

Meniscus tear in Knee : Physiotherapy treatment
Table of Contents
What meniscus tear ?
Meniscus tear in the knee is a common injury, especially among athletes. Meniscus tear can be caused by twisting, bending, or direct blow to the knee. Symptoms of meniscus tear include swelling, pain when walking, and knee instability.
- Meniscus tear tear can be painful and debilitating. Unfortunately, it’s quite common. In fact, a meniscal tear is one of the most frequently occurring cartilage injuries of the knee.
- protects the bones from wear and tear. But all it takes is a good twist of the knee to tear the meniscus. In some cases, a piece of the shredded cartilage breaks loose and catches in the knee joint, causing it to lock up.
ANATOMY OF MENISCUS
- Knee menisci, two in number, are made of fibrocartilaginous tissue and present one each between lateral condylar articulation and medial condyles of tibia and femur. Knee meniscus or simply meniscus refers to either the lateral or medial fibrocartilaginous structure. The menisci are also known as semi-lunar cartilages because of their crescent shape.

Each meniscus has :
Two ends, both attached to the tibia
Two borders – Outer border is thick, convex and fixed to the fibrous capsule, inner border is thin, concave and free.
Two surfaces – The upper surface is concave for articulation with the femur. The lower surface is flat and rests on the peripheral two thirds of the tibial condyle. The peripheral thick part is vascular. The inner part is avascular and is nourished by synovial fluid.
The medial meniscus is nearly semicircular, being wider behind than in front. The posterior fibers of the anterior end are continuous with the transverse ligament. Its peripheral margin is adherent to the deep part of the tibial collateral ligament.
The lateral meniscus is nearly circular. The posterior end of the meniscus is attached to the femur through two meniscofemoral ligaments. The tendon of the popliteus and the capsule separate this meniscus from the fibular collateral ligament.
BIO-MECHANICAL OF MENISCUS
- The menisci act to disperse the weight of the body and reduce friction during movement. Since the condyles of the femur and tibia meet at one point (which changes during flexion and extension), the menisci spread the load of the body’s weight. This differs from sesamoid bones, which are made of osseous tissue and whose function primarily is to protect the nearby tendon and to increase its mechanical effect.

-The meniscus withstands many different forces such as shear, tension, and compression. It also plays a crucial role in load-bearing, load transmission, shock absorption, as well as lubrication and nutrition of articular cartilage . These multiple and complex functions require a specialized form. Since the tissue is wedge-shaped, it proves highly adept at stabilizing the curved femoral condyle during articulation with the flat tibial plateau.
During everyday activity, axial tibiofemoral forces compress the menisci. The wedge shape of the meniscus and its horn attachments serve to convert the vertical compressive forces to horizontal hoop stresses. At the same time, shear forces are developed between the collagen fibers within the meniscus while the meniscus is deformed radially.
SIGN & SYMPTOMS
You might feel a “pop” when you tear a meniscus. Most people can still walk on their injured knee. Many athletes keep playing with a tear. Over 2 to 3 days, your knee will gradually become more stiff and swollen.
- Knee Pain
- Knee joint Stiffness and swelling
- The sensation of your knee “giving way”
- You are not able to move your knee through its full range of motion
- Difficulty bending and straightening the leg
- A tendency for your knee to get “stuck” or lock up
CAUSES
- A torn meniscus can result from any activity that causes you to forcefully twist or rotate your knee, such as aggressive pivoting or sudden stops and turns. Even kneeling, deep squatting or lifting something heavy can sometimes lead to a torn meniscus. In older adults, degenerative changes of the knee can contribute to a torn meniscus with little or no trauma.
- If you are suffering from Knee osteoarthritis, you’re at higher risk of injuring your meniscus. Knee Osteoarthritis is a common joint disease in-which pain and stiffness in your joints also caused by aging and wear and tear.
Meniscus tear types
- Intrasubstance/Incomplete Tear :
An intrasubstance tear is a common finding on an MRI report. Seen in the upper left corner of the image, an intrasubstance tear typically looks normal at the time of surgery. Often these are a sign of early degenerative changes of the meniscus tissue, but seldom are they the sign of a problem. Incomplete and intrasubstance tears of the meniscus are stable injuries, and they generally do not require any surgical treatment. By the time people are in their 20s or 30s, intrasubstances changes of the meniscus tissue are very commonly seen on an MRI.

- Radial Tear :
Radial tears of the meniscus, pictured in the middle of the top row on the image, are the most common type of meniscus tear. These tears are within the avascular zone of the meniscus, where there is no blood supply, and therefore there is little capacity for these tears to heal. Therefore, when these tears come to requiring surgical treatment, typically the only option is to trim out the damaged portion of the meniscus.
- Horizontal Tear :
A horizontal tear is a tear that is most commonly amenable to meniscus repair. Seen in the upper right corner of the image, a horizontal tear runs along the circumferential fibers of the meniscus. Rather than removing the damaged portion of the meniscus, a horizontal tear may be able to be along the circumferential fibers of the meniscus. Rather than removing the damaged portion of the meniscus, a horizontal tear may be able to be sewn together. The key to determining the treatment of these tears is their location. If located within the vascular portion of the meniscus (near the outer edge) then there is healing potential, and thus repair. When located more centrally, these tears will not heal, even if repaired.
- Flap Tear :
A flap tear of the meniscus, pictured in the bottom left corner of the image, is an unusual pattern of the tear. In circumstances where the flap is causing symptoms of catching in the knee, usually, the flap of the meniscus can simply be removed without removing much tissue at all.
- Complex Tear :
A complex tear means there is a combination of tear patterns. Shown in the middle image on the bottom row, a complex tear often involves both radial and horizontal tear patterns. Typically complex tears are not treated with meniscus repair because of the complex nature of the tear. In some unusual circumstances, some of the torn meniscus can be removed, while other portions can be repaired.
- Bucket-Handle Tear :
A bucket-handle tear is a large type of horizontal tear of the meniscus. These tears often cause the knee to become stuck by causing the torn portion of the meniscus to block normal knee motion. Bucket-handle tears often require more urgent surgical treatment in order to allow the knee to start bending again.
DIAGNOSIS
- X-rays : Although x-rays do not show meniscus tears, they may show other causes of knee pain, such as osteoarthritis.
- Magnetic resonance imaging (MRI) : This study can create better images of the soft tissues of your knee joint, like a meniscus.
Test for meniscus tear
- EXAMINATION :-
- 1.McMurray test :
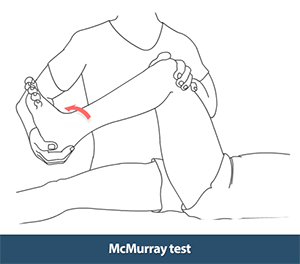
- The patient lies supine on the bed with the hip and knee both flexed. With the foot as close to the hip as possible, the clinician holds the knee joint (with fingers along the joint line) with one hand, and the other hand rotates the tibia internally and externally while extending and flexing the knee. If the test is positive (suggesting a meniscal tear), the patient will feel pain and the clinician will feel and/or hear meniscal movement when the meniscus is compressed between the tibia and femur

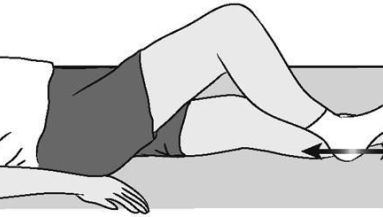
2.Apley test (grinding) test :
-The patient lies prone, with their knee flexed to 90 degrees and their hip extended. The clinician applies axial pressure to the foot and rotates the tibia internally and externally. Pain and/or clicking on compression suggest a meniscal lesion.
Meniscus tear Treatment :
Meniscus tear Treatment are mainly Medical treatment, Physiotherapy treatment, exercise, rest and last option is surgical treatment.
+MEDICAL TREATMENT :- Rest with modified activity.
Apply ice or a cold pack to your knee for 15- to 20-minute sessions, several times a day.
Compress your knee with a brace or knee sleeve to prevent additional swelling.
Elevate your leg above your heart while icing it or whenever resting/relaxing. Without treatment, a piece of meniscus may come loose and drift into the joint. This can cause your knee to slip, pop, or lock.
Meniscus tear surgery
1.Arthroscopic Meniscectomy

A meniscectomy is a procedure to remove the torn portion of the meniscus. This procedure is far more commonly performed than a meniscus repair. The meniscectomy is done to remove the damaged portion of the meniscus while leaving as much healthy meniscus as possible. The meniscectomy usually has a quick recovery and allows for the rapid resumption of activities.
2.Meniscus Repair

A meniscus repair is a surgical procedure done to repair the damaged meniscus. The meniscus repair can restore the normal anatomy of the knee and has a better long-term prognosis when successful. However, the meniscus repair is a more significant surgery, the recovery is longer, and because of limited blood supply to the meniscus, it is not always possible.
3.Meniscus Transplant
Meniscus transplantation consists of placing the meniscus from a deceased donor patient into an individual who has had their meniscus removed.
The ideal patient for a meniscus transplant is someone who had their meniscus removed and subsequently begins to develop knee pain.
Meniscus transplant is not performed for an acute meniscus tear, but rather when removal of the entire meniscus has caused persistent pain in the knee.
PHYSIOTHERAPY TREATMENT :-
Physiotherapy treatment is pain relieving Electrotherapy modalities such as IFT (Interferential Therapy), TENS, Ultrasound Therapy and Exercise.

SQE (Static Quadricep Exercise) :-
Sit on the floor with your injured leg straight out in front of you.
Tighten the muscles on top of your thigh by pressing the back of your knee flat down to the floor.
Hold for about 6 seconds, then rest up to 10 seconds.
HEEL SLIDE :-
Sit on a firm surface with your legs straight in front of you. Slowly slide the heel of the foot on your injured side toward your buttock by pulling your knee toward your chest as you slide the heel. Return to the starting position. Do 2 sets of 15.
-SLR (Straight Leg Raise) :-

Lie on your back with your good knee bent so that your foot rests flat on the floor. Your injured leg should be straight. (During this exercise, your low back should have a normal curve. Your back has a normal curve if you can slip your flat hand in between the floor and the small of your back, with your palm touching the floor and your back touching the back of your hand.)
Tighten the thigh muscles in the injured leg by pressing the back of your knee flat down to the floor. Hold your knee straight.
Keeping the thigh muscles tight, lift your injured leg up so that your heel is about 12 in. (30 cm) off the floor. Hold for 5 seconds, then lower slowly.
PRONE HIP EXTENSOR :-

Lie on your stomach, and lift your leg straight behind you (toward the ceiling).
Lift your toes about 6 in. (15 cm) off the floor, hold for 5 seconds, then lower slowly.
PRONE HAMSTRING :-

Lie on your stomach with your knees straight. If your kneecap is uncomfortable, roll up a washcloth and put it under your leg just above your kneecap. Lift the foot of your injured leg by bending the knee so that you bring the foot up toward your buttocks. If this motion hurts, try it without bending your knee quite as far, in order to avoid any painful motion.
You may also want to add a cuff weight to your ankle [not more than 5 lb (2 kg)], or use soup cans in a plastic bag with the loops around your ankle. With weight, you don’t have to lift your leg more than 12 in. (30 cm) to get a hamstring workout.

HEEL RAISE :-
Stand with your feet a few inches apart, with your hands lightly resting on a counter or chair in front of you.
Slowly raise your heels off the floor while keeping your knees straight. Hold for about 6 seconds, then slowly lower your heels to the floor.
STANDING CALF STRETCH :

Stand facing a wall with your hands on the wall at about eye level. Keep your injured leg back with your heel on the floor. Keep the other leg forward with the knee bent. Turn your back foot slightly inward (as if you were pigeon-toed). Slowly lean into the wall until you feel a stretch in the back of your calf. Hold the stretch for 15 to 30 seconds. Return to the starting position. Repeat 3 times. Do this exercise several times each day.
HAMSTRING STRETCH ON WALL :

Lie on your back with your buttocks close to a doorway. Stretch your uninjured leg straight out in front of you on the floor through the doorway. Raise your injured leg and rest it against the wall next to the door frame. Keep your leg as straight as possible. You should feel a stretch in the back of your thigh. Hold this position for 15 to 30 seconds. Repeat 3 times.
STEP UP :- Stand with the foot of your injured leg on a support 3 to 5 inches (8 to 13 centimeters) high –like a small step or block of wood. Keep your other foot flat on the floor. Shift your weight onto the injured leg on the support. Straighten your injured leg as the other leg comes off the floor. Return to the starting position by bending your injured leg and slowly lowering your uninjured leg back to the floor. Do 2 sets of 15.
Meniscus tear brace :
A meniscus tear brace is designed to provide support and stability to the knee during activities that may cause pain or discomfort. A meniscus tear brace is made up of three parts: an outer shell, a center pad, and an inner strap. The shell provides stability and limits movement. The center pad provides cushioning and protection for the knee. The inner strap gives additional support to the knee joint by attaching the outer shell to the thigh. Meniscus tear braces are used to treat injuries such as a torn anterior cruciate ligament (ACL).
A meniscus tear brace is an orthotic device that is used to help support the knee during physical activity. Meniscus tears are common injuries, particularly in sports such as basketball and soccer, where athletes are required to make sudden movements while bearing weight on their knees. Meniscus tear braces provide support for the knee and prevent the knee from hyperextending. They are clinically proven to reduce pain and swelling during physical activity, and can help prevent further injury to the knee.



MEDIAL MENISCUS TEAR GRADE -3 POSTERIOR HORN, SURGERY PACKAGE COST ??
THANKS
ASGAR BHATI
8005653095
CHURU RAJASTHAN
AGE -38