

Peripheral Artery Disease
Table of Contents
What is Peripheral Artery Disease?
Peripheral artery disease (PAD) is characterized by abnormal constriction of arteries that don’t supply the heart or brain. Peripheral artery disease can occur in any blood vessel, but it develops more commonly in the legs than in the arms.
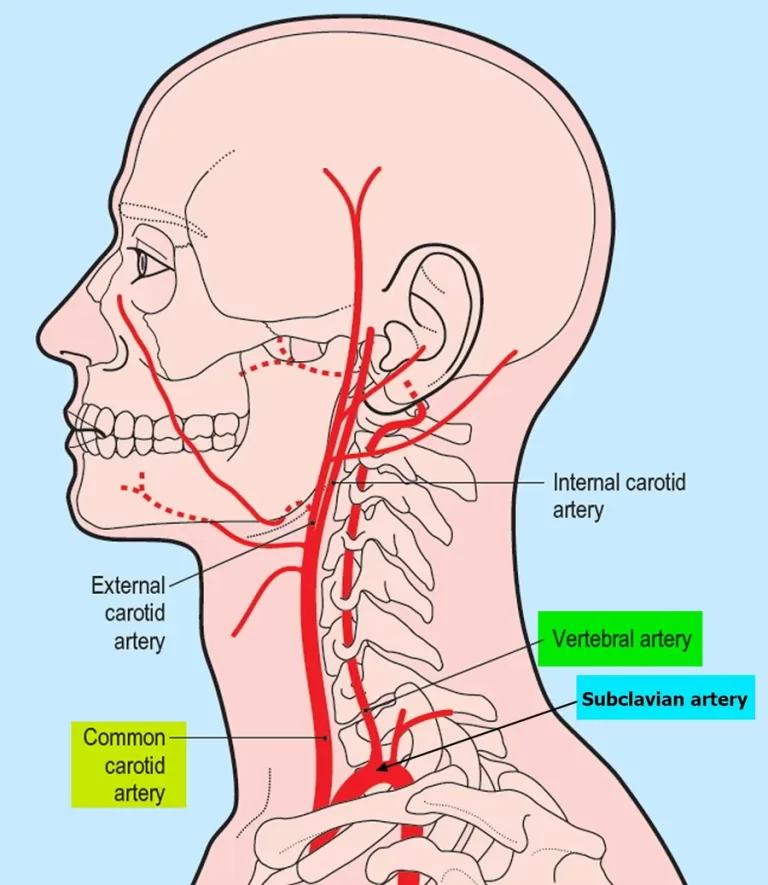
Heart artery narrowing is known as coronary artery disease (CAD), and brain artery narrowing is known as cerebrovascular disease. Although peripheral artery disease most frequently affects the legs, other arteries, including those in the arms, neck, and kidneys, may also be affected.
Peripheral Vascular Disease is a form of peripheral artery disease. The term “vascular” refers to both the arteries and veins in the body. Peripheral artery disease is different from peripheral vein disease. Peripheral Vascular Disease indicates that the arteries, which transport oxygen-rich blood from the heart to other areas of the body, are restricted or blocked. Peripheral venous disease, on the other hand, refers to problems with veins, which are the blood channels that return blood to the heart.
Walking-related leg pain that goes away with rest is the common symptom, also known as intermittent claudication. Other signs include skin ulcers, bluish skin, cold skin, or unusual nail and hair growth in the affected leg. Complications may include infection or tissue death, which may necessitate amputation; coronary artery disease, or stroke. Up to 50% of peripheral artery disease patients have no symptoms.
Cigarette smoking is the most dangerous risk factor for peripheral artery disease. Other risk factors include kidney issues, diabetes, high blood pressure, and high cholesterol. Peripheral artery disease is mostly caused by the formation of fatty plaque in the arteries, known as atherosclerosis, especially in people over the age of 40. Atherosclerosis, blood clots, trauma, fibromuscular dysplasia, and vasculitis are some of the other steps. An ankle-brachial index less than 0.90, which is the systolic blood pressure at the ankle divided by the systolic blood pressure in the arm, is commonly used to diagnose peripheral artery disease. Angiography and duplex ultrasonography may also be used. Angiography is more accurate and allows for immediate therapy; yet, it is accompanied by higher risks.
Screening for peripheral artery disease in patients who do not have symptoms is not clear because it has not been completely investigated. Stopping smoking and supervised exercise therapy may improve results in people with intermittent claudication caused by peripheral artery disease. Medications such as statins, ACE inhibitors, and cilostazol may also be beneficial. Aspirin, which aids in blood thinning and thus improves blood flow, does not appear to benefit people with moderate disease but is usually suggested for those with more severe disease due to an increased risk of heart attacks. Peripheral artery disease is treated surgically with bypass grafting, angioplasty, and atherectomy.
In 2015, around 155 million people globally had peripheral artery disease. It becomes more common as you become older. It affects 4.6% of people between the ages of 45 and 50 and 15% of adults between the ages of 85 and 90 in developing countries. Peripheral artery disease affects men and women equally in the industrialized world, but women are more typically impacted in developing nations. Peripheral artery disease caused around 52,500 death in 2015, an increase from 16,000 deaths in 1990.
What are the Signs and Symptoms of Peripheral Artery Disease?
The signs and symptoms of peripheral artery disease are dependent on the part of the body that is affected. About 66% of patients affected by peripheral artery disease either do not have symptoms or have unusual symptoms. Intermittent claudication (IC), which commonly refers to lower extremity skeletal muscle soreness during exercise, is the most typical sign. IC presents when there is a poor oxygen supply to connect the metabolic requirements of the skeletal muscles. IC is a common indication of peripheral arterial disease. The pain is usually located in the calf muscles in the affected leg and is relaxed by rest. This occurs because during exercise the muscles require extra oxygen. Usually, the arteries would be able to increase the amount of blood flow and therefore increase the amount of oxygen going to them when they are working out. However, in peripheral artery disease, the artery is unable to respond appropriately to the increased demand for oxygen from the muscles and as a result, the muscles are poor of oxygen due to the pain of the power that goes away with rest.
- Other symptoms:
- Pain, aches, or cramps in the buttocks, leg, or thigh
- Muscle atrophy (muscle loss) of the affected lower limb
- Loss of hair on the affected limb
- When touched, the skin in the affected area feels cool, smooth, or shiny.
- Reduced or absent pulse in feet
- Cold or numbness in the toes
- Wounds or ulcers on the affected limb that do not heal
Complications, such as critical limb ischemia and gangrene, can develop in those with severe peripheral artery disease. Critical limb ischemia happens when the artery’s blood flow restriction becomes so severe that the blood is unable to maintain the tissue’s rest oxygenation levels stable. This may result in numbness or tingling in the foot and toes, as well as pain that increases with rest. The loss of tissue in the lower limbs (amputation), ulcers caused by vascular insufficiency, erectile dysfunction, and gangrene are further effects of severe peripheral artery disease. Compared to the general population, those with diabetes get foot gangrene at an incidence that is 30 times greater. A large number of these serious effects, including those that result in amputation, are permanent.
What are the Causes of Peripheral Artery Disease?
Smoking – The single highest risk factor for peripheral artery disease worldwide is tobacco smoking, in any form. According to a dose-response association, smokers have a risk of PAD that is up to 10 times higher. It has also been demonstrated that secondhand smoke exposure causes changes in the endothelium, the lining of blood vessels, which can result in atherosclerosis. Lower extremity peripheral artery disease is 2-3 times as common in smokers than coronary artery disease. More than 80%–90% of patients with peripheral vascular disease of the lower extremities are either current or former smokers. As cigarettes are smoked more frequently and for longer periods of time, the risk of peripheral artery disease increases.
High blood sugar – There is evidence that diabetes mellitus doubles or triples the risk of peripheral artery disease. In peripheral arteries, it accomplishes this by decreasing endothelial and smooth muscle cell activity. The severity and length of diabetes are directly correlated with the risk of developing lower extremities peripheral arterial disease.
High blood cholesterol – An uncommonly high quantity of cholesterol or fat in the blood is known as dyslipidemia. High levels of the protein known as low-density lipoprotein (LDL cholesterol), low levels of the protein known as high-density lipoprotein (HDL cholesterol), an increase in total cholesterol, and/or high triglyceride levels are the causes of dyslipidemia. Accelerated peripheral arterial disease has been linked to this abnormality in blood cholesterol levels. A significant decrease in the incidence of heart attack and stroke is related to the management of dyslipidemia with diet, exercise, and medication.
High blood pressure – An individual’s risk of having peripheral artery disease may rise due to hypertension or increased blood pressure. High blood pressure is also known to increase the risk of heart attacks, strokes, and abdominal aortic aneurysms, similar to peripheral artery disease. Intermittent claudication, the most common sign of peripheral artery disease, is 2.5- to 4-fold higher in males than in women who had high blood pressure.
Levels of multiple inflammatory mediators like C-reactive protein, fibrinogen, homocysteine, and lipoprotein A are among the other risk factors being researched. Peripheral artery disease is twice as likely to affect people whose blood homocysteine levels are higher. No specific genes or gene mutations have been directly linked to the onset of peripheral artery disease, but the genetics of risk factors for the condition, such as diabetes and high blood pressure.
Pathophysiology of Peripheral Artery Disease?
The pathophysiology of atherosclerosis interacts in a complicated way between cholesterol and vascular cells. In the early stages of peripheral artery disease, the arteries enlarge to cover up the plaque buildup and maintain blood flow. When the artery reaches its maximum dilation, the atherosclerotic plaque begins to narrow the arterial flow lumen.
Ischemia (limitation of blood flow) to the lower limbs might be functional or critical depending on the pathophysiologic perspective. Functional ischemia appears clinically as intermittent claudication when blood flow is normal at rest but insufficient during exercise. Critical ischemia is characterized by the appearance of pain at rest or trophic lesions in the legs and is created when the decline in blood flow leads to a perfusion deficit at rest. If sufficient blood flow is not restored, either through surgery or endovascular therapy, an actual possibility of losing the limb is present, also an accurate diagnosis is critical in this situation. It’s crucial to differentiate between the two ideas in order to determine the treatment indication and the prognosis in patients with peripheral artery disease.
Other reasons include in situ thrombosis associated with hypercoagulable conditions and vasculitis. arterial spasm and fibromuscular dysplasia are additional mechanisms of peripheral artery disease. While the mechanism and causation of arterial spasms are not fully known, it has been suggested that trauma can be a secondary cause. When the artery spasms or clamps down on itself, obstructing blood flow, claudication symptoms develop. This results in less blood flowing to the tissue downstream of the obstruction, similar to atherosclerosis. Blood clots, or thrombosis, commonly form as a result of trauma or stasis.
What is the Classification of Peripheral Artery Disease?
The Fontaine and Rutherford systems of classification are the two approaches that are most frequently used to categorize peripheral artery disease.
Rene Fontaine developed the Fontaine phases in 1954 to categorize the severity of chronic limb ischemia:
- Stage I: asymptomatic
- Stage IIa: Intermittent claudication after more than 200 meters of walking
- Stage IIb: intermittent claudication after a walk of fewer than 200 meters
- Stage III: rest pain
- Stage IV: ulcers or gangrene of the limb
The Society for Vascular Surgery and the International Society of Cardiovascular Surgery developed the Rutherford classification, which was first used in 1986 and modified in 1997. There are four grades and seven categories (0–6) in this classification structure.
- Grade 0, Category 0: asymptomatic
- Grade I, Category 1: mild claudication
- Grade I, Category 2: moderate claudication
- Grade I, Category 3: severe claudication
- Grade II, Category 4: rest pain
- Grade III, Category 5: minor tissue loss; ischemia ulceration does not extend to the ulcer of the digits of the foot
- Grade IV, Category 6: major tissue loss; extensive ischemia ulceration or frank gangrene
How Is Peripheral Artery Disease Diagnosed?
For the diagnosis or identification of peripheral artery disease, a physical examination, a history of symptoms, and confirmation testing are required. These evaluations may include ultrasonic imaging, magnetic resonance angiography (MRA) scans, or computed tomography (CT) scans. A doctor will next perform particular exam findings on a patient if they exhibit signs of peripheral artery disease. If a medical professional discovers abnormal physical exam results, they may assess a specific diagnosis. However, confirmation testing is necessary in order to verify a diagnosis.
The following findings indicate a correlation to peripheral artery disease:
- Reduced or absent pulses
- Muscle atrophy or loss
- Blueness of the affected limb
- Compared to the other limb, the affected limb has a lower temperature (feels cooler)
- Thicker nails
- Hair loss and skin that is bright or smooth
- When the injured limb is lifted, Buerger’s test can identify pallor. The limb is then shifted from the elevated position to a sitting posture and examined for reactive hyperemia, which is characterized by redness. The Buerger’s test evaluates arterial sufficiency, or the artery’s capacity to provide oxygenated blood to the tissue it supplies.
- Nonhealing lower limb wound
Ankle-brachial index (ABI) testing is the first step in the diagnosis of peripheral vascular disease. The ABI is a quick, non-invasive test that measures how much higher the ankle’s systolic blood pressure is compared to the upper arm’s. This is based on the theory that a blockage in the arteries supplying blood from the heart to the ankle is suspected if blood pressure readings in the ankle are lower than those in the arm. ABIs between 0.90 and 1.40 are regarded as normal. If an individual’s ABI is less than 0.90, they are diagnosed with peripheral artery disease. However, if the ABI is between 0.41 to 0.90, peripheral artery disease is classed as mild to moderate, and less than 0.40, it is classified as severe. These groups may provide information on how an illness develops. ABI results between 0.91 and 0.99 are considered borderline, whereas values more than 1.40 suggest noncompressible arteries. Calculating an ABI greater than 1.40 may reveal calcification-induced stiffness of the vessel wall, which can happen in persons with uncontrolled diabetes.
Patients with suspected peripheral artery disease and normal ABIs can test their ABIs during exercise. Prior to exercising, a baseline ABI is collected. Following this, the patient is instructed to walk on a treadmill at a steady speed for up to five minutes or until claudication pain appears at which point the ankle pressure is once more measured. An ABI decline of 15%–20% would indicate peripheral artery disease.
If the ABIs are abnormal, a lower limb Doppler ultrasonography is usually performed to assess the location of the obstruction and the degree of atherosclerosis. Further imaging can be performed using angiography, which includes placing a catheter into the common femoral artery and carefully guiding it to the target artery. An X-ray is taken while a radio-dense contrast chemical is injected. Procedures like atherectomy, angioplasty, or stenting can be used to identify and cure any blockage that restricts blood flow that was seen on the X-ray. The imaging procedure that is the most accessible and popular is contrast angiography. Using computerized tomography (CT) scanners, the vascular system can be directly imaged nowadays. According to studies, CT has 95% and 96% sensitivity and specificity for identifying lesions with more than 50% stenosis.
Magnetic resonance angiography (MRA) is a noninvasive diagnostic procedure that uses a combination of a huge magnet, radio waves, and a computer to produce detailed images of blood vessels inside the body. The benefits of MRA include its safety and capacity to provide full three-dimensional high-resolution imaging of the abdomen, pelvis, and lower extremities in a single sitting.
Medical Treatment Of Peripheral Artery Disease:
Cilostazol is a medicine that is used to treat the symptoms of intermittent claudication in patients with peripheral vascular disease. Pentoxifylline is a xanthine derivative that is used to treat muscle pain in people suffering from peripheral artery disease.
Revascularization:
- Patients may be provided to a vascular or endovascular surgeon if their symptoms continue. Revascularization has been shown to be beneficial in proportion to the severity of the ischemia and the presence of other risk factors for limb loss, such as the severity of the wound and infection.
- Angioplasty restores blood flow to the limb immediately. Which procedure is ideal for you is determined by the severity of your obstructions. Angioplasty is most effective in arteries with shorter portions of disease and arteries that are only constricted, rather than entirely blocked.
- Atherectomy is a type of peripheral operation that opens arteries that are blocked by plaque. Your provider will use a catheter (a long, narrow tube) with a sharp blade, laser, or rotating device on the end to scrape away, dissolve, or break up plaque without making a big incision during an atherectomy.
- The surgical restoration of blood flow to restore perfusion distal to a blocked or otherwise disrupted arterial segment is known as peripheral vascular bypass. Peripheral vascular bypass surgery can involve any artery excluding those in the heart or brain.
- Thrombolysis and thrombectomy are procedures used to treat arterial thrombosis or embolism.
Physiotherapy Treatment Of Peripheral Artery Disease:
Physiotherapists would recommend an exercise schedule as the least invasive and most appropriate treatment for peripheral artery disease.
- Exercise on a Regular Basis
- Pain management
- Cardiovascular exercise
- Massage and sensory stimulation
- Muscle strengthening
- Mobilizations of joints and muscles
- Mobility exercises
- Provision of walking aids and footwear advice
- Walking On A Regular Basis: This can be done either outside or on a treadmill. Begin with short distances. If possible, select a path with occasional low-rise inclines.
- Toe Walking: On a flat surface, walk on the balls and toes of your feet. If you’re at home, do this exercise along a wall for support.
- Assisted Standing Calf Raises: Stand behind a chair, holding the backrest or a walking bar for support. Raise your heels and lower them. Your calf muscles can also get stiff, especially if you are used to wearing heels.
- Chair Leg Raises: Chair leg raises are great for increasing blood flow from the hips to the toes. Place your feet flat on the floor and sit in a chair. Lift and stretch your right leg off the floor. Hold it for 5 seconds before dropping it slowly. Repeat using your left leg. If you have any discomfort, break and relax.
Regular Physical Activity – This is the most effective treatment; a doctor will frequently recommend a supervised exercise training program. The patient may need to take it slowly at first. Simple walking regimens, leg exercises, and treadmill exercise programs three times per week can result in symptom reduction in as little as 4-8 weeks.
Dietary Modifications and Alterations – Many people with peripheral artery disease have high cholesterol levels. A low-fat, trans-fat, and cholesterol-free diet, as well as enough fruits and vegetables, can help lower blood cholesterol levels.
Smoking Cessation – Tobacco use significantly raises the risk of peripheral artery disease, heart attack, and stroke. Smokers may be four times more probable than nonsmokers to develop peripheral artery disease. Smoking cessation can assist to decrease the progression of peripheral artery disease and other heart disorders.
Prognosis:
It is essential for individuals diagnosed with peripheral artery disease to receive appropriate medical management and lifestyle modifications to control symptoms, prevent disease progression, and reduce the risk of complications such as limb ischemia and amputation. Treatment options may include lifestyle changes, medication to manage risk factors like high blood pressure and high cholesterol, supervised exercise programs, and in some cases, surgical interventions like angioplasty or bypass surgery. Regular follow-up with a healthcare provider is crucial to monitor disease progression and adjust the treatment plan as needed.
FAQs:
Can peripheral artery disease be prevented?
While it may not be possible to completely prevent peripheral artery disease, certain lifestyle choices can significantly reduce the risk. These include avoiding smoking or quitting if you are a smoker, maintaining a healthy weight, eating a balanced diet low in saturated fats, exercising regularly, and managing conditions such as diabetes, high blood pressure, and high cholesterol.
What are the potential complications of peripheral artery disease?
If left untreated, peripheral artery disease can lead to various complications. The restricted blood flow to the limbs can cause non-healing ulcers, infections, and tissue death (gangrene). In severe cases, this can lead to limb amputation. Peripheral artery disease also increases the risk of cardiovascular events such as heart attack and stroke.
Can peripheral artery disease affect other parts of the body besides the legs?
While peripheral artery disease primarily affects the arteries in the legs, it can also occur in other arteries of the body, such as those supplying blood to the arms, kidneys, and intestines. However, the symptoms and complications may vary depending on the specific location of the affected arteries.
Is peripheral artery disease a life-threatening condition?
Peripheral artery disease itself is not typically life-threatening. However, it is considered a significant marker of systemic atherosclerosis, a condition that affects the arteries throughout the body. This increases the risk of cardiovascular events, such as heart attack and stroke, which can be life-threatening if left untreated.



23 Comments