Mannerfelt Syndrome
Table of Contents
What is a Mannefelt Syndrome?
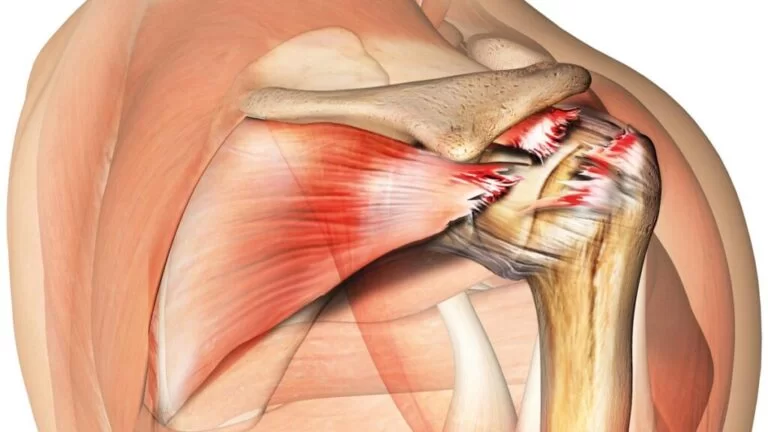
- Mannerfelt’s syndrome is caused by a rupture of the pollicis longus tendon due to a bone spur in the carpal tunnel.
- These carpal tunnel base tears have also been reported in rheumatoid arthritis.
- The tendon of the flexor pollicis longus is most often torn and Mannerfelt named this injury. Hence the name Mannerfelt syndrome. Failure of process in Mannerfelt syndrome is not specific.
- When the tendon of the long flexor of the wrist is torn, it has continuity with the peritoneal sheath or pseudorandom.
- The individual usually has little or no flexion of the distal phalanx.
- Flexor tendon tears occur toward the ulna, affecting the flexor tendon and the flexor tendons. Surgery is usually a treatment option.
Flexor pollicis longus anatomy
Rests on the lateral side of the flexor digitorum profundus
Origin:
- Arises from the anterior surface of the radius between the radial tuberosity above and the pronator quadratus below and adjacent to the anterior surface of the coronoid process of the ulna the fibers run almost to the wrist before the tendon is formed the tendon passes under the flexor retinaculum
Insertion
- palmar/volar exterior of the base of the distal phalanx of the thumb
Action
- flexor of the interphalangeal joint of the thumb important in all hand-grabbing actions also flexes the thumb at the metacarpophalangeal joint and carpal joint
Pulley system in hand
- The pulley system is an important anatomical structure when dealing with the tendon system of the hand.
- The function of the ring pulley system is to keep the tendons close to the bone so that the tendons do not bow during active flexion.
- The cruciform pulley system is flexible and foldable to allow digital bending without deforming the pulley system.
- This should be kept in mind when treating people who have undergone tendon repair, as sometimes patients may experience spring pain after tendon repair.
- Knowing the anatomy and function of the pulley system helps therapists think about its clinical cause is happening
Mechanism of injury
- Flexor tendon injuries usually result from volar/palmar tears.
- It can occur with accompanying neurovascular disease too bad patients often go straight to the hospital because they are likely to have suffered a serious injury.
- Another mechanism of injury is a tear rather than a tear, for example, the FPL tendon is torn from its position.
Distal phalanx –
- Usually due to a closed mechanism of injury.
- This usually occurs as a result of a forced extension during active flexion.
- This occurs in ball sports where the finger is forced to extend when it is bent or where the player grabs the opponent’s shirt (shirt finger) or in an activity such as rock climbing.
What is the cause of Mannerfelt syndrome?
- In rheumatoid arthritis, the ligaments between the carpal bones lose their strength, causing the carpal flexors to exert constant traction, resulting in voluntary subluxation of the carpal bone.
- Destructive rheumatoid arthritis follows nutrient vessels, resulting in erosion of the distal volar vessel and proximal volar trapezium.
- Erosions between the bony tissues create sharp bones that further cool the carpal tunnel floor and cause flexor tendon friction.
- Tendon support causes rupture of the tendon of the flexor pollicis procumbens.
- The most common tear sites are the dorsum, trapezius, distal ulna, hamate, lunate, distal radius, and sesamoid of the ulna.
What is the prognosis of Mannerfelt syndrome?
- The prognosis was assessed in subjects who underwent index finger flexor digitorum sublimis grafting to repair irreparable damage to the flexor pollicis longus tendon.
- If the movement of the interphalangeal joints is restored, the prognosis is considered good.
- Difficulties are tiniest, although rupture of the tendon reconstruction or interphalangeal fusion can happen.
What are the symptoms of Mannerfelt syndrome?
- People with Mannerfelt syndrome often have rheumatoid arthritis.
- The tendon of the long flexor pollicis is the only muscle that flexes the interphalangeal joint of the thumb; therefore, a Mannerfelt lesion is easily detected during a physical examination.
- If a healthcare provider stabilizes the interphalangeal joint and asks the person to flex the interphalangeal joint, it means a tear if the person is unable to flex the joint.
- The clinical symptoms of flexor pollicis longus tendon rupture and incomplete anterior intercostal nerve palsy are similar. A simple test can distinguish it.
- A healthcare provider dorsiflexes a person’s wrist.
- The thumb is hyperextended at the metacarpophalangeal joint and the carpal and wrist joints.
- If the flexor longus tendon is paralyzed but intact, the interphalangeal joint flexes spontaneously and tolerates passive stretching on examination.
- The interphalangeal common remains extended; this indicates a rupture of the tendon of the long flexor pollicis.
Diagnostic procedures
- Flexor Pollicis Longus tendon – flexes the interphalangeal (IP) joint of the thumb separately.
- X-rays – may involve a fracture
- Ultrasound – used to assess suspected injuries
- MRI
Outcome measures
- Pressure force
- Dash
- Goniometric measurement
Treatment of Mannerfelt syndrome
Treatment includes:
Medical management:
- Inflamed tenosynovium has been medically treated to reduce pain and cap formation and the risk of tendon rupture.
- If the lesion is detected, the treatment is surgery.
Surgical treatment:
- Before starting the operation, the person is told about the possibility that some construction techniques can be used and the operation does not cure the underlying disease, for example, rheumatoid arthritis.
- In addition, the person is told that tenosynovitis and tears may recur.
- An unidentified Mannerfelt lesion is cured with the division of the transverse ligament of rheumatoid arthritis.
- After exploration, the bony spur on the floor of the carpal tunnel is excised, followed by a total flexor tenosynovectomy.
- Carpal tunnel has been studied extensively and tendon repair prevents future tears.
- A bone spur rubbing against the tendon of the flexor pollicis longus can also affect the rest of the tendons; therefore, a thorough examination of the carpal tunnel is recommended in individuals with a fused interphalangeal joint.
- Tendon reconstruction and repair are recommended in functional interphalangeal joints.
- A tendon graft or graft is performed when the distal end of the tendon is outside the wrist and cannot be returned to the injury.
- A tendon transfer is also performed in the nonfunctioning flexor pollicis longus muscle.
- Tendon fusion is a treatment for an arthritic or unstable thumb interphalangeal joint.
- A linear incision is made in the proximal palm over the fourth ray and extended in a zigzag pattern over the wrist.
- The central nerve and its branches (cutaneous palmar and motor) are avoided.
- The bone spur is cut away and the adjacent soft tissue is mobilized to cover the exposed bone. The damage can be covered by:
- Silicone film.
- Transverse palm flap.
- Tendon transplantation.
- Short pons tendon graft.
- Conventional full-length tendon graft.
Tendon transfer.
- After the wound is closed, the wrist is held at 15-20 degrees of flexion and the thumb at 30 degrees of palmar flexion.
- After six weeks, a back brace is applied and the removable suture is removed.
- Tendon transposition occurs in the nonfunctional tendon of flexor pollicis procumbens.
- A tendon graft has only one attachment point compared to a tendon graft.
Other benefits of tendon transfer include:
- Gives a more workable tendon.
- Transplantation of the graft does not require an additional procedure.
- Provides mobility in flexor wrist prolapse tendon injury.
Postoperative tendon healing
The stages of tendon healing include 3 stages:
Inflammatory phase
- First phase
- lasts from the first to seven days after surgery
- in this step, fibroblasts produce type III collagen, and macrophages support initiate healing and remodeling
Proliferative phase
- This is the second step
- It lasts from the 8th day to about three weeks after surgery
- In this stage, tissue modeling occurs using a large amount of degraded collagen angiogenesis also occurs at this stage
Transformational phase
- This is the third step that occurs approximately 18 months after surgery.
- At this stage, tensile forces lead to tissue regeneration, and type III collagen is replaced by type I collagen it happens more linearly and creates a bond to increase the strength of the tendon.
Management of postoperative physical therapy
- Therapists must know anatomy, pulleys, areas of tendon damage, and the stages of tendon healing, as this tells me about the treatment method.
- For example, the area? tendon injury determines the splint design and treatment.
- The time and phase of tendon healing affect the rehabilitation exercises initiated.
- For example, if the patient is sent for treatment 8 or 9 days after surgery and the patient has not yet received treatment, the therapist probably did not want to start active range of motion exercises because the tendons are at their weakest between days 8 and 21 after surgery.
- Therapists must also be aware of the importance of the flexor mechanism in the functional use of the arm and how the flexor mechanism. tendon damage can affect the patient’s functioning.
Treatment of wounds and scars
- After surgery, wound care is the first step that must be addressed.
- The postoperative wound can be covered with a basic silicone dressing (products such as Mepitel can be used).
- The finger is surrounded by breathable, convenient gauze.
- Another product therapists may utilize is Coban, but a suitable, comfortable, clean, dry bandage is also acceptable.
- Compression bandages are used to control swelling.
- Once the wound has healed, scar treatment can begin.
- Silicone gel film can be used for scars or paper tapes
Scar treatment
- Products such as Fixomull. Scar massage can be done during therapy sessions and as a preventive measure at home adhesions.
Rehabilitation exercises
- The goal of rehabilitation exercise after flexor tendon repair is to keep tendons gliding and promote differential tendon gliding controls early deposition of collagen making it easy to repair the repair shop to prevent adhesions, tent tears, or recurrence to provide patients with the best possible outcome after surgery.
- Various protocols have been developed for flexor tendon rehabilitation. These programs typically use a combination of active and passive movement duration.
Post-Operative Training– FPL Repair (first 6 weeks)
- Passive IP joint flexion exercises
- Passive thumb compound flexion
- Active flexion to approximately half of the patient’s active range of motion
- 10 repetitions, 5 times a day
Post-operative exercises after 6 weeks
- In all postoperative tendon repairs – splints are used for 6 weeks
- After the first 6 weeks, the patient is weaned from the splint to begin light functional use slowly increase and assess the patient’s fully active and passive range of motion Strengthening can usually begin about 8 weeks after surgery.
- Strengthening exercises can include e.g.
- Press the Theraputty, Play-doh or sponge into the hot water
- May progress to wrist weights and, if necessary, Therabandin for full upper extremity strengthening
- Once the patient can return to leisure activities, can use the arm functionally with minimal limitations, and pain is controlled, the patient can be discharged home with a home program of continued stretching, scar care, and strengthening exercises.
Complications
Some of the complications that therapists must consider when treating patients with flexor tendon injuries include:
Rupture
- Beware of rupture, especially during the first course of the six-week loading period. Signs of a tendon tear may include:
- FDP Tendon – The patient may show signs of active flexion of the DIP joint when the joint is isolated
- FDS Tendon Repair – If the PIP is isolated, the patient may not have active PIP joint flexion
- FPL Tendon Repair – The patient may not have isolated IP joint flexion
- If you are concerned about a patient who may have a tendon rupture, it is important to contact your surgeon immediately.
An infection
There is always a risk of infection during surgery, and it is important to contact the surgeon if signs of infection appear. Signs of inflammation you should pay attention to:
- Redness in and around the wound
- The presence of purulent or cloudy wound drainage
- An increase in temperature around the wound or a fever
- A foul smell comes from the wound
Contractures
- It may occur who undergone FDS and FDP tendon repair
- If a patient develops a contracture, they sometimes need a dynamic splint around 8-10 weeks after surgery.
- It is important that patients perform exercises in the back block splint and actively encourage stretching, especially in the posterior aspect of the PIP joint splint, to prevent contractures during the first 6 weeks.
- It also prevents flexor adhesions and PIP joint contracture.
Scar Adhesions
- Scar adhesions can limit the active and passive range of motion of the patient’s flexor arch and finger, as well as flexion and extension.
- It is important to massage the scar as much as possible and allow the skin to slide freely from the underlying tendons.
- It is important to prevent infection first.
- If significant adhesions are found and proven, patients may require tenolysis or tendinopathy.
Loss of sensation
Sometimes patients have minimal nerve damage at the time of injury that does not require surgical repair, but develop symptoms of nerve damage within six weeks. These symptoms include:
- Numbness, tingling, or tingling in the affected finger
- It is important to discuss these signs and symptoms with your surgeon, as additional surgery may be necessary if the nerve is damaged and cannot be repaired conservatively.
Patient Education
- Patient education is very important in the treatment of flexor tendon injuries.
- Patients should be aware of the necessary precautions.
- The wound should be maintained neat and dry.
- The splint must remain in place 24 hours a day, 7 days a week.
- If the splint needs to be removed, the patient should be instructed in safe hand positions.
- Because of impaired flexibility, the patient must keep the fingers covered and the wrist in a neutral position when the splint is loose.
- This position does not cause any stretching or tension in the tendons.
- Treatment sessions are generally twice a week for the 1st two weeks after surgery. After that, weekly sessions until about 10 weeks after surgery.
FAQs
Rheumatoid arthritis flexor tendon tears are caused either by wear of bone spurs or by direct penetration of hypertrophic tenosynovium into the tendon. All friction tears occur in the carpal tunnel and are the most common cause of tendon tears.
It takes about 3-4 months for the flexor tendon to heal before your arm is strong enough to use without restrictions. you will usually need to wear a splint for about 6-8 weeks after surgery and it will only be removed for exercise as prescribed by your doctor and therapist.
Unlike all kinds of connective tissue, tendons are adept at self-healing, but numerous factors play an essential role in tissue repair and healing. Unlike muscles, tendons generally have moderately insufficient blood flow, which is a very significant element in the healing and healing process.
Vitamin C (VC) has been described as important in tendon and ligament healing mainly due to its antioxidant properties and role as a cofactor in collagen synthesis.
Vitamin C plays an important role in the production of new collagen, and vitamin C deficiency can weaken your tendons and ligaments by inhibiting the synthesis of collagen.