
8th THE VESTIBULOCOCHLEAR NERVE
The vestibulocochlear nerve (auditory vestibular nerve), known as the eighth cranial nerve, transmits sound and equilibrium (balance) information from the inner ear to the brain.
Table of Contents
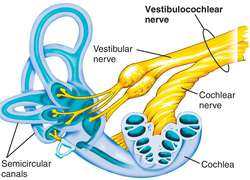
ANATOMY:
The vestibular and cochlear portions of the vestibulocochlear nerve are functionally discrete, and so originate from different nuclei in the brain:
Vestibular component – arises from the vestibular nuclei complex in the pons and medulla.
Cochlear component – arises from the ventral and dorsal cochlear nuclei, situated in the inferior cerebellar peduncle.
Both sets of fibres combine in the pons to form the vestibulocochlear nerve. The nerve emerges from the brain at the cerebellopontine angle and exits the cranium via the internal acoustic meatus of the temporal bone.
FUNCTION:
It is responsible for the special senses of hearing (via the cochlear nerve), and balance (via the vestibular nerve).
hearing:
The cochlea detects the magnitude and frequency of sound waves. The inner hair cells of the organ of Corti activate ion channels in response to vibrations of the basilar membrane. The magnitude of the sound determines how much the membrane vibrates and thereby how often action potentials are triggered.
equilibrium:
The vestibular apparatus senses changes in the position of the head in relation to gravity. The vestibular hair cells are located in the otolith organs (the utricule and saccule), where they detect linear movements of the head, as well as in the three semicircular canals, where they detect rotational movements of the head.
CLINICAL SIGNIFICANCE:
Symptoms of damage
Damage to the vestibulocochlear nerve may cause the following symptoms:
-hearing loss
–vertigo
-false sense of motion
-loss of equilibrium (in dark places)
-nystagmus
-motion sickness
-gaze-evoked tinnitus.
EXAMINATION OF AUDITORY FUNCTION:
Examinations that can be done include the Rinne test and the Weber test.

RINNE TEST:
The Rinne test is a hearing test, primarily for evaluating loss of hearing in one ear (unilateral hearing loss). It compares perception of sounds transmitted by air conduction to those transmitted by bone conduction through the mastoid. Thus, one can quickly screen for the presence of conductive hearing loss.
procedure:The Rinne test is performed by placing a 512 Hz vibrating tuning fork against the patient’s mastoid bone and asking the patient to tell you when the sound is no longer heard. Once the patient signals they can’t hear it, the still vibrating tuning fork is then placed 1–2 cm from the auditory canal. The patient is then asked again to indicate when they are no longer able to hear the tuning fork.
Normal hearing
Air conduction should be greater than bone conduction and so the patient should be able to hear the tuning fork next to the pinna (outer ear) after they can no longer hear it when held against the mastoid.
abnormal:
If the patient is not able to hear the tuning fork after it is moved from the mastoid to the pinna, it means that their bone conduction is greater than their air conduction. This indicates there is something inhibiting the passage of sound waves from the ear canal, through the middle ear apparatus and into the cochlea.
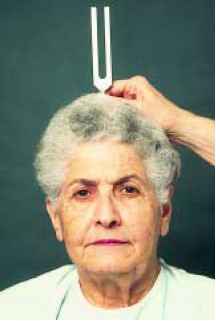
WEBER TEST:
In the Weber test a vibrating tuning fork is placed in the middle of the forehead, above the upper lip under the nose over the teeth, or on top of the head equi-distant from the patient’s ears on top of thin skin in contact with the bone. The patient is asked to report in which ear the sound is heard louder.
normal : A normal weber test has a patient reporting the sound heard equally in both sides. In an affected patient, if the defective ear hears the Weber tuning fork louder, the finding indicates a conductive hearing loss in the defective ear. In an affected patient, if the normal ear hears the tuning fork sound better, there is sensorineural hearing loss on the other (defective) ear.
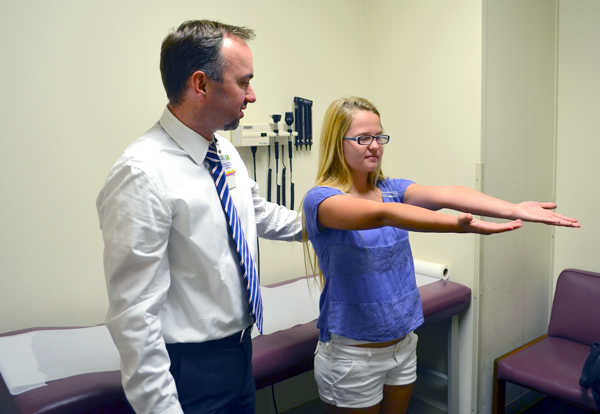
EXAMINATION OF VESTIBULAR FUNCTION:
On examining a patient with suspected vestibular dysfunction, observation for nystagmus is of primary importance prior to formal testing. Usually he complains of vertigo (illusion of movement of self or environment), saying that the room is spinning in the direction of the fast component.Testing of the inner ear is not a simple matter. Asking the patient to focus on your nose while using your hands to rapidly move the head to either side (“head thrust”) can provide some information. Usually, individuals are able to maintain good focus if the inner ears are intact.
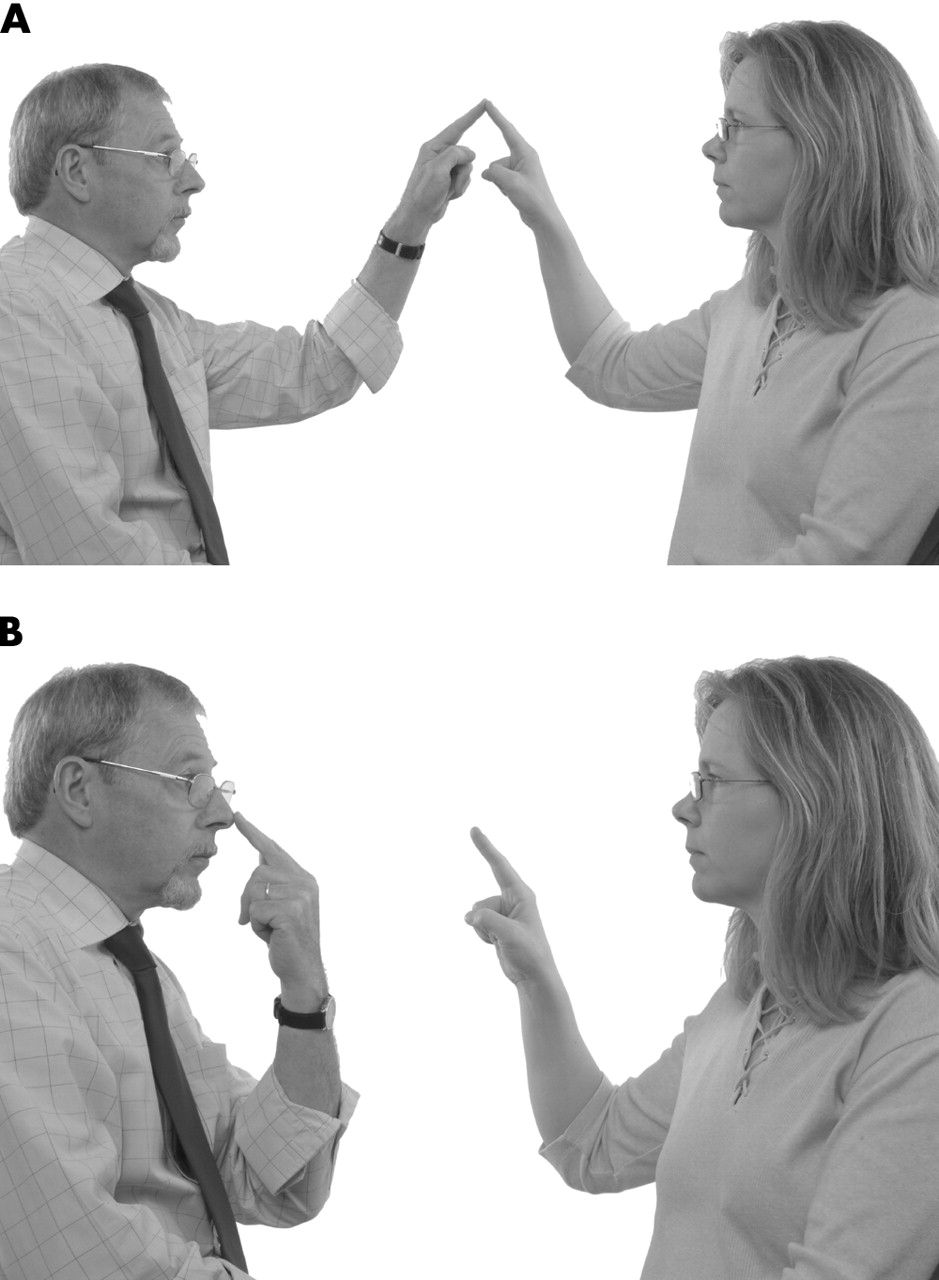
other test are:
-past pointing
-finger nose test
-romberg test

DISORDERS:
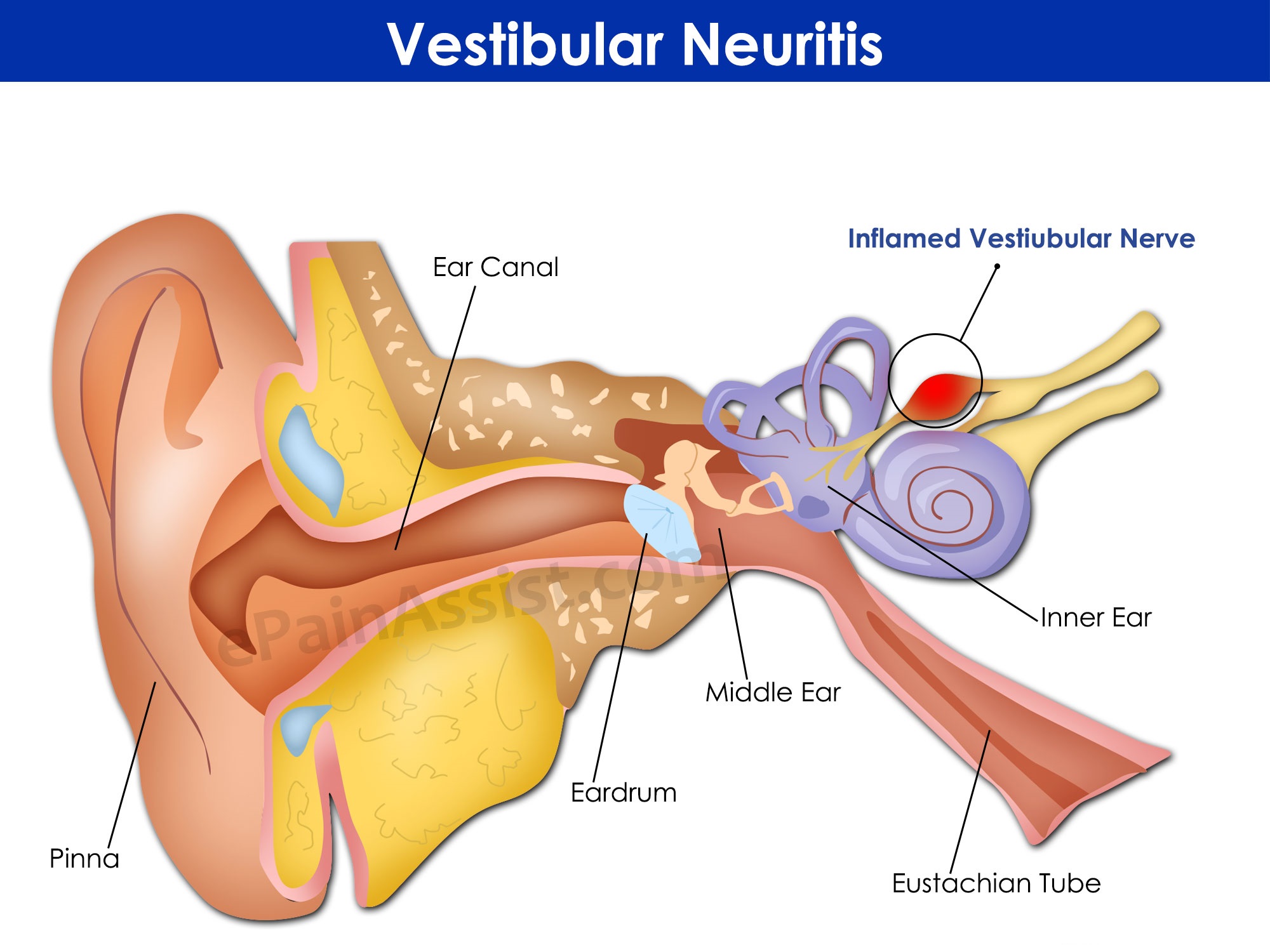
VESTIBULAR NEURITIS:
Vestibular neuritis refers to inflammation of the vestibular branch of the vestibulocochlear nerve. The aetiology of this condition is not fully understood, but some cases are thought to be due to reactivation of the herpes simplex virus.
It presents with symptoms of vestibular nerve damage:
-Vertigo – a false sensation that oneself or the surroundings are spinning or moving.
-Nystagmus – a repetitive, involuntary to-and-fro oscillation of the eyes.
-Loss of equilibrium (especially in low light).
-Nausea and vomiting.
The condition is usually self-resolving. Treatment is symptomatic, usually in the form of anti-emetics or vestibular suppressants
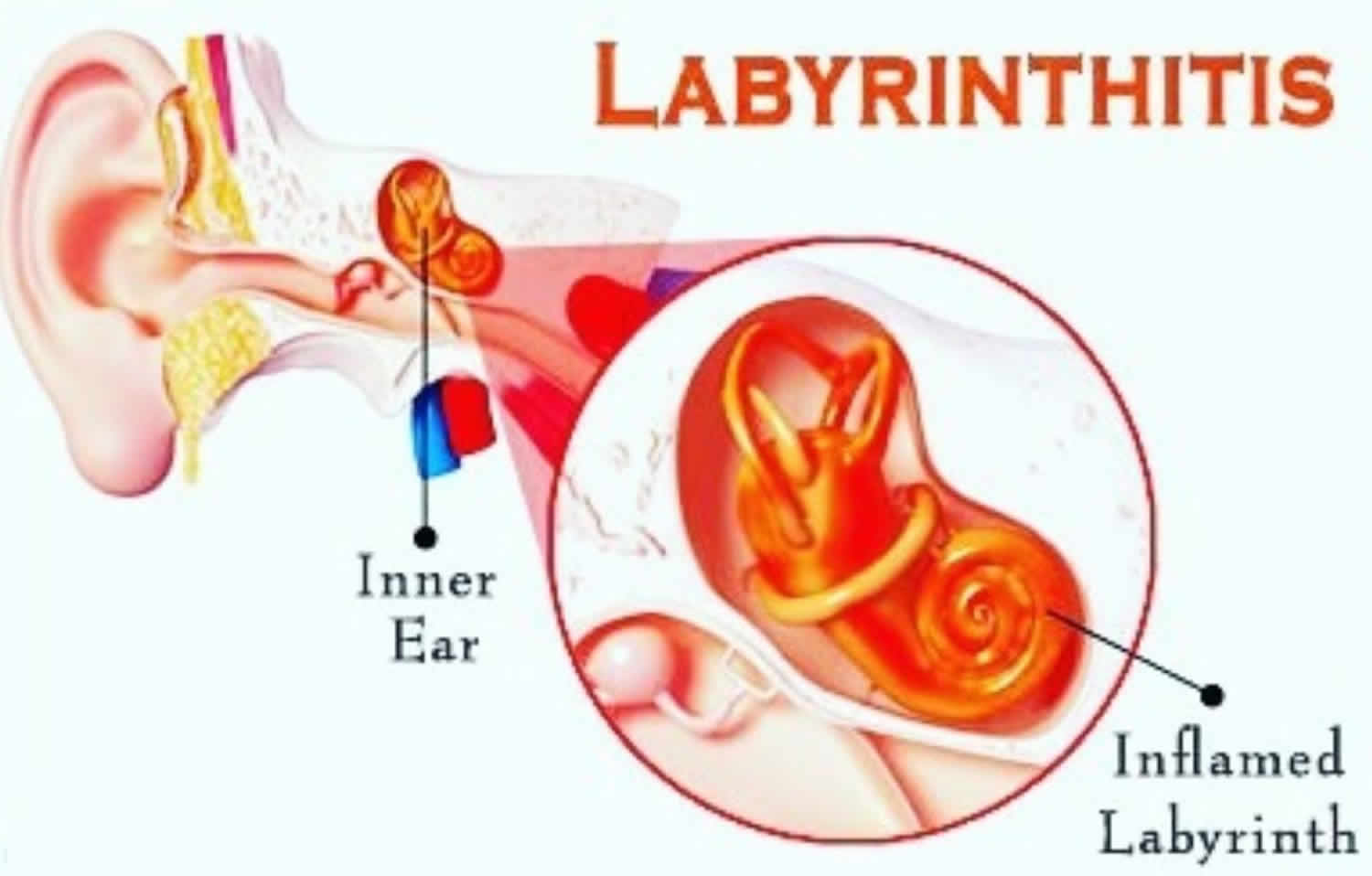
LABYRINTHITIS:
Labyrinthitis refers to inflammation of the membranous labyrinth, resulting in damage to the vestibular and cochlear branches of the vestibulocochlear nerve.
The symptoms are similar to vestibular neuritis, but also include indicators of cochlear nerve damage:
-Sensorineural hearing loss.
-Tinnitus – a false ringing or buzzing sound.

Thank you very much, nice way to understand