used to evaluate scapular contributions to the extant shoulder pain depending on alterations in motion. The baseline AROM and pain are evaluated. The therapist then administers an assist to scapular dynamics. This test is positive if ROM is elevated or pain is decreased as the therapist manually assists upward scapular rotation during active upper extremity elevation.

- Lateral scapular Slide test (LSST): Measurements are taken from the spine of scapulae to T2 and T3 vertebra, the Inferior angle of scapulae to T7 toT9 vertebra, and the superior angle of scapulae to T2. The measurements are appropriated in 3 positions, (A) sitting/standing with arms resting on the side, (B) Hands on the waist, Thumbs Posteriorly (45 degrees abductions), (C) 90 degrees abduction, and maximal internal rotation. measurement should not alter more than 1 to 1.5 cm, more than the 1.5 cm difference is significant.
- Isometric Scapular Pinch test: The patient is in a standing position and is asked to actively by the patient squeeze or retract the scapulae together as hard as possible. Normal Response: An individual can hold the squeeze for 15 to 20 sec without burning pain or observable weakness. Positive: Burning pain present. examine for the patient relaxing the contraction.

- Scapular Load test: As in the position of the lateral scapular side test, Manual pressure is applied in the anterior, posterior, inferior, or superior direction to the arm, and the scapula should not locomote more than 1.5 cm.
- Wall pushup test: The patient performs the wall pushups test 15 to 20 times. Weakness of scapular muscles mainly serratus anterior or winging usually visible with 5 to 10 pushups. For stronger and younger people, perform the test on the floor.
Manual muscle testing
- Manual muscle test for the middle and lower trapezius manual resistance at 130-150 degrees and serratus anterior manual resistance of the arm at 130degrees of flexion
Pectoralis minor muscle tightness.
- Current measures examine manual muscle length at resting positions and identify a patient as having a tight pectoralis minor muscle.
Static Measurements
- Static measurements consist of (1) infraspinatus: difference in vertical height of the superomedial scapular angle of the dropped scapula co-related to the contralateral angle. (2) Lateral displacement: variation of superomedial scapular angle from the midline (3) abduction: variation in angular degrees of medial scapular margin from plumb line.
Core Evaluation
- The examiner stands behind the patient and asks the patient to contract the gluteal muscles while performing the low-row test. The patient is told to keep the shoulder extended and resist the anterior force offered by the therapist. If the strength of resistance the patient offers the therapist increases, it indicates that core and gluteal strengthening will aid scapular motion, and strengthening of the core is hence indicated.
Treatment of scapular dyskinesia
- Manual grade 4 mobilization to reduce posterior capsule tension, and cross-body stretch.
- Manual stretching and soft tissue mobilization to decrease pectoralis minor tension (cadaveric position imply a position of 150 degrees elevation with 30 degrees scapular retraction is optimal)
- Exercises of side-lying forward flexion, external rotation, prone extension, and prone horizontal abduction to strengthen the middle and lower trapezius over the upper trapezius.
- Quadruped position and variable push-up positions activate the serratus anterior
cross body stretch

- Use the unaffected arm to lift the affected arm at the elbow & bring the arm up and across the body,
- exert gentle pressure to stretch the shoulder.
- The cross-body stretch is held for 15 to 20 seconds.
- repeat this exercise 10 to 20 times per day.
quadruped position

Quadruped is the position where both the hands and the knees are on the floor. It is the starting position of crawling that all people quadruped help them develop curves in their spine and core strength.
Rehabilitation Protocol for scapular dyskinesia
Phase I flexibility
Soft tissue Release techniques
Pectoralis Release

- This technique interprets an arthroscopic release of the pectoralis minor tendon. The patient is positioned in the right lateral decubitus position, and the left arm is hanging in balanced traction. The right upper extremity is proceeded and covered to allow for medial access to the coracoid process
Posterior rotator cuff release

- Sitting or standing position, use the unaffected arm to lift the affected arm at the elbow and take it up and across the body. Press slightly, just above the elbow, to stretch the shoulder. clasp the stretch for 15 to 20 seconds.
Posterior capsule Release

put your hand onto that shoulder and then just roll around the back of that shoulder joint massaging into the back of the shoulder
Upper traps release

- stand facing the back of the wall put the knick ball to the level of the scapula and squeeze the ball as tight as you can
levator scapulae release

- Raise the right arm forwards and reach over the back of the head and apply downward pressure. This technique rotates the shoulder blade downward, which helps lengthen the levator scapulae muscle even more before it is stretched.
- Above mention, all techniques are Manual/self-release techniques
T-spine Mobility
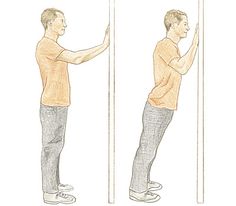
Thoracic Extension Roller & Bar
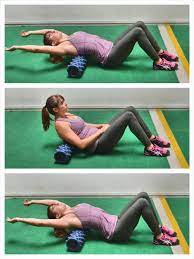
- This is a great drill to improve thoracic extension. To begin, set up a bar and roller on the floor. Place the roller on your thoracic spine then reach your arms overhead to grab the bar.
- There are two hand positions for this drill.
- The first one is hands positioned close together which will focus more on stretching the lats and teres major.
- The second variation is to place the hands wide which will focus more on stretching the pecs.
- When doing this drill it is very important to remember to breathe. Deep inhalations and exhalations will help you relax into the stretch.
- Aim to hold for 90 seconds for multiple sets.
Cat-Camel Drill

- This exercise is a great way to improve flexion and extension of the thoracic spine.
- Starting in the quadruped position, slowly move from a fully flexed position to a fully extended position.
- When doing this, it is important to inhale as you extend, and exhale as you flex.
- We recommend starting with 10-12 reps for multiple sets.
Deep Squat + Thoracic Rotation

- The deep squat with thoracic rotation is a more advanced drill that is a prerequisite for the overhead squat.
- There are two variations of this one The first one is done with no weight for reps, and the second is done with a light DB (2-3kgs) and held for a short time.
- The goal is to keep your hips in a deep squat position while you reach overhead with one arm. Start with 3 sets of 8 on each side.
Spiderman, Thoracic Rotation

- Spiderman with thoracic rotation is great for hip mobility and thoracic rotation.
- To begin the movement, start in a push-up position.
- The first step is to bring one leg outside your hand. In this position, you should feel a stretch on the hip flexors on the back leg and a stretch on the adductors on the front leg.
- The second step is to reach the sky with the hand, ensuring you rotate through your thoracic spine.
- Hold the top position for 3-5 seconds then swap sides.
- We recommend starting with 6-8 reps on each side for multiple sets.
Side-Lying Thoracic Windmill

- The side-lying windmill is a great exercise to improve thoracic extension and rotation.
- Lying on your side, start with your hip flexed at 90 degrees, resting your knee on a foam roller. Glide your top hand around your head with the goal being to get your arm to reach the floor on the opposite side.
- We recommend starting with 6-8 reps on each side for multiple sets
Sleeper’s stretch
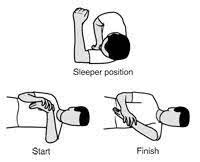
- Roll onto the involved shoulder. Place the elbow parallel to the shoulder. With the non-involved side, push the forearm down towards the floor. Hold for 30 seconds, 3 repetition
Genie Stretch

- Lean your right shoulder into a corner to assist in stabilizing the shoulder blade. Bring the left arm over the top of the right and reach for your elbow. Keeping your right shoulder blade down, gently pull your right arm across your body until you feel a slight stretch across the back of the shoulder.
Upper traps stretch

- Draw your head back, lining your ears up with your shoulders (a chin tuck position). Place one hand behind your back and place your other hand on your head and gently stretch your head away from the arm that is placed behind your back. Repeat 2-3 Times
- Hold 30 Seconds
- Complete 1 Set
- Perform 2 times per day
Isometrics for scapular dyskinesia
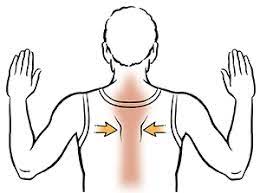
Scapular Pinches Stand up straight
- Raise each arm up to the side, bent at 90-degree angles with palms forward. Squeeze your shoulders back, pushing your shoulder blades toward each other. Hold for 5 seconds. Relax
Robbery Pinches

- Stand up straight with your feet hip-width apart.
- Keeping your back straight, bend your knees a little and hold your arms out in front with your palms facing your thighs.
- Straighten your knees and simultaneously bend your elbows, rotating your forearms upwards, facing your palms forwards.
- Squeeze your shoulder blades together as you do this.
- Repeat this movement.
- this exercise is also called “standing robbery with theraband”
- steps are the same as above just the elbow bent during exercise
Shoulder ER isometrics

- Bend your right arm in front of your body, palm up. Hold your right wrist with your left hand.
- Try to push your right arm outward, while pulling back with your left arm.
- Hold for 5 seconds
- Repeat 5 times.
- Repeat this exercise 3 times a day, or as instructed.
Scapular Depressor isometrics

- place the one-hand center of the scapula
- ask the patient to squeeze the shoulder blade
- 3 to 5 sec hold then relax
- repeat 5 to 10 times
Isotonics for scapular dyskinesia
Scapular Theraband exercise
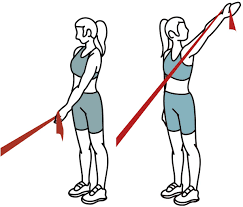
- patient position: standing
- attach a theraband to a solid object
- squeeze shoulder blades together and reach backward with the elbows, pulling the theraband toward you
- allow the theraband to retract forward again, but keep engaging the shoulder blade together
- reps 10 to 15 times
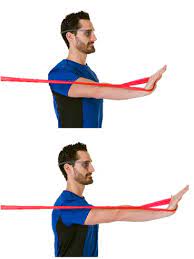
Shoulder ER in standing

- Hold the theraband between the hands with the elbows at an angle of 90-degree close to the sides.
- moves clockwise the lower part of the affected arm outward to two or three inches, and hold for five seconds.
- Repeat outward rotation 10 to 15 times, one time a day.
Shoulder IR in standing

- Stand close to the door and hook one end of the rubber exercise band around the doorknob.
- Hold the other end in the hand of the affected arm, and hold the elbow at an angle of 90-degree.
- Pull the theraband toward the body 2 or 3 inches and hold for 5 seconds.
- Repeat this exercise 10 to 15 times, one time a day
Dynamic Hug

- Abduction of your shoulders about 60° degrees and bend your elbows about 45°degrees. Keeping your arms elevated and in abduction position, push your arms forward and inward as if you were giving someone a hug. When your hands cross slowly in the middle, hold quickly and then slowly return to the starting position.
Scapular punches
- With the theraband in hand in line with arms straight and shoulder blade pulled back. Press out by pushing through the shoulder blade trying to drive the shoulder blade forward. Slowly let the shoulder blade back to starting position.
Phase II rehabilitation for scapular dyskinesia
Seated Rows
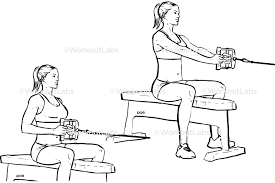
- Sit comfortably on the bench or plinth and plant flexion of your feet on the floor or foot pads, knees are in flexion. Extend the arms and grasp the handle or cable. Move your shoulders back and down. Brace your core muscles.
- blow out Bend your elbows to pull the handle or cable, keeping your elbows tucked in and your back neutral. Pause for 1 second.
- Inhale and gently extend your arms, counting to 3.
- finish one set of 12 to 15 reps
- this exercise is also called” low-row wall isometrics”
High Rows or lats pulldown

- Lift the chest upward and snatch the elbows back until the hands are right in front of the shoulders, then pause for 2-3 seconds. gently straighten the arms to return the weight to the starting position
Prone Rows

- To perform the prone rows, the patient begins the exercise laying face down with their throwing arm hanging straight towards the floor, holding an appropriate dumbell. Using a balanced pace, the patient raises the dumbbell to their chest, holds the position at the top for two seconds, and then gradually lowers the weight of the dumbell back to the starting position. Resistance is increased as strength develops.
Prone Y, I, T, and W
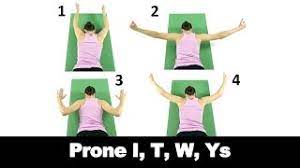
- position: face turn down on the floor with a towel under the forehead
- step1:engage the gluteal and abdominal muscles by drawing the belly button toward the spine
- step2:place the arm straight out to the side at a 90-degree angle with the body and thumb upward toward the ceiling
- step3:moves the shoulder blade down and backward, elevate the arm off the floor, and hold for 3 count
- step4:proceed to elevate the arm at progressive levels, resembling letters “y” and “l”, before bending the elbow, bring the arm sideways to make “w”
- step5:hold all four positions for 3 counts with the thumb pointed up toward the ceiling
- step6:reset the gluteal, abdominals, and shoulder blades muscles and repeat again
- reps:3 to 5 times
- sets:2 to 3
- frequency:3 to 5 times per week
Lawnmower/Standing D2 Cocking with theraband or dumbells

- put one end of the theraband below the sole of the foot
- another end of the theraband clasp in the opposite hand
- snatch the theraband with your hand as high as you can
- hold 5 second
- reps 10 to 15 times
Side-lying ER with dumbell
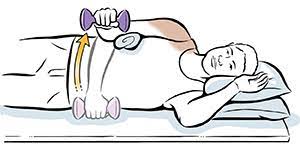
- The moving arm begins at the side of the body with the elbow bent to 90 degrees. While keeping the elbow of the moving arm fixed to their sideline, the patient externally rotates their shoulder, holds the rotated position for two seconds, and then slowly lowers the arm to the starting position
PNF D1/D2 pattern of upper extremity
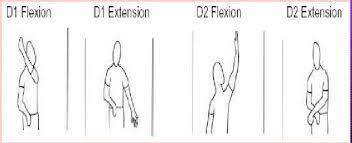
- The D1 shoulder flexion pattern starts with shoulder flexion, adduction and internal rotation, forearm supination, wrist flexion, and finger flexion. The anteposition for D1 flexion is shoulder extension, abduction, external rotation, forearm pronation, wrist, and finger extension.
- D2 flexion starting position shoulder flexion, abduction and external rotation, forearm supination, wrist, and finger extension.
- D2 extension includes shoulder extension,adduction,internal rotation,forearm supination,wrist and finger flexion
Scapular clocks
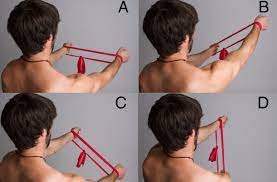
- start by placing both hands on the wall in front of the shoulder with the arm straight, wrist extended with the theraband of appropriate resistance around the wrist retract and depressed the scapula then move your arm in a different position on an imaginary clock on the wall such as 3 o’clock,2 o’clock,4 o’clock
- make sure that always keep tension in the theraband
Wall washes
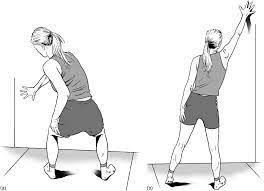
- Start by placing your hand up on top of or up against a wall above head height and then only moving your hands the shoulder blade rotates only so that it goes down
- 10 to 15 reps
Phase III Closed kinematic chain exercises and advanced exercises.
Standing cable column punches

- Hold the cable with one hand and get into a boxing-style dot while using the cable as resistance throw the proper touch dot. Return back to your starting position.
Seated Pike lift

- Sit on the floor on a mat with your legs extended in front of the wall.put your feet on the floor
- Keep your legs straight, lock your knees, and point your toes out in front of you. Put your hands on the mat or floor, approximately in line with your knees.
- Engage your core muscle and lift Keeping your back straight and near vertical, legs straight, knees locked, and toes extended forward, slowly lift your legs and tap your heels together. raise your feet until they’re about 10 cm, or 4 inches, off the floor.
- Lower, With your core muscle still engaged, bring your heels apart and slowly lower your feet back down to the floor. Make sure to maintain that same position from the back, knees, and toes.
- repeat 10 to 15 times
Push Plus/Scapular Pushups

- Standing or prone straight facing the wall and put your hands on the wall. Align the hands on your chest and shoulder width apart.
- Keep the arms fastened out and palms level on the wall.
- Without buckling your arms, reach with your sternum towards the wall until both shoulder bones return together in the back.
- Passing over two hands coordinately, shift the sternum away from the wall until both scapulae open up and your upper back is somewhat adjusted; at that point, reuse.
Standing Snow Angels

- Hold a theraband at each hand end overhead with arms straight. Squeeze the shoulder blades together forcefully and keep the shoulder blade retracted throughout the movement. At a controlled temperature lower the arms straight down so the band slides down the back, then reverse the motion.
Wall ball Scours

- Bend your legs and drop your butt down so that your legs form a 90-degree angle. shift your weight down through your heels and explode your weight upwards, throwing the ball up and against the wall. speedily catch the ball, then drop back down and repeat the squat movement. Perform 5 sets of 10 repetitions
FAQS
- How long does scapular Dyskinesia take to fix?
Most abnormalities in the scapular movement or scapular position can be improved through rehabilitation exercises, often with a physical therapist or athletic trainer. Generally, therapy may last anywhere from 4-8 weeks depending on the severity of the injury
- How do you improve scapular Dyskinesia?
SIDE-LYING SCAPTION RAISE. Laying on one side, start with the top arm 30 degrees in front of the hip.
SHOULDER SCAPTION
QUADRUPED ALTERNATE ARM
ELBOW KNEE PLANK. - Can scapular Dyskinesia cause neck pain?
scapular dyskinesia may greatly affect the neck and contribute to neck pain, shoulder pain, headaches, upper cervical laxity, and even thoracic outlet syndrome.
- How can scapular Dyskinesia be prevented?
You can prevent scapular dyskinesia by Stretching and warming up before throwing or completing any overhead activities
- How rare is scapular Dyskinesia?
Scapular dyskinesia or alterations in dynamic scapular control is present in as many as 67% to 100% of athletes with shoulder injuries. However, it is also present in many asymptomatic individuals.




One Comment