
Occipital Neuralgia
Table of Contents
What is a Occipital Neuralgia?
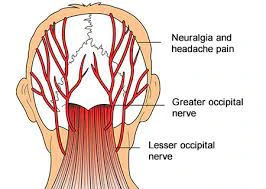
- Occipital Neuralgia with unilateral pain that starts in the neck. Occipital neuralgia is a distinct type of headache symptom-wise by piercing, throbbing, or electric-shock-like chronic pain in the upper neck, back of the head, or back of the ears, usually on 1 side of the head. A common chronic or recurrent headache usually starts after neck motion. It is usually situated with a reduced range of motion (ROM) of the neck. Occipital Neuralgia was 1st introduced by Sjaastad et al.(1983).
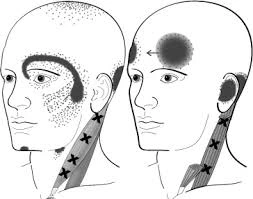
- It is a chronic headache that begins from the atlantooccipital or the upper cervical joints or is perceived in 1 and more regions of the head or face. Some individuals will also feel pain in the scalp, forehead, or back of the eyes. Their scalp might also be tender to the touch, or their eyes especially sensitive to the light. The position of pain is related to the areas supplied by the greater or lesser occipital nerves, which travel from the area where the spinal column communicates with the neck, up to the scalp at the behind of the head.
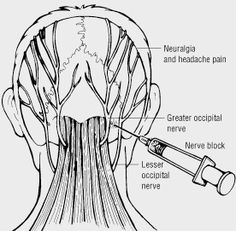
- The pain occurs because of irritation and injury to the nerves, which might be the result of trauma to the back of the head, pinching of the nerves by more tight neck muscles, compression of the nerve as it leaves the spine due to osteoarthritis, and tumors or the other types of lesions in the neck. Localized inflammation and infection, gout, diabetes, blood vessel inflammation (vasculitis), or frequent lengthy periods of maintaining the head in a downward or forward position are also situated with occipital neuralgia. In many cases, however, no cause will be found. A positive response (relief from pain) after an anesthetic nerve block will work as a confirmation of the diagnosis.
Definition Occipital Neuralgia
- Occipital neuralgia is a well-defined type of cervicogenic headache characterized by piercing, throbbing, or electric-shock-like chronic pain in the upper neck, back of the head, or back of the ears, generally on 1 side of the head. Typically, the pain of occipital neuralgia starts in the neck or then spreads upwards.
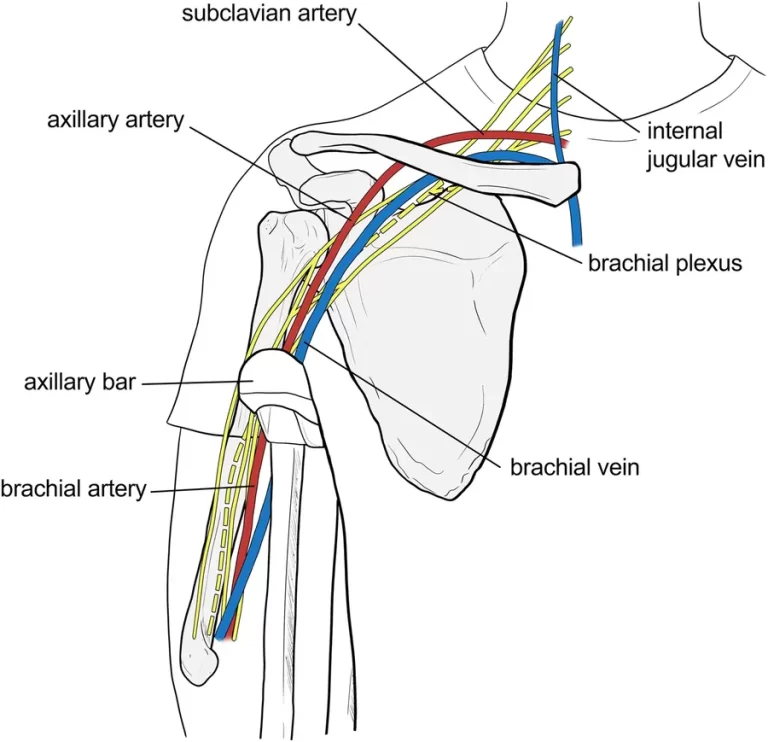
Clinical relevant anatomy of the cervical spine
Anatomy of Occipital Neuralgia
- The cervical spine is an important 1 anatomically, clinically, or therapeutically.
- It is the area where the nerves of arms originate through the brachial plexus or where the cervical plexus forms providing nerve supply to the diaphragm surrounded by different structures.
- It also allows the opening of quite important vascular structures to reach the brain or allows the joining place for muscles that move into the head, neck, or shoulder girdle.
- To engulf this complicated region, we will consider the bony structures 1st, or after that discuss the ligaments, nerves, or musculature that are situated in this area of the cervical spinal column, arriving at the conclusion with some clinical implications of damage to a few of these structures.
- The cervical spine consists of seven vertebrae, C1 to C7, the cervical nerves from C1 to C8, muscles, or ligaments.
- The first 2 vertebrae C1 or C2 have unique shapes or functions. They form the upper cervical spine.
Upper Cervical Spine
- The cervical spine is made up of seven vertebrae, C1 to C7.
- In that, the first 2 vertebrae C1 or C2 create the upper cervical spine.C1 to C2 have unique shapes or functions.
Nerves
- Many important nerves originate from the cervical spinal cord.
- Most of these nerves arise in 1 of 2 plexuses: The cervical plexus and The brachial plexus
- C1 (Atlas) vertebrae assist the skull. It articulates superiorly with the occiput which is termed the atlantooccipital joint.
- The atlanto-occipital joint is responsible for 33% of flexion or extension. The structure of the atlas allows forward or backward motion of the head.
- Below the C1 (atlas) is the C2 (axis) which is responsible for the rotation. This joint (The atlantoaxial joint) is responsible for 60% of all cervical rotation.
- C3-C7 cervical vertebrae that made up the lower cervical spine, are the same as each other but very different from the C1 or C2.

SPINAL NERVES
- Certain spinal nerves are included in Occipital Neuralgia. Spinal nerves are signal transmitters that give the communication between the brain and the body through the spinal cord. At every level of the cervical spine is a set of spinal nerves; 1 on the right side or another 1 on the left side of the spine. C1, C2, and/or C3 might be involved in the development of Occipital Neuralgia because these nerves allow function (motion) or sensation of the head or the neck. Nerve compression can also cause inflammation or pain.
Pathophysiology
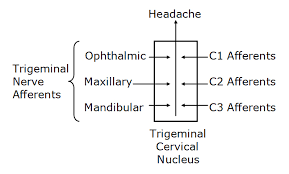
- The C1-C3 nerves collect the pain signals to the nociceptive nucleus of the head or the neck(the trigeminocervical nucleus). Aseptic inflammation or the neurotransmission within the C-fibers because of cervical disc pathology is thought to begin or worsen the pain in Occipital Neuralgia.
- The nociceptive nucleus of the head or the neck(the trigeminocervical nucleus) collects afferents from the trigeminal nerve as well as the upper 3 cervical spinal nerves. Neck trauma, whiplash injury, strain, and chronic spasm of the scalp, neck, and shoulder muscles can raise the sensitivity of the area which is the same as the allodynia(Pain due to a stimulus that will not normally provoke pain) that is seen in later chronic migraines. A lower pain threshold makes patients near to more severe or chronic pain. Because of that early diagnosis or therapeutic intervention are very necessary.
Epidemiology
- It is a rare chronic headache in people who is between 30 to 45 years of age.
- According to NCBI(national center for biotechnology information), a prevalence of 4.1% was located. In 41 cases with the highest number of Occipital Neuralgia criteria, there was a male prevalence (F/M: 0.71). While occipital neuralgia traits (mechanical precipitation etc.) were normally present in Occipital Neuralgia, ‘migraine traits’, like nausea, vomiting, or throbbing seem to be rarely present. In 97% of the cases, pain exacerbations start in the neck or the occipital area.
Which are the Causes of Occipital Neuralgia?
- Many things can be the reason for Occipital Neuralgia.
- Occipital Neuralgia can come from problems with the cervical vertebrae, joints, and neck muscles. e.g.people in certain jobs, like carpenters, truck drivers, or hair stylists can get Occipital Neuralgia from the way they hold their head or neck when they work. Some people who hold their heads out in front of their bodies are also caused by Occipital Neuralgia. This movement is known as “forward head movement,” as it puts extra stress on the neck or the upper back.
- It seems to be referred pain begins from irritation caused by cervical structures nerves supplied by the upper 3 cervical spinal nerves C1, C2, or C3; therefore, any structure nerve supplied by the C1 to C3 spinal nerves could be the source of an Occipital Neuralgia. The cause of Occipital Neuralgia is often related to more tension in the neck. The headache might result from cervical spondylosis, a damaged disc, and whiplash-type motion that irritates a cervical nerve, and sometimes over-activity of neck muscles also cause Occipital Neuralgia because of spasm of para-spinal neck muscles.
- The facet joints of cervical vertebrae (neck bony structure) or the neck muscles also contribute to the development of an Occipital Neuralgia
Medical conditions which can be responsible for Occipital Neuralgia are :
- Whiplash and another injury to the neck
- Poor Posture
- Fractures
- Cervical Disc Prolapse
- Tumors in the Cervical region
- Cervical spondylosis or osteochondritis are not accepted as a cause of Fractures.
- Infections
Symptoms of Occipital Neuralgia
- Occipital Neuralgia is pain that arrives from a sudden movement of the neck.
- Another is that you get headaches when the neck holding in the same position for some time.
Symptoms of Occipital Neuralgia may include
- pain on 1 side of the face
- a reduced range of motion (ROM) in the neck
- pain near the eyes
- pain or stiffness of the neck
- Pain radiate from the Upper trapezius muscle to the shoulder or sometimes arm region.
- Spasm of Paraspinal Neck Muscles
- pain while coughing and sneezing
- pain in the neck, shoulder, and arm on the affected side
- Throbbing head pain
- Headache which is triggered by certain neck movements and postures
- Weakness in the deeper neck flexors
- sensitivity to light or noise
- Nausea
- Tenderness in the Upper Cervical area
- Poor Posture
- Blurred vision
Other signs may include
- Steady pain
- Pain on 1side of the face
- An Occipital Neuralgia pain that can last for hours and days
- When you cough, sneeze and take a deep breath cause headache
- Pain that stays in one spot, like the back, front, and 1 side of the head
- Stiff neck (you cannot move the neck normally)
- Even though Occipital Neuralgia or migraine is different but some of the symptoms will be similar.
- For example, you may:
- Throw up
- Feel sick to the stomach
- Feel uncomfortable in bright light
- Have pain in the shoulder or arm
- Have blurry vision
- Some people get Occipital Neuralgia or migraine at the same time.
- Feel uncomfortable with loud noise
Risk Factors of Occipital Neuralgia
Risk factors that may be aggravated Occipital Neuralgia include:
- Muscular stress
- Fatigue
- Current and prior neck injuries
- Cervical disc problems
- Sleep difficulties
- Poor posture (High cell phone use)
How do doctors diagnose Occipital Neuralgia?
- Diagnosis of Occipital Neuralgia involves ruling out other conditions.
- Diagnosis also includes testing for movement or ruling out the affected nerves, bones, or muscles.
- For diagnosis, the doctor will start by questioning some questions regarding the symptoms.
- Then, they will run through a set of special tests.
- All of this assists the doctor to rule out if the nerves or spinal cord are under too much pressure.
- The doctor will perform a physical examination to find the cause of the neck pain and other symptoms.
Physical examination:
- Pain localized in the neck or occiput, which can spread to other regions in the head, such as the forehead, orbital region, temples, vertex, and ears, generally affected side. Pain is the trigger and is aggravated by specific neck motions and sustained postures.
At least one of the following:
- Changes in neck muscle texture, tone, shape, and reaction to active or passive stretching or contraction
- Abnormal tenderness of neck muscle
- Limitation of passive neck movements
Radiological examination:
Radiological examination discloses at least 1 of the following:
- Abnormal posture
- Movement abnormalities (flexion/extension)
- Congenital abnormalities
- Fractures
- Rheumatoid arthritis
- Other distinct pathology (not spondylosis and osteochondrosis)
- Bone tumors
Flexion rotation test
- The inverse relationship between headache severity of OC (Occipital Neuralgia) distinct pathology (not spondylosis and osteochondrosis) or ROM (range of motion)towards the more restricted side for the Cervical Flexion rotation test (FRT) was statistically relevant for all patients with Occipital Neuralgia (Sn = 0.91, Sp = 0.90). The patient might feel no pain at the time of the FR test. During the test, the neck of the patient is passively held in end range of flexion. The therapist rotates the neck to both sides until they feel resistance and until the patient says they are in pain. At this endpoint, the physical therapist will make a visual approximation of the rotation range or says on which side the FRT was positive and negative. The test was considered positive when the approx range was reduced by more than 10° from the anticipated normal range (44°).
Other tests are:

- X-ray: X-rays will help to know about degenerative changes to the spine (cervical spine) or the problems like bone spurs.
- Computed tomography (CT): A CT scan is an imaging technology that uses multiple X-ray images to see the neck or spine in different “slices.”
- Magnetic resonance imaging (MRI): An MRI scan is used with powerful magnetic or radio waves to generate highly detailed images of bone or soft tissues, including those of the spinal cord.
- Blood tests: A complete blood count (CBC), erythrocyte sedimentation rate (ESR), or a C-reactive protein (CRP) test can assist to determine if inflammation and infection are present.
- In a myelogram, a dye injection highlights a few areas of the spine. CT scans and X-rays are used to provide more detailed images of affected regions.
- . A nerve conduction study (NCV) checks the speed or strength of the signals sent by nerves. This is done by putting electrodes on the skin where the nerve is supplied in the muscle.
RED FLAGS
- An aggravate design of a pre-existing headache in the non-presence of obvious predisposing factors
- Sudden onset of a severe headache
- If the headache is situated with focal neurologic signs other than a typical aura
- If the headache is situated with fever, neck stiffness, skin rash, or a history of cancer, HIV, and other systemic illness
- New onset of a headache during the pregnancy
- Moderate and severe headache aggravated by cough, exertion, and bearing down
Patients with 1 or more red flags must be referenced for an immediate medical consultation or further investigation.
Differential Diagnosis
Distinguished from serious pathology such as:
- Cervical Myelopathy
- Cervical Instability
- Vascular Pathologies of the Neck
- Intracranial Pathology
- Cervicogenic Headache
Prognosis of Occipital Neuralgia
- Occipital neuralgia is not a serious life-threatening condition. Many persons will increase with therapy involving heat, rest, anti-inflammatory medications, or muscle relaxants. Recovery is commonly complete after the bout of pain has ended or the nerve damage repaired and lessened.
Treatment of Occipital Neuralgia
Medical Treatment
- There are numerous ways to decrease the pain, and get rid of it completely:
Medicine:
- Non-steroidal anti-inflammatory (NSAIDs) such as ibuprofen, muscle relaxers, or other pain relievers might relieve the pain.
Nerve block:
- This might temporarily ease the pain or help you better work with physiotherapy.
Spinal manipulation
- This is the coordination of massage, physiotherapy, or joint motions.
- It should only be done by a chiropractor, a physiotherapist, and an osteopath.
Other options:
- Non-surgical ways to cure the pain consists of relaxation techniques, such as deep breathing, yoga, or acupuncture.
Physiotherapy treatment of Occipital Neuralgia
- The doctor may give reference to you a physical therapist for treatment or also help to ease the neck pain.
You can try many things at home if the condition is mild
- Rest
- Take an over-the-counter(OTC)pain reliever, such as non-steroidal anti-inflammatory drugs (NSAID) or acetaminophen (Tylenol), which consists of ibuprofen or naproxen sodium.
- Use a hot pack and a cold pack on the neck for 7-10 mins which help to ease the pain.
- Exercise daily to help you recuperate faster.
- Wearing a cervical collar to limit motion or to provide a support
- In moderate conditions, you may prefer a physiotherapist.
Pain management
- Treating occipital neuralgia with Electrotherapy.
- Some people respond well to treatments like OTC (over-the-counter) pain medications and physiotherapy, some people might need other solutions for curing their pain.
- Electrotherapy might effective for pain management.
What is Electrotherapy?
- Electrotherapy uses light electrical pulses to stop the pain on a point surface of the body. Commonly, all of these therapies use a device with electrodes to transmit a low-voltage electrical current to pain surfaces.
- The primary goal of electrotherapy is pain management.
Uses of electrotherapy
- It can assist to improve blood circulation, which boosts the body’s healing process.
- This might also help to strengthen muscles, stimulate bone growth, or repair damaged tissues.
- Moreover, electrotherapy may raise the motions or function in an affected portion.
- These are the lower-voltage electrical currents, a person commonly only feels a tingling sensation.
- Some people even feel that using an electrotherapy machine for a relaxing purpose.
- The adverse effects of electrotherapy are generally mild or not.
- The most generic side effect patients tell is skin irritation because of the adhesive tape on the electrodes to stick it onto the skin surface. Many times a feeling of burning sensation on the area of the skin because of not using the device properly.
Electrotherapy Modality
Here are some common types of electrotherapy that the physiotherapist may prefer:
TENS (Transcutaneous Electrical Nerve Stimulation)
- One of the most commonly used electrotherapy devices is used for pain decrease. Small or sticky pads with electrodes are put over and near the area where a person senses pain. The physiotherapist will decide the surface of the placement of electrodes. A series of low-voltage electrical currents are transmitted by the battery-operated unit to the area. You will be raised and decreased the electrical current as well as the frequency or the patterns of stimulation by using the controller.
PENS(Percutaneous Electrical Nerve Stimulation)
- An alternative option to the TENS is PENS (percutaneous electrical nerve stimulation) uses a needle on the behalf of pads to transmit electrical currents. It will work as acupuncture with electrical stimulation. The benefits of using needles rather than pads mean the pulse of the electrical current is nearer to the pinched nerves or the muscles. This can help to ease pain immediately in many patients.
- Commonly, this therapy is used as an outpatient procedure. A person can also use a PENS device at the home.
PEMF (Pulsed Electromagnetic Field Therapy)
- It takes a varied process to use electricity for pain easing. PEMF tries to heal at the cellular level rather than treating nerves and muscles. Specialized coils generate an electromagnetic field surrounding part and all of the body during the whole treatment. These electromagnetic waves stimulate the cell’s electrons or help in the healing process or stimulate bone growth.
- PEMF treatments will recover the cells or make them more active in healing, rebuilding, or fighting disease. Treatment occurs in a therapist’s clinic. Some PEMF products might be purchased for home care use.
Cervical traction
- Cervical traction help to ease the pain. It includes using weights to raise space between the cervical joints or also easing the pressure on the cervical discs or the nerve roots.
- Chiropractic manipulation might help to decrease severe pain
- Different forms of physiotherapy, consist of the application of heat or cold therapy, traction, and exercise.
Strengthening Exercises for Occipital Neuralgia
- Strengthening exercises for neck muscles including deep neck flexors or the upper quarter muscles
- Cervical spine mobilization techniques
- C1-C2 Self-sustained Natural Apophyseal Glide (SNAG) has shown to be effective for decreasing the Strengthening exercises for neck muscles consisting of deep neck flexors or the upper quarter muscles symptoms
- Thoracic spine thrust manipulation or exercise
- Upper cervical spine mobilizations
- Active mobilization exercises
- Work-related ergonomic training
- Passive mobilization with movement
- Thoracic Manipulation
- Deep Neck Flexor Exercise
- Active mobilization with movement
Trigger Point Therapy
- This is the combination of the different manual approaches, e.g., compression, stretching, and transverse friction massage. Pressure decreases over the sternocleidomastoid muscle. Pressure is given slowly and progressively to raise over the trigger point until the finger encountered a raise in tissue resistance (tissue barrier). This pressure is held until the therapist feels relief from the stressed band. At that time, the pressure is increased again until the next increase in tissue resistance. Stretching of the tight band muscle fibers is also necessary. Trigger point therapy is working for lengthening the trigger point in the muscle or the situated connective tissue. The physiotherapist gives moderate slow pressure over the trigger point or slides the fingers in alternate directions.
- This manual therapy is applied gently and calmly or is performed without inducing pain in the patients.

Co-contraction of the Neck Flexor or Neck Extensor
- It is facilitated with neck rotation or the neck exercises are illustrated once the patient can activate the deeper muscles.
- The patient will perform a self-resisted isometric rotation in the correct sitting position. They look into the palm or allow the resistance to facilitate the muscles or to perform the consecutive rhythmic to or fro stabilization exercises with an importance on the slow onset or slow-release maintaining contractions, by using resistance to match about a 10–20% effort. Retrain the strength of the superficial or the deeper flexor synergy.
Extensors of the Craniocervical Spine

- The patient exercises the eccentric control of the head into the flexion occurring by the concentric control of the back to the neutral position in a four-point kneeling position to train the coordination of the deep or superficial cervical extensors. These exercises are done with re-education of the scapular muscles in these positions or begin in the program. The exercise is gradually been progressed by performing varying small ranges of craniocervical extension or flexion while holding the cervical spine in a normal position.
Tucked in Exercise
- The patient’s position should be Sitting straight & look straight ahead with the ears level parallel over the shoulders joints.
- Place 3 to 4 fingers on the chin.
- Maintain the finger, pull the chin & head extended beside up to a slow stretch is felt at the bottom of the base of the head & top of the neck.
- Maintain or hold for 5 to 10 secs. Repeat seven to ten times.

Neck flexion Exercise (Neck tilt)
- In Relax sitting position flex the head down to rest the chin on the chest (Flex the neck fully).
- Gently tense the neck muscles & hold for 4 to 8 secs.
- Return to the initial position & repeat seven to ten times.
Neck retraction exercises
- Sit on soft ground or a chair & then engage the core to help stabilize the spine.
- Brace the posterior muscles in the neck to bring the head back into a steady position while having the chin slightly downward.
- Maintain the position briefly.
- Relax & then repeat.
- Start with 1 set of 5 reps and work the way up to ten reps in total.
Isometric Neck extension exercise
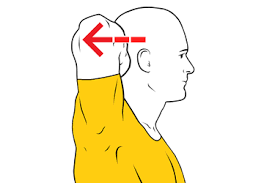
- In Relax sitting position without arching the back, slowly move the head backward so you are looking upward.
- Hold for 5 to 10 secs. Return to starting position.
- This is a good exercise to do during working hours to prevent neck strain.
- Gently tense the neck muscles & hold for 5 to 10 secs.
- Return to a neutral position & repeat 10 times.
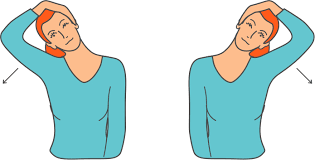
Neck flexion Exercise (side to side)
- Flex the head down towards the shoulder, & try to touch the shoulder with the ear (Without elevating the shoulder).
- Gently tense the neck muscles & hold for 8 secs.
- Return the head to a neutral position & repeat in the opposite direction.
- Repeat 10 times on both sides.
Isometric Neck Rotation exercise

- Begin this exercise by doing a rotation of the head towards 1 side, keeping the chin at the same level & moving within normal limits.
- Slowly stretch the neck muscles & hold for eight secs.
- Back the head to the neutral position & repeat in the other direction.
- Repeat 10 times on each side.
Re-education of the cervical flexors for anti-gravity function in a sitting position
- This re-education of the cervical flexors is a controlled eccentric action of the neck flexors onto the cervical extension range obeyed by a concentric action of these muscles to back the head to the normal erect position. The back to the correct position surely is initiated by CCF (craniocervical flexor), nor then a dominant action of the SCM (sternocleidomastoid).
- The exercise is gradually progressed by gently and slowly raising the range to which the head is moved into extension as control improves, or by introducing isometric holding through the range.
Prone Cobra Exercise

- This exercise is start by lying face downwards on the ground & assists gravity as resistance in the process.
- Put the face downwards on the floor, and put the forehead on a wrapped-up hand towel for support.
- Put the arms by the side, & palms downwards on the surface.
- Drag the tongue onto the upper palate of the mouth.
- Squeeze the shoulder blades combine & elevate the hands off the ground.
- Roll the elbows inside, palms outsides, & thumbs upside.
- Smoothly raise the forehead about an inch off the towel maintaining the eyes looking ahead forward at the ground
- Maintain the position for seven to ten secs.
- Do seven to ten reps.
Retrain the Scapular Muscles

- Retrain scapular muscle which is oriented in posture betterment strategy is to have the patient movable the coracoid upward or the acromion backward, which ends in a slight retraction or the external rotation of the scapula. The aim is to facilitate the coordinated motion of all parts of the trapezius or the serratus anterior muscles, allowing the lower trapezius to little bit depress the medial portion of the scapula, consequently easing the levator scapulae.
- Once the patient habituates the correct scapular orientation, re-educate the endurance capacity of the scapular stabilizers again and again reps of 10-sec hold of the corrected scapular position to enhance the early endurance retraining. The endurance of the middle of the lower trapezius muscles is also educated by accomplishing an exercise in the prone lying position opposite the effects of gravity.
- Retrain scapular control is mannered with arm movement or load. This is necessary when activities such as computer work and desk work trigger pain. The patient is inspired by retaining their newly learned scapular position while doing small range (+/- 60 degrees) arm motions, for example, while working at a computer. Scapular control in coordination with control of cervicothoracic postural position is also trained for functional activities such as lifting or carrying objects.
Isometric Neck Exercise
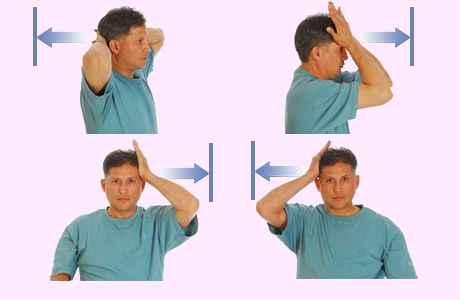
- Isometric neck exercises assist to strengthen the neck muscles. This exercise is mostly prescribed by Physiotherapists from day one to relieve Neck pain.
Isometric Neck Exercise
How to perform this exercise In a sitting alignment, - keep the Body steady and straight, Place both hands beside the neck (as seems in the images), & try the neck to push compress on the hands & At the same time Resist the neck muscles, both hands steady and align pattern for 4 to 5 secs & then relax.
- The first day does 8 reps & the 2nd day does 10 reps. Do some exercise on the forehead & each side of the neck.
- Do the exercise by compressing the side of the head. Repeat 8 times, then opposite sides.
Anterior stabilization lying head lift and rotation
- Lie flat on the back & then place the fingers slightly beneath the jaw till you feel the front neck muscles.
- Smoothly tuck in the chin or slightly lift the head about 1cm off the floor. Then slightly rotate the neck a few cm to each side slowly.
- Depending on the individual type of fitness, maintain the position for a minimum of 2 secs up to 5 secs per rep. Aim for 5 to 10 reps at a time in sets of 2 to 3.

Superman Exercise
- Do this exercise on a mat or a firm floor. Sleep down flat on the stomach while the arms are extended outside straight of the body.
- The legs should be maintained flat on the ground, as well as the arms.
- Lift the arms or the legs simultaneously like you are trying to fly. squeeze the lower back. Make sure to respiration occur properly.
- Depending on the individual type of fitness, maintain the position for a minimum of 2 secs up to 5 secs per rep. Aim for 5 to 10 reps at a time in sets of 2 to 3.
- Individual fitness levels will determine how many reps or sets the individual is capable of doing at a single time or in a single day.
Chin to chest Exercise
- Get into a sitting position on the ground. Put 2 hands at the base of the head with fingers interlocked.
- Staring the thumbs down or the elbows extended ahead.
- Do the head down to the chest or just hold it for 20 to 30 secs.
- Do ten reps of this exercise.

Head lifts
- You are Lie flat on the back with the arms stretched to the sides.
- Nod the head & tuck in the chin.
- Hold this exercise for a few seconds before releasing back to a neutral position.
- Hold this exercise position for 10 seconds.
- Perform the 10 times in 1 session & 3 sessions per day.
Upward Plank Exercise

- This pose allows you to passively hang the head back & down, releasing tension in the neck & shoulders. This lengthens & stretches the longus capitis, SCM, chest, & shoulder muscles.
- Make sure the back of the neck is fully relaxed to avoid compressing the spine. If it is uncomfortable for you to let the head hang back, you can tuck the chin into the chest & lengthen the back of the neck. Precise on engaging the neck muscles without straining.
- You can also allow the head to rest back on some type of support such as a chair, a wall, or stacked blocks.
- How to do- Come into a seated position with the legs straight in front of you.
- Press the palms to the floor alongside the hips.
- Lift the hips & bring the feet under the knees.
- Deepen the pose by straightening the legs.
- Open the chest and & let the head drop back.
- Hold for up to 30 secs.
- Do this pose up to three times.
Upper Quarter Strengthening Exercises
- Middle Trapezius Strengthening
- Lower Trapezius Strengthening
- The addition of upper quarter exercises in the treatment plan for patients with cervical dysfunction is necessary to integrate ‘global’ muscles that have relations to the cervical spine through an anatomical chain.
Trapezius Strengthening exercise
- First, place the knee joint on a bench or chair.
- Try to lean forward so that the hand is reached the bench and also help to support the weight.
- The other hand is placed at the side and palm facing the body.
- Try to raise the arm and rotate the hand to the thumbs-up position.
- Stop this exercise when the hand is at shoulder height and the arm is parallel to the floor.
- Slowly lower the arm to the original position for a count of five.
- Do this exercise two to three times per day.
- Do the exercise by pressing on the side of the head. Repeat eight times, then on other sides.
Trapezius Diagonals exercise
- The patient stands with theraband lower their opposite foot
- While grasping theraband, move shoulders up and down
- With your hand at your opposite hip, slowly raise it beyond
- your body, as if you’re pulling a blade
- Hold 3 seconds and repeat 10-15 times
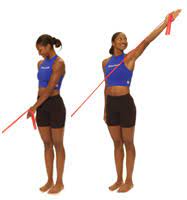
Lateral Raises exercise
- Stand with the arm at your side with the elbow straight and the hands twisted so that the thumb’s face is ahead.
- put up the arm straight out to the side, palm downward, until the hands reach the shoulder position.
- Do not put up the hands forward than the shoulder. Pause and slowly down the arm.
- Perform 3 sets of 10-15 repetitions. for progression do this exercise with a dumbbell
Upright row exercise
- This is a common exercise for strengthening the trapezius. You can also try this exercise with dumbbells or a therabend in your hands.
- Stand up straight.
- With your fists held, pull up your fists as high as you can while bending your elbows, keeping your hands close to the front of your body. Hold for a count of ten.
- Release your arms back into a relaxed position, fists still hold
- Reprise 20 times.
Push-up exercise

- lying face down on the floor, positioning your hands slightly wider than your shoulders.
- Don’t lock out the elbows; keep them slightly bent.
- your legs should be straight back and balanced by your hands and toes. raise your body off the floor and back to starting position,
- 10-12 times.
Reeducate the Strength of the Superficial or the Deep Flexors Synergy
- The head raised must go 1st with CCF (craniocervical flexors) followed by cervical flexion to just raise the head from the bed. Gravity or the head weight gives resistance. Precautions must be taken that high load exercise is not taught too early, as it may be exaggerated the symptoms.
Re-education of Posture
- Posture is an attitude that is assumed by the body or an indirect measure of the functional position of the neuromuscular system
- The postural position is educated in a sitting position or is corrected from the pelvis.
- A different aspect of the training of postural position is the correction of the scapular position.
- The stability of a correct scapular position with significant muscle coordination has been the added benefit of creating reciprocal relaxation in the muscles.
Sensory-motor Training
- Because occipital neuralgia is believed to be a dysfunction of the sensorimotor system. Sensorimotor training consists of progressive exercise on unbalanced surfaces to promote reflexive stabilization or postural stability. Unbalanced surfaces such as exercise balls can be used to add more challenge to the cervical spine as well as the whole body for stability exercises. These end stages of the rehabilitation program for occipital neuralgia patients might be progressed toward functional activities to back the patient to fully participate.
Neck Strengthening with thera-band
- These technics were basically posted isometric relaxation procedures (A) myofascial mobilization, or (B) selected elements of McKenzie therapy. Exercises were primarily given to the muscles with Trigger points, showing a pathological rising in the EMG amplitude. When relaxation is painful, tensed muscles are achieved, and the next step of treatment includes strengthening exercises of the neck muscles. All of the exercises are done under the supervision of a physiotherapist. Exercise intensity shall not raise the pain sensation in the cervical spine, and the shoulder girdle muscles. They aren’t responsible to provoke the headache.
- There are isometric exercises with a gently loading raising or dynamic exercises. Elastic thera bands are most generally used during these kinds of exercises. Additionally, the self-control exercises of the correction of the body posture are done out in front of the mirror relying on visual feedback.

Theraban Rows
- First Place the theraband around a doorknob & tie a knot in the theraband & close it in the door.
- The band is at head or chest level.
- You are sitting straight with each end of Theraband behind the head and the knee joint slightly bent, abdominal muscles tight.
- Must be Maintained the tight trunk muscles and then pull the head back while squeezing the shoulder blades together or combined.
- You are trying to focus on squeezing the shoulder blades without shrugging the shoulder joint up towards the ears.
- Then return to starting position but Do not lean back.
- Hold this exercise position for 10 seconds.
- Perform the 10 times in 1 session & 3 sessions per day.
Preventive Measure of Occipital Neuralgia
- Maintaining a good posture while sitting and driving ( sitting tall with shoulders back or without protruding the head forward)
- Using a helping travel pillow on the plane and bus to avoid unnecessarily side-bending and flexion
- Avoid poor postures and motions that increase pain to start
- Using a neck brace or collar (soft collar) might be helpful while sitting upright and sleeping in a chair
- Avoid tummy-sleeping posture
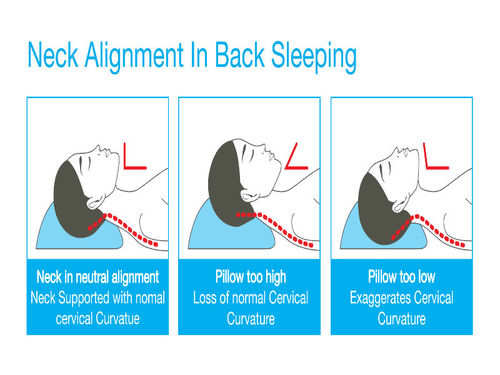
- Find the proper pillow to avoid the head from being too high and too low while during the time of sleeping.
Prevention while sleeping
How to select the proper pillow for Occipital Neuralgia?
- The best pillow for neck or shoulder pain is firm enough to maintain the head at a correct angle but soft enough to ease the pressure points. Many people find comfort with either memory foam, latex, buckwheat, and feather pillow, as these kinds of materials give the best balance of support or pressure relief.
1. Cervical pillows for neck pain relief
- Cervical pillows especially give neck support or keep the spine in proper posture while you are asleep. It’s elevated where the neck is more compressed than the head lies. The pillow works ergonomically to support the neck. Cervical pillows come in various shapes or materials according to comfort.
- If you are changeover from a normal regular pillow to a cervical pillow, you might feel discomfort for some days. Using it each day for taking a short rest during work can adapt easily.
2. Pillows that place on the neck for back sleepers
- Choosing the right pillow for the neck depends on how you sleep. If you sleep on the back, try to choose a pillow that molds to the head or neck so that the neck is enough to support. Memory foam pillows and water pillows are better choices for back sleepers. They keep their shape but adjust according to the body.
3. Firm pillows for side sleepers
- If you sleep on the side, then choose a firm pillow. Place the bulk of the pillow beneath the neck rather than the head, which gives proper support to the spine.
- It assists if the pillow has elasticated. A pillow with a elasticate is 1 with extra material in it, with the join into rectangular panels on all 4 sides of the pillow so that the cushioning adjusts when you move the head. A pillow without a elasticate has only 2 pieces, a top or a bottom that are stitched combined. Side sleepers are also required to put a pillow under their legs to help maintain spine posture.
4. Thin pillows for stomach sleepers
- When you are sleeping on the stomach you put stress on the back. So, you have to use a thin pillow and no pillow to avoid stress on the back. Also, use a thin pillow beneath the abdominal area that can help to reduce the stress on the back.
5. Horseshoe pillows when traveling
- When you are traveling by car, plane, and train, a horseshoe pillow is great support for the neck.
- If you have neck pain, do not let the head bend to the side when you sleep during traveling. Make sure the neck is supported.
FAQs
What Triggers Occipital Neuralgia?
Occipital neuralgia is most commonly occured by the pinched nerves in the root of a individual’s neck. Sometimes this is caused by the neck muscles that are very tight in a individual’s neck. In few cases, it can be caused by a head and neck injury. Long term neck muscle tension is also an common cause.
Is Occipital Neuralgia Serious?
Occipital Neuralgia is not an life threatening condition, but it might have a major impact on the overall quality of the life. It might develop pain that interferes with daily activities of life or it may prevent you from enjoying time with family and friends.
How Do You Know That You Have Occipital Neuralgia?
The primary symptom of trigeminal neuralgia is sudden attacks of severe, sharp, shooting facial pain that last from a few secs to about two mins. The pain is generally described as excruciating, like an electric shock. The attacks will be so severe that you are unable to do anything while they are happening.
What Are The Symptoms Of Occipital Neuralgia?
Symptoms of Occipital Neuralgia consists of :
pain on 1 side of the face
a reduced range of motion (ROM) in the neck
pain near the eyes
pain or stiffness of the neck
Pain radiate from the Upper trapezius muscle to the shoulder or sometimes arm region.
Spasm of Paraspinal Neck Muscles
pain while coughing and sneezing
pain in the neck, shoulder, and arm on the affected side
Throbbing head pain
Headache which is triggered by certain neck movements and postures
Weakness in the deeper neck flexors
sensitivity to light or noise
Nausea
Tenderness in the Upper Cervical area
Poor Posture
Blurred visionHow Is Occipital Neuralgia Treated?
Massage therapy.
Hot therapy, and using heating pads on the affected area.
Physical therapy.
Botulinum toxin (Botox) injections to reduced inflammation.
Nerve blocks, an injection of numbing medication or steroids.




One Comment