
Manual Muscle Testing (MMT): Grading, Procedure
Table of Contents
What is a Manual Muscle Testing (MMT)?
Manual Muscle Testing(MMT) is an assessment method for the evaluation of muscle weakness used by physiotherapists, chiropractors, and other healthcare professionals to make an effective treatment plan and is also helpful in the progress of muscle strength throughout a specific regimen.
Manual Muscle Testing (MMT) is a vital part of medical examination.
MMT is a procedure for the evaluation of the strength of an individual muscle or muscle group, based on the effective performance of a movement in relation to the force of gravity or manual resistance through the available range of motion
i.e. How efficiently a muscle is working.
Muscle strength tests can be performed using manual strength testing, dynamometry, and functional tests. Manual muscle testing is one of the most commonly used for muscle testing by physiotherapists.
With Manual Muscle testing(MMT), the patient is informed to move the limb to be tested in its available range of motion, working against gravity or while the examiner gives opposing manual resistance to check the grade of the muscle.
Manual Muscle testing(MMT) is an essential part of a physiotherapy assessment and grading of muscle strength that help when performed properly. MMT can provide important information which can help therapists in planning appropriate interventions, modifications, or treatments. There are certain protocols to use when performing MMT to ensure quality results.
Basic Components of Motor Examination:
1. Nutrition or bulk of muscle
2. Tone
3. Reflexes
4 Range of motion (ROM)
5. Manual muscle testing
6. Functional assessment
As per Daniels and Worthington’s book ‘Muscle Testing: Techniques of Manual Examination and Performance Testing’, there are two different methods for performing manual muscle testing.
1. Break testing:
in manual muscle testing, is when resistance is applied to the body part at the end of the available range of motion. It’s called the break test because when a therapist provides resistance the objective for the patient is to not allow the therapist to “break” the muscle hold.
2. Active Resistance testing:
in manual muscle testing is when resistance is applied through the body part through the available range of motion. This type of manual muscle testing requires skill and experience and is not the recommended practice.
Protocols for Manual Muscle Test (MMT):
Here are some basic Protocols you can consider for more accurate MMT results:
- Make sure to discuss with the patient before starting MMT and the results you are looking for.
- Start with the non-injured side first and applied consistent force when applying pressure.
- Instruct your patient to breathe normally during the test.
- Make sure the patient is dressed comfortably in loose clothing and has a full range of movement.
- Place the patient in a fully supported position, so they are able to completely focus their effort on the body part being tested.
- Always start with testing an antigravity position. If muscles are weak then, they are then tested in the horizontal plane.
- Resistance is applied opposite the direction of the muscles being tested.
- Make proper planning before starting MMT such as all the muscles that should be examined in one position. This reduces any inefficiency during the examination and reduces examination time.
- Always try to provide adequate stabilization to unrelated joints to avoid tricky movements such as stabilization of the shoulder will prevent motion when the patient is resisting elbow flexion.
- Always perform both sides to compare the muscle grades to get the most exact examination of strength.
These protocols are important to get the most accurate results with MMT. However, there are a few things to avoid which can negatively affect results.
What to Avoid When Performing Manual Muscle Testing?
Few things you should avoid when performing MMT:
- Avoid jerking motions when applying resistance during testing
- Discontinue testing if the patient has pain or discomfort
- Do not leave the patient unattended
Grades of Manual Muscle Testing (MMT):
1. MRC scale
2. oxford scale
3. Kendall scale
4. others
1. MRC SCALE:
| MRC Scale | Explanation |
| 0 | No visible or Palpable contraction |
| 1 | Visible or Palpable Contraction |
| 2 | Full ROM gravity eliminated |
| 3 | Full ROM against gravity |
| 4 | Full ROM against Gravity, Moderate Resistance |
| 5 | Full ROM against Gravity, Maximum Resistance |
2. OXFORD GRADING:
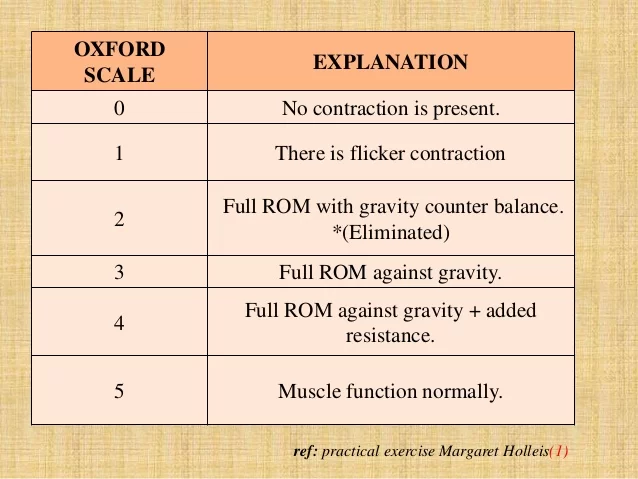
MODIFIED OXFORD GRADING:
(0): No contraction
(1): flicker contraction
(2-): moves through partial ROM gravity eliminated
(2): able to move through full ROM gravity eliminated
(2+): moves through full ROM gravity eliminated with resistance
(3-): partial ROM against gravity
(3): full ROM against gravity
(3+): person hold the position against gravity with slight resistance
(4): full ROM against gravity with moderate resistance
(5): full ROM against gravity with maximum resistance
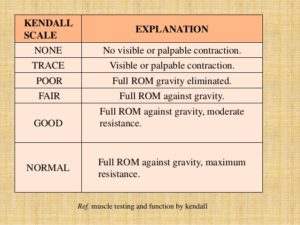
3. KENDALL SCALE:
Basic Rules of Manual Muscle Testing:
-patient position
-joint position
-check the available passive ROM
-give accurate, audible commands and instructions
-demonstrate the desired movement
-check the strength of the normal side first
-do not change the patient’s position repeatedly
-always start with grade 3 i.e. against gravity movement
Hand Placement:
PROXIMAL HAND:
At the origin of the muscle and proximal joint giving stabilization.
DISTAL HAND:
distally offering resistance or assistance depending upon performance.
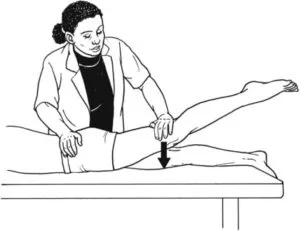
Application of Resistance:
-resistance is applied slowly and gradually.
-increasing or decreasing manual resistance.
-increasing or decreasing the length of the weight arm.
example:-with the patient is in a prone position a known resistance is given at the level of the knee joint is more easily overcome by hip extensors than if it is applied at the foot.
Contraindications of Manual Muscle Testing (MMT):
-If the motion to the joint will cause further damage or interrupt the healing process immediately after injury or surgery.
-Therapist suspects subluxation (partial dislocation), dislocation, or fracture.
-If myositis ossificans (pieces of bone in the muscle) or ectopic ossification (pieces of bone forming in the tissue) is suspected or present, AROM and PROM should not be undertaken without first ensuring the patient is assessed by a professional who has expertise.
-If inflammation is present in the region.
-Presence of inflammatory neuromuscular disease (Guillain-Barre, polymyositis, dermatomyositis).
-For patients with severe cardiac or respiratory disease or disorders associated with acute symptoms.
-In the presence of pain. Pain will inhibit muscle contraction and will not give an accurate indication of muscle strength. May also cause further injury.
Precautions:
-In painful conditions.
-In the presence of an inflammatory process in a joint or the region around a joint.
-In patients taking medication for pain or muscle relaxants, because a patient may not be able to respond appropriately and movement may be performed too vigorously.
-In the presence of marked osteoporosis or in conditions where bone fragility is a factor, perform PROM with extreme care or not at all.
-In assessing a hypermobile joint.
-In patients with hemophilia.
-In the region of a hematoma, especially at the elbow, hip, or knee.
-In assessing joints if bony ankylosis (bones fused together) is suspected.
-After an injury where there has been a disruption of soft tissue (tendon, muscle, ligament).
-In the region of a recently healed fracture.
-After prolonged immobilization of a part.
Manual Muscle Testing of Upper Extremities:
-Shoulder Flexion
-Shoulder Extension
-Shoulder Abduction
-Shoulder Horizontal Adduction
-Scapula Elevation
-Scapular Retraction/ Adduction
-Elbow Flexion
-Elbow Extension
-Wrist Flexion
-Wrist Extension
Manual Muscle Testing of Lower Extremities:
-Hip flexion
-Hip extension
-Hip abduction
-Hip adduction
-Hip internal rotation
-Hip external rotation
-Knee flexion
-Knee extension
-Ankle dorsiflexion
-Ankle planter-flexion
-Ankle inversion
-Ankle eversion
What is the limitation of MMT?
Manual Muscle Testing (MMT) has several limitations that should be considered when using this assessment technique:
- Subjectivity: MMT heavily relies on the therapist’s subjective judgment and interpretation. The grading of muscle strength is based on the therapist’s perception of resistance or movement, which can introduce variability and subjectivity in the results.
- Lack of standardization: There is no universally accepted standardization for MMT. Different therapists may use slightly different techniques or grading scales, which can lead to inconsistencies in the assessment and make it difficult to compare results between practitioners.
- Cooperative effort required: MMT requires active patient participation and cooperation. Some patients, such as those with neurological or cognitive impairments, may have difficulty understanding or following the instructions, compromising the reliability of the assessment.
- Limited assessment of functional movements: MMT assesses muscle strength in isolated movements or muscle contractions. It may not fully capture the muscle’s ability to perform complex functional movements or activities that involve multiple muscle groups working together.
- Influence of pain and fatigue: Pain or discomfort experienced by the patient during MMT can affect their ability to generate maximal muscle contraction. Similarly, fatigue can impact subsequent repetitions of the test, leading to inaccurate strength assessment.
- Inability to assess muscle coordination and timing: MMT primarily focuses on muscle strength and does not evaluate factors such as muscle coordination, timing, or neuromuscular control, which are essential for optimal movement and function.
- Lack of sensitivity: MMT may not be sensitive enough to detect small changes in muscle strength, especially in patients with mild weakness or those who are already at a high level of strength.
Despite these limitations, MMT can still provide valuable information when used in conjunction with other assessment techniques and clinical judgment. It is important for physiotherapists to be aware of these limitations and consider them when interpreting the results and designing appropriate treatment plans for their patients.
Clinical Significance
Manual Muscle testing(MMT) can help assessment of many conditions in which examination of muscle weakness plays a key role. Careful examination and proper technique are essential for ensuring valid and quality assessments.
The Oxford Scale is commonly accepted worldwide and does not require any equipment, and also shows reasonable interrater reliability. Hand-grip dynamometry is less subjective and gives a significant measurement that can be used over time for precise methods of measurement.
Manual Muscle testing aims at how individual patients are able to perform their daily living and whether muscle strength is a limiting factor.
Protein supplementation may push gains in both aerobic and anaerobic power as the frequency, duration, and volume of strength training improve.
FAQ
How accurate is MMT?
Manual Muscle Testing (MMT) is a widely used method for assessing muscle strength in clinical settings. However, its accuracy and reliability can vary due to several factors. Here are some considerations regarding the accuracy of MMT:
Inter-rater reliability: MMT’s accuracy can be influenced by the reliability between different therapists or assessors. Different practitioners may have varying levels of experience, training, and subjective judgment, leading to inconsistencies in grading and results. Standardization and training can help improve inter-rater reliability.
Intra-rater reliability: Even when performed by the same therapist, MMT may exhibit variability in results. Factors such as inconsistent application of resistance, variations in patient positioning, and differences in subjective interpretation can affect the reliability of repeated measurements by the same practitioner.
Subject cooperation and effort: The accuracy of MMT depends on the patient’s cooperation and ability to give maximal effort during the test. Factors such as pain, discomfort, fatigue, and patient comprehension can impact the reliability of results. Patients with neurological or cognitive impairments may have difficulty following instructions or providing consistent effort.
Limitations in assessing specific muscle functions: MMT primarily evaluates muscle strength in isolated movements or contractions. It may not fully capture the muscle’s ability to perform complex movements or functional activities that involve multiple muscle groups working together. This limitation can affect the accuracy of MMT when assessing certain functional movements.
Validity and sensitivity: The validity of MMT refers to its ability to accurately measure the construct it intends to assess, which is muscle strength in this case. While MMT has been widely used in clinical practice, its validity has been a topic of debate. Some studies suggest that MMT may lack sensitivity in detecting subtle changes in muscle strength, especially in individuals with mild weakness or high levels of strength.
Complementary assessments: To enhance the accuracy of muscle strength assessment, MMT is often used alongside other assessment methods such as dynamometry (measuring force using devices) and functional performance testing. Combining multiple assessment tools can provide a more comprehensive evaluation of muscle strength and minimize the limitations of individual methods.
It’s important to note that the accuracy and reliability of MMT can be influenced by various factors, and its results should be interpreted in conjunction with other clinical findings, patient history, and the therapist’s professional judgment.Who started Muscle testing?
Manual muscle testing (MMT) was developed by several researchers and practitioners in the field of physical therapy, including Kendall, McCreary, and Provance. However, MMT can be traced back to the work of Swedish physician, Gustav Zander, who developed an early version of the dynamometer in the 19th century. The dynamometer was a device that measured muscle strength by applying resistance to various muscle groups.
Later, in the early 1900s, physical therapist Florence Kendall incorporated muscle testing into her clinical practice, which eventually led to the development of the Kendall method of MMT. This method used standardized techniques and grading scales for assessing muscle strength in different muscle groups. Kendall’s work significantly influenced the field of physical therapy and laid the foundation for modern MMT techniques.
Since then, various researchers and practitioners have contributed to the development of MMT and its applications in clinical settings. Today, MMT is a commonly used method for assessing muscle strength and function in physical therapy, sports medicine, and other healthcare fields.




i’d like to know the referrence of the first figure