Quadriceps Tendon anatomy
Table of Contents
Introduction
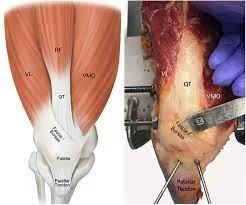
The thick, robust tendon that joins the quadriceps muscles to the patella (kneecap) is called the quadriceps tendon. It is an essential component of the leg’s extensor mechanism and is critical in knee joint movement. The four quadriceps muscles, which are found in the front of the thigh, converge to produce the quadriceps tendon.
Quadriceps tendon
Origin: The united tendon of the four quadriceps muscles is where the quadriceps tendon begins. The vastus muscles come from different sections of the femur, while the rectus femoris comes from the anterior inferior iliac spine.
Insertion: The bottom or base of the patella receives the quadriceps tendon. The quadriceps tendon contains the patella, a sesamoid bone a bone buried in a tendon.
Function: The strongest knee extensor is the quadriceps femoris. The knee can be extended by all four of its parts, although they can only do so in certain directions. The patella is pulled along the lower limb’s mechanical axis by the rectus femoris muscle. The remaining muscles, on the other hand, pull in both proximally and lateral directions since they originate from the femur. Herein lies the critical importance of the vastus obliquus, the previously discussed portion of the vastus medialis. Its fibers that are oriented horizontally resist the pull of the three vastus, which helps to stabilize the knee during extension and keeps the patella from dislocating.
Since the rectus femoris muscle crosses both the hip and the knee joints, it performs extra functions in addition to extending the knee. It facilitates thigh flexion by acting on the hip joint. This muscle assists in the anterior flexion of the pelvis toward the thigh when its patellar attachment is stabilized. The rectus femoris can also extend the knee and flex the hip at the same time.
- Striking a Ball: When coupled hip flexion and knee extension are required, the rectus femoris is activated.
- Moving around: As the leg swings forward, the quadriceps muscles lengthen it, and when the heel hits the floor, they prevent the knee from bending.
- Patella Controlling: During the last phases of knee extension, the vastus medialis is most active, regulating the patella’s movement.
- Stepping Exercises: like climbing stairs
- Squats: When squatting, the quadriceps regulate the downward motion.
- All four muscles contract statically to offer stability when standing on one leg.
- Lifting the Leg Off the Bed: Raising a straight leg requires a forceful contraction of the rectus femoris.
Interesting Info: The quadriceps muscles don’t do anything when you’re just standing there.
The structure: The tendon gives the knee joint strength and stability. It is produced up of thick, fibrous connective tissue. Because walking, running, and jumping create stresses on the tendon, the collagen fibers are arranged in a parallel pattern within the tendon.
The nerve supply: femoral nerve
Encircling Structures: The patellar ligament, a continuation of the tendon that runs from the patella to the tibial tuberosity on the anterior surface of the tibia, is tightly linked to the quadriceps tendon. The knee’s extensor mechanism is a continuous structure of the patellar ligament and quadriceps tendon.
Trauma or overuse can result in injuries to the quadriceps tendon, such as tears or ruptures. Medical intervention, such as rest, physical therapy, or in extreme situations, surgical repair, may be necessary for certain ailments. If you have knee pain or think there may be a problem with your quadriceps tendon, you should consult a doctor.
Rectus femoris
Place of origin and insertion: The fusiform muscle, the rectus femoris, has two heads. It comes from the anterior inferior iliac spine (straight head) and the supraacetabular groove (reflected head), two locations on the ilium. The anterior side of this area is covered by the two heads coming together to form a single muscular belly that runs down the thigh almost vertically. Converging muscle fibers form a thick tendon that inserts into the patella’s base. There are rare instances where the rectus femoris has a third head that comes from the iliofemoral ligament.
Relationships: The sartorius, iliacus, and tensor fasciae latae muscles are situated deep in the proximal portion of the rectus femoris muscle. The anterior compartment of the thigh is filled up, all the path up to the rectus femoris. These are composed of the lateral circumflex femoral artery, the vastus intermedialis, the hip joint capsule, the anterior boundaries of the vastus lateralis, and periodic femoral nerve branches.
Blood supply: The quadriceps artery, which can originate from the lateral circumflex femoral, deep femoral, or femoral arteries, provides blood to the rectus femoris muscle. To a lesser degree, the superficial circumflex iliac and lateral circumflex femoral arteries also give blood to the rectus femoris.
Action: hip joint flexion at the thighs, Leg extension at the knee joint
Place of origin and insertion: The pectineal line of the femur, the medial lip of the linea aspera, the inferior portion of the intertrochanteric line, and the proximal half of the medial supracondylar line are the landmarks from which the vastus medialis muscle originates. Its fibers spiral around the muscle’s long axis as it descends obliquely through the thigh.
The fibers at the bottom of the structure form a conspicuous bulge above the patella’s medial side, arranged in an almost horizontal plane. this specific region of the vastus medialis is the vastus obliquus. Lastly, the quadriceps femoris tendon allows the muscle to penetrate the base of the patella. A portion of its tendinous fibers insert into the tibia’s medial condyle as they travel downhill
Relation: The rectus femoris partially covers the vastus medialis, which is located medial to it. The superficial surface of the vastus medialis is also crossed by the sartorius muscle. The lateral wall of the adductor canal, also known as Hunter’s canal, is formed by the vastus medialis in the middle third of the thigh.
The sartorius medially and the adductor longus and magnus posteriorly complete this canal. It carries the saphenous nerve, femoral vein, femoral artery, and nerve to the vastus medialis (both of which are branches of the femoral nerve).
Blood supply: Three femoral artery muscle branches feed blood to the vastus medialis. The descending genicular artery and the deep femoral artery also provide it with some little contributions.
Action: Knee Joint extension of the Leg
Origin and insertion: Of the four quadriceps femoris muscles, the vastus lateralis is the biggest. The proximal half of the intertrochanteric line, the anterior and inferior borders of the greater trochanter, the lateral lip of the gluteal tuberosity, and the proximal half of the lateral lip of linea aspera are among the spots on the femur where a broad aponeurosis gives rise to it. Many muscle fibers originate from the deep surface of the aponeurosis, which covers the upper three-quarters of the muscle.
Via the quadriceps tendon, the muscle inserts at the base of the patella after descending via the lateral portion of the anterior thigh compartment. A portion of the tendinous fibers descend to the proximal tibia, where they merge with the iliotibial tract and insert into the lateral condyle of the tibia.
Relation: The lateral intermuscular septum divides the vastus lateralis muscle, which is located superficially to the biceps femoris muscle. The gluteus maximus and tensor fasciae latae cover the lateral aspect of the muscle. It is connected to the vastus intermedius on its medial surface, and the lateral femoral circumflex artery and femoral nerve branches divide it from it.
Blood supply: The superior medial artery, a branch of the lateral circumflex femoral artery, provides blood to the vastus lateralis.A branch of the quadriceps artery is the inferior medial artery. The lateral artery is the deep femoral artery’s initial perforator.
Action: Extension of the knee joint
vastus Intermedialis
Place of origin and insertion: Between the vastus lateralis and vastus medialis muscles is the vastus intermedius muscle. It initiates at the proximal two-thirds of the femur’s shaft, which is the anterior surface of the bone. The muscle fills the space between the vastus medialis and lateralis as it descends over the anterior surface of the femur.
It releases a broad aponeurosis at the distal femur level, from which the common quadriceps tendon links it to the base of the patella. Additionally, it inserts into the tibia’s lateral condyle.
Relations: The other quadriceps femoris muscles round the Ventus intermedius fully. Its anterior surface is covered by the rectus femoris, while its lateral and medial surfaces are occupied by the vastus lateralis and medialis, respectively.
Blood supply: The deep femoral artery and the quadriceps artery provide blood to the vastus intermedius.
These four muscles combine to generate the quadriceps tendon, which is located directly above the patella. The tendon attaches to the patella’s upper surface as it descends farther. The patella is then attached to the tibial tuberosity, a bony protrusion on the tibia, by the patellar tendon, which then extends inferiorly. The patellar tendon is involved in the final connection to the tibia and is occasionally thought of as an extension of the quadriceps tendon.
The patellar tendon and the quadriceps tendon are essential for the knee joint’s extension. Walking, running, jumping, and stair climbing are among the activities that greatly depend on the quadriceps tendon and related muscles performing at optimal capacity. Tears or strains in the quadriceps tendon can have a major effect on knee function and may need to be treated medically to be properly rehabilitated.
The Quadriceps Tendon’s Superficial Layer
One of three probable locations for the RF, the most superficial muscle in the quadriceps group, is the superior third of the patella’s anterior surface and the base’s anterior section. According to one explanation, the RF tendon joins the ligamentum patellae superficially after attaching to the patella in part.
According to a second view, the tendon of rectus femoris unites with the tendon of vastus intermedialis to form a unilaminar suprapatellar tendon, which may receive some fibers from the tendons of vastus lateralis and vastus medialis or their connection to the patella independently. The trilaminar tendon is formed when the superficial quadriceps tendon insertion connects to the tendons of the other quadriceps muscles. The unilaminar or trilaminar superficial fibers of this common tendinous connection cross the patella and merge into the patellar ligament.
The Quadriceps Tendon’s Intermediate Layer
Together, the vastus medialis and lateralis combine centrally to form a continuous aponeurosis that continues laterally and medially to insert into the sides of the patella, as well as into the base of the patella, immediately posterior to the insertion of rectus femoris. Further laterally, the vastus lateralis terminates in an aponeurosis that extends distally to the superolateral side of the patella and melds with the lateral side of the suprapatellar or rectus femoris tendon. Additional fibers join to the tibia’s medial condyle after passing superficially through the patella. The vastus lateralis then expands laterally and merges with the knee capsule to produce a portion of the lateral patellar retinaculum.
The majority of the vastus medialis fibers terminate in an aponeurosis that merges with either the rectus femoris tendon or the medial side of the suprapatellar tendon. More distally than fibers arising from any other region of the quadriceps group, the most distal fibers adhere directly to the medial margin of the patella. A tendinous enlargement extends along the medial side of the patella from the distal border of the vastus medialis.
As a component of the medial patellar retinaculum, the deep fibers of this extension support the joint capsule. By adding to the MPFL’s superficial layer, the obliquely oriented fibers from the more superficial vastus medialis obliques support medial patellar stability. Additional tendinous fibers join to the lateral tibial condyle by obliquely crossing the patella.
The term “vastus medialis obliques” is frequently used to refer to the farthest-extending muscle fibers of the vastus medialis. In contrast to the vastus lateralis obliques, the presence of a division, such as a thin layer of fat or fascia or a nerve branch between the oblique and longitudinal heads of the vastus medialis, can vary, making it challenging to distinguish between the two heads.
Whether the vastus medialis obliques is a distinct muscle with its innervation is a matter of debate. A distal-proximal dissection that makes it impossible to discern between a fascial separation and the lateral segment of a tunnel encircling the sartorius is what leads to the formation of a fascial plane.
Even though anatomists and surgeons frequently acknowledge the existence of vastus medialis obliques, the vastus lateralis obliques receive little consideration. This anatomically different group of vastus lateralis fibers is distinguished from the main belly of the vastus lateralis by a shift in fiber orientation or a thin coating of fat or loose fascia.
Some people claim that this muscle group originates from the lateral intermuscular septum, while others say that the iliotibial tract (ITT) is where it comes from. Because these fibers have a more lateral insertion on the patella than the longitudinal head of the vastus lateralis, they are thought to be significant because they offer a more direct lateral pull on the extensor mechanism.
The Quadriceps Tendon’s Deep Layer
The lateral intermuscular septum is the vastus intermedialis’s distal origin, and the vastus lateralis is its proximal origin.
It either merges with the vastus medialis and vastus lateralis or inserts itself into the base of the patella posteriorly through a broad, thin tendon. mentioned that the suprapatellar tendon, which inserts on the base of the patella, can be formed by the union of the vastus intermedialis and the rectus femoris. This insertion strengthens the patellofemoral ligaments medially and laterally.
The Superficial Fibrous Layers of the Quadriceps Tendon and Related Structures
The three distinct and independent layers of fibrous tissue covering the anterior knee are easily distinguished. The patellofemoral and meniscopatellar ligaments form the deep anterior fibrous layer, which is medial and lateral to the patella. Compared to the lateral patellofemoral ligament, the medial patellofemoral ligament is stronger and larger.
There are two layers within the intermediate layer: the superficial and deep midline layers. The fibers that form the quadriceps and patellar tendons, as well as the crossing vastus medialis and vastuslateralis fibers that pass to the opposing side’s tibial condyles, make up the deep midline layer. The superficial midline layer is a thick extension of the ITT that extends laterally.
The superficial midline layer is a thin layer that extends from the sartorius and joins the fascia lata medially. The fascia lata extends proximally and the crural fascia extends distally into the superficial aponeurotic layer. Because haphazard inspections have given us the impression that the quadriceps tendon forms in a manner that is frequently very different from how it normally
Palpation the quadriceps tendon
When palpating the anterior thigh, one should feel for any muscle defects, locate the area of maximum sensitivity, and measure the length of the torn muscle.
assessing one’s quadriceps’ strength should involve assessing one’s ability to withstand hip flexion and knee extension. Resisted knee extension with the hips flexed and extended is a vital segment of rectus femoris strength assessment that is satisfactory.
In practical terms, this is best achieved by assessing the patient while they are both seated and prone-lying. It is requested of the patient to resistively extend their leg (at the knee). The quadriceps femoris will not contract if there is injury to the femoral nerve. The best way to estimate the flexibility and range of motion of the quadriceps is to lie prone.
The patient usually experiences pain when direct palpation over the muscle tension, passive stretching, and resisted muscle activation are used.
The grading of a muscle injury and the guidance for additional diagnostic tests and therapy are determined by evaluating the muscle’s tenderness, strength, and any visible defects at the time of damage.
Examine each muscle head for imbalances that could cause issues with patella tracking, for example.
Look for any muscle imbalances, such as. A common imbalance that develops in runners is between their well-developed quadriceps and strong hamstrings.
When nerve palsy is suspected, the femoral nerve can be tested using the quadriceps femoris muscle.
Functional test for quadriceps tendon
Test for Timed Up and Go (TUG)
A straightforward assessment tool used to gauge your functional mobility is the Timed Up and Go test, or TUG test. The TUG test clocks how long it takes you to get up, go forward 10 feet, turn around, move back, and then sit down again. The TUG test is most frequently used in physical therapy to determine your level of mobility safety. Your healthcare professional may also use it to gauge how likely you are to fall and how well you can balance while walking.
The goal of the TUG test
A healthcare provider can learn more about your mobility abilities with the TUG test. It can be used to gauge how well therapy is working for you both during your initial appointment with a physical therapist and during your course of treatment. The American Geriatric Society also suggests it as a regular autumn screening test. Because the TUG test is simple to administer and most people can finish it, it is widely utilized with older persons. A more thorough Get Up and Go (GUG) exam may incorporate the TUG test. Additional tasks, such as standing with your eyes closed or sitting in a chair without utilizing the armrests, are usually included in GUG tests.
The TUG test has a lot of advantages
- Very little equipment is required.
- It can be done practically any place.
- It takes a few minutes at considerable.
- You can do it on your own at home.
- The test can be administered with very little instruction.
Ways to get ready for the timed up-and-go Exam
Only a few pieces of equipment are needed for the TUG test
- A chair with a flat back and a sturdy seat
- A stopwatch on a manual or smartphone
- A ruler or measuring tape
- A chalkboard or piece of tape
- Typical walking footwear
- Any walking aid that you regularly use, like a quad cane or walker
The therapist will position a chair in an open area and measure three meters (9.8 feet) from the front edge of the space to set up the test. The distance is marked on the floor with a little piece of tape or chalk. For the chair to stay in place when you stand, stability is essential. Usually, you can avoid this by doing the test in an area with carpeting.
How to Take the TUG Exam: You will sit in the chair and begin the TUG exam with your arms comfortably resting at your sides or on your lap (not on the armrests). Your hips should be positioned back in the seat while you are sitting properly. The therapist signals “Go” and sets the stopwatch to begin the test. After that, your movements getting up from the chair, walking three meters, turning around, and getting back into the chair—would be timed. Your TUG score is the time that was recorded using the stopwatch.
A practice run is often followed by two timed tests administered by physical therapists. Your final score is the mean of the two recorded test times. Although using an assistive device is allowed, using any other kind of physical aid is not advised. Someone should be by your side to keep you from falling if your balance is off, but they shouldn’t hold you up. The TUG test has no time limit. In general, older adults in good health can finish the task in ten seconds or less.
Very elderly and weak people could need two minutes or longer. If your physical therapist or healthcare professional approves, you can administer the TUG test at home. However, if you have serious problems with your balance or mobility, you should never attempt it by yourself.
Interpreting the Outcomes
Based on how long it takes to finish the exam, mobility is evaluated
< 10 seconds indicates normal,< 20 seconds indicates good mobility, able to go outside without assistance.
Less than 30 seconds results in balance and walking issues; requires walking assistance while walking outside
Conditions Related to the quadriceps tendon
Numerous sports and physical activities put a lot of strain on the quads, which raises the possibility of injury to the quad muscles themselves. Because it covers the other quad muscles and is closest to the skin, the rectus femoris is the quadriceps muscle that sustains injuries the most commonly.
when you sustain an injury to your quadriceps muscle, you should experience troubles with functional mobility, or the capacity to bring out day-to-day activities. you may be surprised to learn that your quadriceps muscles allow you to move around in bed. They should aid you in moving from one side to the other and in rushing your base when you’re lying down. Your quadriceps maintain the proper posture of your kneecap.
Your kneecaps and/or quadriceps may be affected by the following injuries:
Quadriceps contusion: A contusion, or bruise, is the most typical type of quadriceps injury. It occurs when a blow to the thigh tears and bleeds the quadriceps muscle. The surrounding muscle becomes inflamed as a result. Extending the knee can be extremely painful in cases of severe quad contusions.
A quadriceps strain is an injury that results from overstretching the muscle and rupturing the muscle fibers. Because of the pulling sensation at the front of the thigh, a strain may be described as “pulling” the muscle. A strain results in muscle soreness and edema. Additionally, bruising and a brief loss of strength in the strained muscle are possible. It may not be possible for you to straighten your knee if the rip is large enough to cause the quads to split from the kneecap.
Tendonitis, or inflammation of a tendon, is a condition that affects the connective tissues that link muscles to bones in the quadriceps. Inflammation of the quad muscles and quad tendon is caused by quadriceps tendonitis. This is a typical overuse ailment brought on over time by excessive strain on the quadriceps and/or knee joints. When you move your knee, the discomfort and swelling above the kneecap get worse.
Kneecap dislocation: This injury occurs when the bone directly below the kneecap is torn off by your quadriceps muscle, causing the kneecap to slip out of its grooveTrauma, such as a fall or sports injury, is almost always the reason for this. When the harm materializes, significant knee discomfort and a “popping” feeling could be present. Straightening the knee can be quite painful and difficult since it swells up quickly.
Excessive running and jumping can cause patellofemoral stress syndrome, which is an inflammation under the kneecap caused by continuous stress on the knee joint. Because the quads can’t keep their position, the kneecap rubs against its groove. Walking downstairs or downhill exacerbates the discomfort and swelling caused by this chronic overuse injury under the kneecap and in the front of the knee.
Iliotibial band syndrome: The iliotibial band is a lengthy tendon that runs from your hip bone to your shin bone on the outside of your thigh. With the syndrome of the iliotibial band, This tendon causes pain and inflammation on the outside of the knee as it grinds against your hip or knee bones.
This could happen if your quadriceps are weak or tight, or if your hamstrings are weaker than your quadriceps. Excessive knee bending, such as that which happens during cycling or running, can also cause it.
Paralysis and quadriceps paresis: The most common causes of quadriceps paresis and paralysis are spinal cord injuries and strokes, which result in muscle weakening or total loss of function. A pinched nerve in the lower back, such as the L3 vertebra, can also result in quadriceps paresis. This condition results in significant disability and instability of the knee.
Compartment syndrome: Sports injuries are the most common cause of this uncommon, excruciating, and potentially fatal illness. The syndrome might appear hours after a direct strike to the leg causes a quadriceps contusion or vascular (vein) injury. As pressure builds up in the quad, there is a reduction in blood flow to the area, which can lead to damage to the muscles and nerves. In drastic events, the harm can be uncorrectable.
Muscle cramps: You are familiar with the sensation if you have ever experienced a cramp in your leg. Your quadriceps may become painful with a knot as the muscle contracts and relaxes. Occasionally, a cramp can strike out of the blue, leaving your leg paralyzed by pain. Several typical reasons for thigh cramps include dehydration, pregnancy, poor circulation, and muscle fatigue. Some medical illnesses and treatments, including vascular disease, thyroid abnormalities, and type 2 diabetes
Treatment
The particular problem that is impairing the quadriceps muscle(s) will determine how it is treated. The options include surgery and medication as well as rest and rehabilitation activities.
The majority of quadriceps contusions are small and resolve on their own in a matter of weeks. If you keep applying pressure to the injured muscle, it may take longer for severe contusions to heal. They might accept up to six weeks to cure. The RICE method which stands for rest, ice, compression, and elevation is used to treat contusions. This is the best method for healing the contusion, minimizing discomfort, and reducing swelling.
Quadriceps strain: If you give your strained quad enough rest from physical activities, mild to moderate strains may take up to three weeks to heal. In addition to reducing discomfort and swelling, the RICE technique can expedite the healing process. Physical therapy may be recommended by your healthcare practitioner if the strain is more severe
Quadriceps tendonitis: RICE and nonsteroidal anti-inflammatory medications (NSAIDs), such as Aleve (naproxen) and Advil (ibuprofen), are recommended as early treatments for this condition. For tendonitis, physical therapy is frequently advised to reduce discomfort and prevent additional damage. Pain during regular activities might be minimized by bracing or taping the patella. You can wear custom orthotics, or shoe inserts, to assist in maintaining the appropriate alignment of your knee.
Kneecap dislocation: Kneecaps that are dislocated frequently realign on their own. To be sure, you should still visit your healthcare practitioner. If the kneecap has not realigned itself, your healthcare professional will realign it. Your knee will be examined with an X-ray to look for any fractures or rips in the ligaments. In addition to physical treatment, your knee may be stabilized using a brace. You might require surgery if your knee has dislocated multiple times, if there is a fracture, or if there is a rupture in a ligament. Physical therapy and the usage of a knee brace will come next.
Patellofemoral stress syndrome (PFSS): RICE is the first line of treatment. You must take it easy on your knee and stay away from anything that aggravates the discomfort. NSAIDs can be used as needed to treat inflammation and discomfort. To prevent further problems and strengthen the muscles supporting the knee, physical treatment is frequently advised. To lessen pain while you exercise, a physical therapist might offer you a knee brace or you how to tape your knee. Moreover, orthotic shoe inserts can support knee stability.
Iliotibial band friction syndrome: The initial steps in treating iliotibial band friction syndrome are resting the affected knee, avoiding activities that exacerbate the discomfort, and applying ice to the outside of the knee. NSAID use can lessen pain and inflammation. Your doctor might suggest cortisone shots if your pain is very bad to lower inflammation. In certain situations, physical therapy is suggested. If various treatments don’t work to improve your health within six months, surgery can be suggested. The portion of the iliotibial band that is rubbing on the femur is surgically removed.
Paresis or paralysis of the quadriceps: The nature and extent of the damage will mostly determine the prognosis. To lessen the consequences of paresis and regain motor and nerve function, physical treatment is advised. Muscle function may be enhanced by a therapy known as neuromuscular electrical stimulation (NMES), in which electrical impulses are used to contract the quadriceps muscles. To support the knee, foot orthotics, and knee braces are frequently utilized. For people who have paresis, assistive equipment like a walker or cane can make moving about safer. The cause of the brain injury may need to be treated with emergency surgery.
compartment syndrome: A fasciotomy, a type of emergency surgery, is required to treat the acute form of compartment syndrome. To quickly release the pressure that has built up in the afflicted quad muscles, the surgeon will make incisions in your skin and the surrounding tissues. Physical therapy will be required after surgery to restore your leg’s strength, flexibility, and range of motion. You will need to apply the RICE approach frequently and take plenty of breaks from physical activity. Complete recovery from compartment syndrome may require up to four months.
Treatment for muscle cramps: You can attempt several techniques to ease the discomfort, such as stretching or massaging the affected area, using a heating pad, and drinking water.
Modifications of the quadriceps tendon during illness
When systemic illnesses are present, skeletal muscle adapts. This indicates that muscle function alters volumes and metabolism, exacerbating the clinical picture.
Aging: The shape and function of the quadriceps muscle are altered due to its adaptation to increasing age. Sarcopenia causes the muscles to lose volume and mass, which weakens their coordination and strength. Denervation procedures outcomes the loss of motor units while the proportion of red fibers rises. Fibrosis procedures and intramuscular fat gain as a result.
Chronic Heart Failure and Chronic Obstructive Pulmonary Disease (COPD): Reduced quadriceps femoris muscle mass, increased connective tissue, and fibrosis phenomena are associated with chronic and ingravescent respiratory disorders such as COPD. These outcomes in a lowering in strength, balance, and contractile capability when walking or standing. Muscle fatigue occurs more quickly as a result of an increase in anaerobic fibers at the expense of oxidative fibers. Along with a localized and systemic metabolic change (increased cardiovascular risk), there is an increase in intramuscular fat. The functional modification of the muscle affects females more closely than males.
Multiple Sclerosis: The quadriceps muscle experiences a loss of bulk and strength as a result of the disease. Anaerobic fibers proliferate while oxidative fibers diminish. White fibers evolve more multiply, but they also experience more significant atrophy. promote fibrosis and intramuscular fat accumulation.
Exercises for the quadriceps tendon
People can work their quadriceps using a range of workouts designed to help build and condition this muscle group. To help promote blood flow to the area, it is advised to warm up and stretch briefly before exercising.
This can involve walking for five to ten minutes, followed by a standing quadriceps stretch or a prone squad stretches, for the quadriceps. To perform this stretch, bend your knee and bring your heel up to your buttocks. After grabbing their ankle, the person slowly brings it closer to their torso and holds it there for 30 to 60 seconds.
Among the quadriceps exercises that people can attempt are
Leg press
Another piece of equipment for the gym is a seated leg press.
Regarding this task: After deciding on a suitable weight, position yourself on the machine with your feet up against the resistance plate.
To move the plate away, flex your quadriceps.
After a brief pause, flex and allow the plate to return in a gradual, controlled motion to the starting position.
Extension of the legs
One type of weight equipment that one could find in a gym is the seated leg extension. A user sits on the machine and places their feet under the bar after choosing the proper weight. After the leg has been straightened, the person can slowly move back to the beginning position by extending their quadriceps muscles.
Squats
Your quadriceps are among the several lower body muscles that squat test and build. Squats also have two other major benefits: you can perform them anywhere and they don’t require any specialized equipment.
To perform this exercise, place your feet slightly wider apart than the breadth of your hips.
As you gradually bring your hips back into a sitting position, shift your weight onto your heels. As you perform this exercise, keep your chest raised and your abdominal muscles tight.
Until your thighs are nearly parallel to the floor, keep lowering your hips. Your glutes and thighs should feel a little tight.
Take a moment to stand with your legs crossed over your toes but not past them.
Exhale, then raise yourself to the beginning posture.
Do this drill ten or twelve times.
Lunges
Lunges, like squats, can assist you in building stronger lower body muscles, such as your hamstrings, quadriceps, and calf muscles.
You can experiment with several variations, such as walking, side, and forward lunges.
Step one in performing a forward lunge: Place your feet hip-width apart. Take a step forward with your right leg and bend your left knee almost to the floor without going all the way down.
To bring the left leg back to its initial position, push through the right foot.
With the other pair of feet, repeat the exercise.
Lunges can also be performed with additional weights or one’s body weight.
Perform 10–12 repetitions for every leg.
Deadlifting
For this exercise to enhance your quadriceps, you will need some equipment, such as a barbell with detachable weights or a set of kettlebells.
Your quads, gluteal muscles, and back muscles are strengthened when you perform deadlifts.
To carry out this task: Place two kettlebells on the floor, slightly outside of each foot, and stand with your feet shoulder-width apart. As you thrust your hips back and bend your knees, contract your abdominal muscles.
As soon as your hands touch the kettlebell handles, sag your hips.
Hold the kettlebells firmly while maintaining a straight back and arms.
Raise your body slowly until you are standing straight up while holding the handles of the kettlebells.
Take a breath, pause, and lower your body until the kettlebells make contact with the ground. Then, stand back up while still gripping the kettlebells.
Do the exercise six to ten times over. You can increase the difficulty of this workout by using larger weights.
Stretches for the quads
Regarding the amount and kind of stretching that is required before jogging or engaging in other forms of exercise, experts can occasionally differ. However, a few light stretching exercises will help you extend your range of motion and loosen up your muscles before and after an exercise session.
Try the basic quad stretch, which involves standing on one leg. For support, you can hang onto a chair or the wall.
Bend your leg at the knee and raise the other foot behind you.
Attempt to place your foot against your buttock.
After a brief period of holding, return your foot to the floor.
The kneeling stretch is an additional effective quad stretch.
Beginning posture of kneeling stretch: While still kneeling, place the left knee exactly under the left hip on the floor (or a stretch mat), and place the right foot in front of the right hip so that the right hip is in a ninety-degree posture and the right knee is immediately over the right ankle. To help keep your spine tall and straight, place both hands softly on your right thigh.
Pull your shoulders back and down without arching your lower back by depressing and retracting your scapulae. Then, “brace” yourself by using your abdominal and core muscles to strengthen your spine and maintain a level and stable pelvis. Maintaining your left knee firmly planted in the ground, bend forward into your right hip.
Keep your pelvis from rotating to the front (forward). Squeeze and contract your left hip’s glute muscles to extend the stretch to your left hip flexors.
For a total of two to five repetitions, hold the stretch position for thirty to forty-five seconds at a time. Try to get a little deeper into the stretch with each repeat, but be sure to keep your core braced to prevent the pelvis from rotating and losing the stretch. After finishing every exercise on one hip, switch to the other.
Exercise Variation: Raise your left arm straight up in the air, slant it slightly to the right, and bend forward into your right hip to intensify the stretch. Make sure to alternate directions to guarantee that the pelvis stays level and to get the most out of the stretch, keep your abdominals tight during the entire exercise. Underneath the knee, use an Air cushion or a rolled-up stretch mat to ease any discomfort.
Summary
A collection of muscles on the front of the leg is called the quadriceps. The rectus femoris, vastus lateralis, vastus intermedius, and vastus medialis are their four separate muscles. They aid in activities like walking and jumping and are in charge of extending the leg. These muscles stabilize your kneecap in addition to being involved in a variety of dynamic actions. Because you utilize your quads for a variety of tasks, They might be prone to accidents. Athletes frequently have quad injuries. People should take it easy after an accident and let their muscles heal. Injuries can be avoided by exercising and extending these muscles properly.
What Is Included in Physiotherapy for the Quads?
The following are the primary physical therapy exercises that are utilized to enhance the health and functionality of your quadriceps:
Strength: Exercises involving the knee and the hip are crucial for enhancing quad strength since the quadriceps muscles cross both the knee and the hip. The quads are the focus of basic knee strengthening exercises, and the quadriceps are also heavily worked in advanced hip strengthening activities.
Flexibility: You may increase the flexibility of your quadriceps muscles by performing a variety of simple stretches. It’s critical to exercise caution and pay attention to your pain to avoid overstretching your knee and reinjuring it.
Balance and proprioception: Since the quadriceps are crucial for maintaining your balance and upright posture, balance and proprioception (body position awareness) workouts frequently target them. While advanced balance exercises can help heal knee pain and quad injuries, basic balance exercises can also assist prevent falls.
The ideal workouts for your particular illness might be recommended by your physical therapist.
Which diseases and illnesses impact the quadriceps muscles?
Strains are the most familiar kind of quad muscle injury. Overstretched muscle fibers result in a strained quadriceps muscle. The rectus femoris is generally affected by thigh strains because it travels two highly dynamic joints.
Strains on the thighs might be minor or severe.
Grade 1: A little rip or overstretch in the muscle fibers. It would help if you even utilized your leg precisely though you could have some modest thigh muscle soreness or edema.
Grade 2: These tears of the quadriceps are more intense. They may outcome in intense discomfort and weakness. probably your leg won’t permit you to carry weight.
Grade 3: Either the muscle tears out from the tendon or the quad tendon breaks, entirely detaching it from your kneecap. Your leg is so painful and puffy that you are incapable of utilizing it. If you have a torn quad muscle, you might detect a deformity beneath the skin.
Who develops ruin to their quadriceps?
Runners, jumpers, and kickers repeatedly suffer from quad muscle ailments. This protects sprinters as well as athletes who partake in softball, basketball, rugby, football, and soccer. Moreover, if you are older than 40, you may experience quad pain which has certain medical disorders, such as multiple sclerosis, diabetes, gout, or rheumatoid arthritis, which should damage tendons.
possess a history of quad injuries.
feel tired in your quadriceps.
own weak hamstrings or quads.
utilize drugs that weaken muscles and tendons, such as corticosteroids.
FAQS
How do you maintain the health of the quad muscles?
To take care of your quadriceps, avoid pushing through pain in your legs, hips, or knees.
resting your quadriceps after working out or exerting yourself.
Warming up and stretching your quadriceps before a workout
How frequent are injuries to the quadriceps?
Injuries to the quadriceps are uncommon. Approximately 1 in 10,000 athletes may maintain a thigh strain, according to collegiate athletes. Injuries to the hamstrings, which are discovered at the rear of the thigh, are more familiar.
Is the tendon of the quadriceps flexor or extensor?
The quadriceps extends the knee joint through the extensor mechanism, which includes the patella, ligamentum patellae, and quadriceps tendon. The contraction of the quadriceps plays a crucial role in stabilizing the knee joint. Without it, when bearing weight, the knee tends to bend.
Which name do you give the quadricep tendon?
The portion distal to the sesamoid bone is referred to as the patellar ligament (ligamentum patellae), patellar tendon, or infrapatellar tendon. It passes through the quadriceps tendon or the suprapatellar tendon.
What is the physiology of the quadriceps tendon?
The rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius muscles are the four quadriceps muscles whose tendinous fibers merge to form the quadriceps tendon. It is 35 mm wide and 8 mm thick on average.
Which two structures is the tendon of the quadriceps connected to?
The patella, or knee cap, is where the quadriceps tendon, which later forms the patellar ligament, connects to the shin from all four segments of the quadriceps muscle. The patella, which is attached to the shin from below by the patellar ligament, is where the quadriceps are attached to the patella.
To which muscles does the quad tendon attach?
When the quadriceps muscle group was dissected, it was discovered that a fifth muscle component—the tensor vastus intermedius—consistently fused into the quadriceps tendon in addition to the rectus femoris, vastus lateralis, vastus intermedius, and vastus medialis.
Does a quad tendon grow back?
The quadriceps tendon has the same capacity for complete regeneration following harvest as the patellar tendon.
Why repair an ACL with a quad tendon?
The quadriceps tendon has become more and more popular as a source of graft for ACL restoration in recent times. Compared to other autograft options, the all-soft tissue quadriceps graft has several advantages. Compared to the patellar tendon (PT), it possesses 20% more collagen fibrils per cross-sectional area histologically.
References
- Quadriceps femoris muscle. (2023, November 3). Kenhub. https://www.kenhub.com/en/library/anatomy/the-quadriceps-femoris-muscle
- Waligora, A. C., Johanson, N. A., & Hirsch, B. E. (2009, August 19). Clinical Anatomy of the Quadriceps Femoris and Extensor Apparatus of the Knee. Clinical Orthopaedics and Related Research. https://doi.org/10.1007/s11999-009-1052-y
- Professional, C. C. M. (n.d.). Quad Muscles. Cleveland Clinic. https://my.clevelandclinic.org/health/body/22816-quad-muscles
- Pt, B. S. (2023, June 5). The Anatomy of the Quadriceps Muscles. Verywell Health. https://www.verywellhealth.com/what-are-the-quadriceps-muscles-2696379
- Quadriceps Muscles: Anatomy & Function – Knee Pain Explained. (n.d.). Knee-Pain-Explained.com. https://www.knee-pain-explained.com/quadriceps-muscles.html
- Morales-Brown, L. (2023, December 6). What to know about the quadriceps muscles. https://www.medicalnewstoday.com/articles/quadriceps-muscles
- Quadriceps Muscle. (n.d.). Physiopedia. https://www.physio-pedia.com/Quadriceps_Muscle
- What to Know About Your Quadriceps Muscles. (2020, June 16). Healthline. https://www.healthline.com/health/quadriceps