Tibia Fracture
Table of Contents
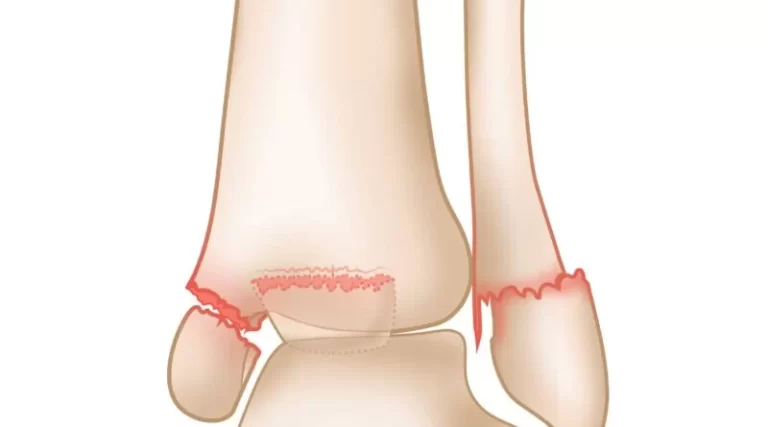
What is a Tibia Fracture?
A tibia fracture refers to a break or fracture in the tibia bone, which is the larger of the two bones in the lower leg. It is commonly known as the shinbone and is responsible for bearing much of the weight of the body.
Tibia fractures can occur due to various reasons, such as trauma, falls, sports injuries, or excessive stress on the bone. The severity and treatment of a tibia fracture depend on the location, type, and extent of the break.
The American Academy of Orthopaedic Surgeons claims that the tibia is the long bone in the body that fractures most frequently. Any cracks or breaks in the tibia bone can be referred to as tibia fractures.
One of the two bones that make up the lower leg is the tibia, jointly with the fibula. The tibia is the larger of each of these bones.
The tibia plays a very crucial role in body mechanics, as it is:
- The tibia is the biggest bone of the lower extremity
- answerable for keeping most of the body load
- important for correct knee and ankle joint mechanics
A fractured tibia frequently happens with different types of tissue injury to the nearby muscles or ligaments. It must always be checked out by a medical expert.
Types of Tibia Fractures
Depending on the mechanism of the broken bone, the severity and kind of fracture can differ. It can be a transverse fracture, which means the break is horizontal across the bone, or oblique, meaning the break is at an angle.
Proximal fractures are those that affect the proximal portion of the tibia. Tibia shaft fractures happen below this region.
The tibia can have the types of fractures:
- Stable fracture. A stable fracture is defined as a involves a break in the bone that remains most of the bone intact and in its original position. The broken portions of the tibia line up and hold their correct position during the recovery time. This is understood as a non-displaced fracture.
- Displaced fracture. A displaced fracture is defined as a break in the bone that displaced part of the bone so that it is no longer aligned within the normal position. Operation is frequently required to fix this kind of fracture and realign the bones back together.
- Stress fracture. Stress fractures, also called hairline fractures, are common overuse syndromes. These fractures are minor, light cracks in the bone.
- Spiral fracture. It’s defined as when a twisting motion reason for a crack, there may be a spiral-shaped fracture of the bone.
- Comminuted fracture. It’s the most severe and complicated type which define as when the bone fractures into three or more pieces, this is named a comminuted fracture.
When bones are fractured, they can either remain under the skin or break via its surface. Open fractures are fractures where a damaged bone breaks through the skin. With closed-type fractures, the bone does not break the skin and is not exposed to the environment, though there may even be internal tissue injury.
Cause of Tibia Fracture
Long bones in the body are strong, but there are various manners in which a person can cause a tibia fracture. These contain:
- traumatic injuries, such as road traffic accidents or falls
- sports that involve repeated impact to the shinbones, such as long marathon
- injuries from contact sports for example American football
- osteoporosis, which causes the bones weaker than normal
- overuse syndromes, for example, those caused by running, can result in stress fractures of the foot, ankle, tibia, or hip.
Symptoms of Tibia Fracture
Symptoms of a fractured tibia can have:
- a localized pain in one region of the tibia or various different places if there are multiple fractures
- swelling at the lower limb
- problem or difficulty standing, walking, or taking weight
- leg deformity or irregular leg length
- bruising or discoloration near the shinbone
- altered sensation
- bone protruding via the fascia
Diagnosis
To diagnose a fractured tibia, a physician’s preference asks about a person’s medical history and how the injury was caused. They will do an assessment and order diagnostic tests to evaluate the extent of the injury and whether the bone is fractured. This is critical for choosing the best approach to treatment.
Diagnostic tests may have:
- an X-ray to have a visualized of the tibia bone
- a computed tomography (CT) scan, also named a CAT scan, which is additional powerful than an X-ray and provides a 3-D picture of the bone
- a magnetic resonance imaging (MRI) scan for a precise image of the muscles, ligaments, and bones around the tibia
An MRI scan is usually used if the other scans have not been able to analyze the situation.
A person with a fractured tibia might require physical therapy as well as aids or a walker in order to assist them get back on their own in a number of situations.
Evaluation
Considering the range of movement and stability are usually difficult because of pain.
The neurovascular assessment is extremely necessary to evaluate the dorsalis pedis and posterior tibialis arteries. The soft tissues must be considered to determine any signs or symptoms of compartment syndrome. The skin must be considered for lesions, abrasions, fractures blisters, and the state of the compartments. To properly diagnose compartment syndrome, a high threshold of suspicion is required.
Recommended imaging contains complete-length AP and lateral views of the concerned site, AP, lateral and oblique views of the same side knee and ankle. CT scan is meant to place an intra-articular involvement and exclude posterior malleolar fracture in spiral distal third fractures.
Classifications
Some classifications assist with treatment judgments.
Western and Tscherne
This is a classification of closed fracture soft tissue damage and is as follows:
• Grade 0: Injuries from indirect impact with minimal soft tissue injury
• Grade 1: Superficial contusion pr abrasion, uncomplicated fractures
• Grade II: Deep abrasions, muscle or skin bruise, direct hit, approaching compartment syndrome
• Grade III: Extreme skin contusion, crushed skin or muscle destruction, subcutaneous degloving, recent compartment syndrome, and rupture of a major blood vessel or nerve
The Gustilo-Anderson
This classification is used to evaluate open tibia fractures.
- Type I is restricted periosteal stripping, sterile wound < 1 centimeter
- Type II mild to moderate periosteal stripping; damage more than 1 cm in length
- Type IIIA significant soft tissue damage, marked periosteal stripping with damage that is usually more than 1 centimeter in length with no flap needed
- Type IIIB is significant periosteal stripping and soft tissue injury with a flap needed because of insufficient soft tissue coverage
- Type IIIC these are significant soft tissue damage with a vascular injury needing restoration
Treatment of Tibia Fracture
Treatment of a fracture of a tibia relies on different aspects, concerning a person’s general health at the moment of the fracture, the mode of the mechanism of the injury and severity of the injury, and the existence or degree of damage to the soft tissues that cover the tibia.
In extreme circumstances, the operation can be required to create sure the bone recovers correctly. A surgeon may insert metal screws and plates on the bone to keep it in the proper place, permitting it to recover with minimal long-term damage.
- A splint or cast to keep the bone in place, stop it from moving and permit it to recover. A splint can be removed easily and so it is a more flexible treatment option than operational ones.
- A longitudinal traction or functional brace, is used in circumstances of less severe cracks to keep the bone in position while it recovers.
Non-Operative Treatment
Closed-reduction and nonoperative treatment in a long leg cast are satisfactory for fractures in < 5 degrees of varus-valgus angulation, < 10 degrees in anterior-posterior angulation, more than 50% cortical apposition, smaller than one-centimeter shortening, and < ten to twenty degrees of flexion and smaller than ten degrees of rotational malalignment afterward to reduction.
Operative Treatment
External Fixation
Treatment of choice when consequential soft tissue compromise is exited or in more than two trauma cases where damage-control orthopedics is essential.
Intramedullary Nailing (IMN)
This is the intervention of preference for operative fixation.
If corresponding outcomes of Intramedullary Nailing (IMN) with external fixation, Intramedullary Nailing (IMN) is correlated with reduced malalignment and corresponded to closed reduction, Intramedullary Nailing (IMN) is correlated with reduced union time and time to weight bearing.
Percutaneous Plating-Shaft
This approach is frequently utilized in the lower tibia or proximal-third fractures that are also proximal or lower for intramedullary nailing.
Amputation
This is another treatment technique but can be hard to get the patient to buy into this treatment. The mangled extremity severity score (MESS) can assist indicate when an amputation is necessary. A score of seven or above is greatly predictive of amputation. mangled extremity severity score (MESS) has great specificity but low sensitivity in predicting amputations. Relative indications have significant soft tissue trauma, warm ischemia of more than 6 hours, and severe at the same side foot trauma. It is essential to mention that loss of plantar sensation is not a total indication of amputation.
Recovery
Recovery from a tibial fracture changes depending on how severe the fracture is.
An individual will usually heal within four to six months. The healing period can be longer for an entire crack compared to a partial one and may take extended if a person has insufficient health for different causes.
It can take longer time than this time frame for someone to be able to return to their regular activities. People must always obey their physician’s recommendations regarding returning to walking, exercising, and another physical exercises later a leg fracture.
Specific exercises can support taking the stress off the tibia bone, for example, exercises that strengthen the hips, calves, and thighs. This protection may also avoids future damages from occurring.
Complications
- Complications of a tibia fracture may include:
- complications from an operation or the requirement for further surgeries
- nerve, muscle, or blood vessel damage
- compartment syndrome, a severe condition in which there is a reduction in blood circulation to the limb because of swelling
- infection in a bone is known as osteomyelitis
- development of a non-union where the bone does not recover
- In many circumstances, a tibial fracture will be successfully managed without any complications.
FAQ
The management of an open tibial fracture initiates with antibiotics and a tetanus shot to reduce the threat of infection. Then the damage is sterilized to remove any debris and bone pieces. The operation can also be required depending on the injury extent, the quantity of tissue damage, and any vascular (circulation) issues.
The operation can be needed to repair a broken tibia. Open fractures require to be washed and treated directly away since they have a threat of infection. There are various operative procedures that can be used relying on where the tibia is fractured, how extreme the fracture is, and if different parts of the leg were also injured.
Several fractures recover in six to eight weeks, but this differs tremendously from bone to bone and in each person depending on a multiple of the factors discussed above. Hand and wrist fractures frequently recover in four to six weeks whereas a tibia fracture may take twenty weeks or more.
Most tibial shaft fractures carry four to six months to recover fully. Few take even longer, particularly if the fracture was open or cracked into several fragments or if the patient uses tobacco products
Inadequate levels of vitamin C, vitamin D, and calcium can avoid a bone from recovering. An infection in the bone, which is known as osteomyelitis, can even delay or avoid recovery. A bone can become infected if bacteria from damage on the surface of the skin travel through the bloodstream to the bone
Yes, flexing the knee can begin instantly after a tibial plateau fracture if you did not have an operation. If you had an operation then you can begin flexing the knee to 90 degrees 1 week after the operation. Once the incision is completely cured(10-14 days) you can go beyond 90 degrees of knee flex.
Relying on the kind and severity of the fracture, the bone stays fairly normal for the rest of the patient’s life. But we all understand that as we get older, it is it carries longer to heal from a fracture and the results are relatively less specific.