

Lumbar spine range of motion exercise
A Lumbar spine range of motion exercise mainly refers to an activity aimed to increase the movement of the lower back. The movement is mainly influenced by many structures, as well as configurations of the bone surfaces within the lumbar spine, joint capsule, ligaments, tendons, & muscles acting on the lumbar joint.
A range of motion exercise is also called the “ROM” exercise. This is the capability of the lumbar spine to go through its complete spectrum of motion. The range of motion of a lumbar spine may be a passive range of motion exercise, and active-assisted range of motion exercise, or an active range of motion exercise.
Table of Contents
Introduction of the three types of a range of motion exercise
- The first one is the passive range of motion: A motion is applied to the lumbar spine only by other individual or individuals. When the passive range of motion is applied, the lumbar spine of the person receiving exercise is completely relaxed while an outside force moves the body part, namely the lumbar, throughout the available range of motion.
- The second one is the active-assisted range of motion: A lumbar spine receives minimal help from an outside force. The range of motion may result from the majority of the motion applied by a physical therapist or by a person or individuals helping the patient. It can be the half effort on the lumbar spine from each source, meaning a patient’s own effort and the external force.
- The last one is the active range of motion: A motion of the cervical spine provided entirely by the patient performing this exercise. In this mode of exercise, there is no outside force adding to a motion during performing the movement.
What is a goniometer?
- The goniometer is a metal or even plastic device with two arms that are used to measure the range of motion of the lumbar spine. The goniometer is placed on the head as well as measured by looking at the numbers to represent angular distance on the device. To measure the lumbar spine range of motion the physical therapist most commonly use a goniometer.
- If the patient is suffering from a decreased range of motion in the lumbar spine, the physical therapist can use the goniometer to assess what the range of motion is at the beginning of an assessment, and then the therapist makes sure the intervention is working by using a goniometer in subsequent sessions as well.
Various types of the Goniometers
- There are several types of goniometers available, but of all the types, the universal goniometer is the most widely used.
- Universal Goniometer
A universal goniometer comes in two forms, the first one is a short arm, and the second one is a long arm. The short arm goniometer is used for smaller joints such as the wrist, elbow, or ankle, whereas long arm goniometers are more accurate for the joints with long levers such as the knee as well as hip joints. - Gravity Goniometer/Inclinometer
In the type of goniometer, one arm has the weighted pointer which remains vertical under the influence of gravity. - Software/Smartphone-based Goniometer
The smartphone as a digital goniometer has several benefits such as availability, ease of measurement, application-based tracking of the measurements, and one-hand use. These types of goniometers use the accelerometers in phones to calculate knee joint angles. - Arthrodial Goniometer
This is ideal for measuring cervical rotation, anteroposterior flexion, and lateral flexion of the cervical spine as well. - Twin axis electrogoniometer
The inter-rater, and intra-rater reliability of an electrogoniometer, is higher than the universal goniometer still challenging to apply in the clinical evaluation of a patient, hence used more often for research purposes.
Tape Measure
- The least expensive instrument for measuring spinal motion, and perhaps the easiest to use, is the tape measure. Moreover, the tape measure probably has been used in the clinic for measuring the range of motion of the lumbar spine longer than any other measurement.
Movements of the lumbar spine
- Flexion: When the spine is bent forward meaning towards the floor side from anteriorly.
- Extension: When the spine is bent backward meaning towards the floor side from posteriorly.
- Lateral flexion: When the spine moves laterally on the left and right sides.
- Rotation: When the spine rotates to right and left sides.
Measurement of the flexion as well as extension
Schober Method
- One of the most common tape measure procedures used to measure lumbar flexion relates to the technique originated by Schober and subsequently modified for the measurement of spinal flexion. Macrae, as well as Wright Schober, described an original two-mark method for the measuring lumbar spine flexion, in which one mark is made at a lumbosacral junction, as well as the second mark is made 10 cm above the first mark, whereas the subject stands with a spine in a normal position. Then the standing subject bends forward as long as possible, and an increase in distance between the first as well as second marks provides the estimate of the amount of flexion that is present in the lumbar spine.
- Due to a tape measure technique relying on the stretching or even distraction of the skin overlying the spine, this technique is sometimes referred to as a skin distraction method.
- Macrae and Wright modified an original Schober method by introducing the third mark, the measurement mark placed 5 cm below the lumbosacral junction. It is modification uses the mark at a lumbosacral junction as well as other marks 5 cm inferior as well as 10 cm superior to a lumbosacral junction. The rationale offered by Macrae as well as Wright for making a modification of the original Schober technique is that when using a Schober technique in their pilot work, and authors observed that skin above as well as below the lumbosacral spine was distracted while flexion of a lumbar spine, leading to inaccuracies in measurement. This is a technique that Macrae, as well as Wright8, referred to as the “modified” Schober technique included three marks:
- The first one is the lumbosacral junction,
- The second one is 5 cm inferior to the lumbosacral junction, and
- The last one is 10 cm superior to the lumbosacral junction. Van Adrichem as well as van der Korst13 suggested that using a lumbosacral junction (the base mark used for a Schober technique), which had to be identified by palpation, added difficulty to the method of measurement. Given this information, Williams et al14 suggested that a “modified-modified Schober,” rather than a Schober or even the modified Schober method, should be used.
- The modified-modified Schober uses two skin landmarks (as opposed to the three skin landmarks used with a modified Schober). These two landmarks include the point bisecting a line that connects the two posterior superior iliac spines (PSIS) (baseline) as well as the mark 15 cm superior to a baseline landmark.

Measurement for the lateral Flexion
- Two methods for using the tape measure to examine lateral flexion of the lumbar spine have been introduced in the literature, with neither method becoming predominant in clinical use. These described two methods include placing marks at a lateral thigh as well as the fingertip-to-floor method.
- Measuring lateral flexion by placing the mark at a location on a lateral thigh that the third fingertip may touch while erect standing as well as after lateral flexion was first introduced by Mellin. The distance between described two marks represents a range of lateral flexion to that side.
- Using a fingertip to floor method, the distance from the third fingertip to a floor is measured, first with a patient standing erect, as well as then the subject laterally flexes the spine. The change in distance from the erect standing to lateral flexion is considered a range of lateral flexion.
Passive range of motion exercise
- A passive range of motion exercise is really useful for the lumbar spine that has become inactive because of an injury or even a paralysis attack. In a passive range of motion exercises, the patient does not perform any type of movement themselves; instead, a physical therapist or even caretaker moves a stiff lumbar joint, smoothly stretching muscles and reminding them how to move correctly as well.
- In most cases, therapeutic stretching exercises are combined with the passive range of motion exercises to promote faster recovery of the stiff or flaccid lumbar spine. Here, the clinician stretches the soft tissue of the lumbar spine to relax the surrounding muscles as well as relieve tension. The passive range of motion exercises also assists in minimizing stiffness, rigidity, or even flaccidity in the lumbar spine that has been immobilized.
- The safest, as well as common passive range of motion(PROM)exercises, are related to stretching the surrounding muscles with the aim to increase muscle flexibility. The most common way to do this exercise is with the use of a tool, namely a stretching strap. This will assist the patient to hold the stretch for a more sustained period of time, but having a physiotherapist who helps with the stretch is a more beneficial way to practice passive range of motion(PROM) exercises. With this type of exercise, the trained professional moves a body into a stretch as well as holds it, with an intent to improve muscle flexibility.
- This is superior for some reasons.
- The first one is a physiotherapist understands proper limits and knows how far to go.
- The second one is a physiotherapist knows how long to hold a stretch.
- The last one is that physical therapists are also trained to know if it is targeting the proper areas to achieve more benefits. With that in the brain.
In which conditions a physical therapist should apply the passive range of motion exercise
- Passive range of motion exercises is used when there is a paralysis attack, when a patient is comatose, in the presence of the healing fracture, or if the pain is elicited while the active muscle contraction. One of the main goals of a passive range of motion exercise is to counteract the detrimental effects of immobilization. However, this is mandatory to remember that a passive range of motion exercise cannot prevent muscle atrophy.
Some benefits of the passive range of motion exercise
- The passive range of motion exercise not only gives assistance in promoting healthy joint functionality but also benefits a patient in decreasing pain, increasing healing, restoring as well as maintaining range of motion in the lumbar spine, and building muscle mass, allowing for the great blood flow as well as helping in improving oxygen levels.
Some guidelines for the passive range of motion exercise for the lumbar spine
- Passive range of motion can be done in the supine or in a sitting position.
- Support the weight of the leg at all times during performing the lumbar spine movement.
- Support above and below the lumbar spine the patient is moving.
- Keep the movement slow and smooth as well.
- Do not force the movement if the lumbar muscle or lumbar joint is stiff.
- The therapist should move only as much as the lumbar muscle or lumbar joint will allow.
- A passive range of motion should be pain-free, if lumbar motions cause pain, stop as well as let the physical therapist know.
- Performing the passive movements in the lumbar spine can be difficult, as the physical therapist needs to move a heavy trunk and/or lower limbs. Thus, joint play movements often replace passive movement. When performing these movements, reduced range of motion, pain, or even changes in end feel should be noted.
Exercises
- Lumbar passive flexion
First of all, the therapist should tell the patient that he should take the side-lying position, with knees as well as hips at 90 degrees. After that, the physical therapist palpates between spinous processes using three fingers; one above a spinous process, one on as well as one below the process. Next, the physical therapist then uses their body weight to perform the flexion motion in a lumbar spine, as well as feels for the ‘gapping’ while performing the movement, noting if a motion is normal, hypo, or hypermobile. Results depend on the ability of the physical therapist, as a test shows only average inter-rater reliability. Do this action ten times per session. Do three sessions per day.

- Lumbar passive extension
To begin with, the physical therapist should tell the patient to take a prone position, with the arms crossed as well as the head resting on the hands. After that, the physical therapist uses the crossed arms to pull a patient’s trunk upwards, while feeling the motions of the spinous processes as well as noting normal, hypo or hypermobility. Perform this movement ten times per session gently. Do three sessions per day. - Left side lumbar passive side flexion
To embark with, the physical therapist tells the patient that lies prone, in the same position as the extension. Next, the physical therapist again uses the crossed arms to pull a patient’s trunk left side as well as notes a ‘gapping’ between the spinous processes as well as whether the motion is normal, hypo, or hypermobile. Perform this action ten times per session. Do three sessions per day. - Right side lumbar passive side flexion
To start with, a physiotherapist should tell a patient to take a prone position, in the same position as an extension. After that, a clinician again uses the crossed arms to pull the patient’s trunk sidewards and notes the ‘gapping’ between the spinous processes and whether the movement is normal, hypo, or hypermobile. Do it ten times in one session. Do three sessions in one day. - Left side lumbar passive rotation
First of all, the physiotherapist tells the patient to take a side-lying position, with hips as well as knees flexed and arms crossed as well. A physical therapist uses one hand to palpate the spinous process and another arm on a hip to create the left side rotational movement, noting a motion as normal, hypo, or hypermobile. Perform ten repetitions in one session. Do three sessions per day. - Right side lumbar passive rotation
To start with, a physical therapist should tell a patient to take the side-lying position, with hips and knees flexed as well as arms crossed. The physiotherapist uses one hand to palpate the spinous process as well as the other arm on the hip to create the right side rotational movement, noting the motion as normal, hypo, or hypermobile. Do it ten repetitions per session. Do three sessions in one day.
Active-assisted range of motion exercise
- As the name suggests, these exercises mainly involve minimal help from a physical therapist or even from a patient himself/herself or even with the use of a tool, such as a band or a strap. The patient does most of the movements, but the patient gets little help to complete the lumbar motion correctly. Frequently, in the major cases, these restricted lumbar movements are the result of the weakness or pain caused due to falls, bruises, or accidents, up to major injuries. The physiotherapist mostly uses a strap or even a band to secure the lumbar spine before assisting in the movement. In the starting, a patient may suffer a great deal of pain as well as a weakness when performing these lumbar spine exercises, but with time, a patient has a great scope for gradual as well as lasting improvement in a range of motion around the lumbar joint.
Some benefits of the lumbar active-assisted range of motion exercise
- Improve movement of the lumbar spine.
- Increase the function of the lumbar spine.
- Improve lumbar spine movement efficiency.
- Improve independence.
- Helps to Reduce Back pain
- Improve as well as maintain knee-joint integrity.
How does the patient get started?
- Learn the active-assisted range of motion exercises for the lumbar spine from a patient’s home health care. The patient can practice these exercises with the assistance of the patient’s home-health therapist. A physical therapist can instruct a patient on correct handholds and assist the needs of the patient. The therapist may also show the easiest way to do all these exercises therefore a patient does not get hurt or even tired. Find a comfortable position for a patient. Most patients prefer to use a bed for exercising with support.
- Do all lumbar range of motion exercises slowly, smoothly, and gently as well. Never force jerk or over-stretch the muscles of the lumbar spine. This can hurt the muscle or the joint instead of assisting. Move the lumbar joint only to a point of resistance. This is the point where the patient may not bend the joint any further. Stop lumbar range of motion exercises if a patient feels pain while performing the motion. Ask the physical therapist to tell a patient right away if he/she feels increased pain as well as soreness that does not stop after ceasing any exercise. Lumbar range of motion exercises may cause mild symptoms, but again, should subside quickly. Try to do these exercises again by modifying a physical therapist’s assistance level; which can decrease the soreness noted with the exercise.
Exercises
- Lumbar active-assisted flexion
To begin with, a physical therapist should tell a patient that he/she should take a side-lying position, with knees and hips at 90 degrees. Next, a therapist palpates between the spinous processes using three fingers; one above the spinous process, one on, and one below the process. After that, the physical therapist gives the command to the patient to move the body upward on the face side and perform the flexion motion in the lumbar spine, if the patient is not able to do the entire movement then the therapist will assist the patient to complete the full range of the lumbar flexion. Do it ten times in one session. Do three sessions in one day. - Lumbar active-assisted extension
First of all, a physiotherapist should tell a patient to take the prone position, with the arms crossed and head resting on
the hands. Next, a physiotherapist gives the command to the patient to move the trunk upside towards the ceiling as far as possible, but when the patient cannot perform the entire range of motion then the therapist assists the patient to complete the full range of motion. Perform ten times in one session gently. Do three sessions in one day.

- Left side lumbar active-assisted side flexion
To start with, a therapist tells a patient that lies prone, in the same position as an extension. After that, a physical therapist gives the command to a patient that touches the lower limb as far as possible on the left side, but when the patient cannot complete the full range the therapist assists the patient to reach the full range of side flexion on the left side. Do this action ten times in one session. Do three sessions in one day. - Right side lumbar active-assisted side flexion
To embark with, the physical therapist should tell the patient to take a prone position, in the same position as the extension. Then, the physiotherapist gives the command to the patient that touches the lower limb as far as possible on the right side, but when the patient can not reach the end point then the therapist helps in completing the entire range of side flexion. Perform this ten times per session. Do three sessions per day. - Left side lumbar active-assisted rotation
To begin with, a physical therapist tells a patient to take the sitting position, with hips and knees flexed as well as arms crossed. The therapist uses one hand to palpate a spinous process as well as the other arm on the hip to create the left side rotational movement, After that, the therapist gives the command to the patient that moves the upper body on the left side, meaning turn on the left side, but when the patient cannot complete the full range of lumbar rotation, then the therapist assists the patient to complete the full range of motion. Perform ten repetitions per session. Do three sessions per day. - Right side lumbar active-assisted rotation
First of all, the physical therapist tells the patient to take the sitting position, with hips as well as knees flexed as well as arms crossed. A physical therapist uses one hand to palpate the spinous process as well as another arm on the hip to create the right side rotational movement, Next, a physical therapist gives a command to a patient that moves the upper body on the right side, meaning turn on the right side, but when a patient cannot complete the entire range of lumbar rotation, then a physiotherapist helps a patient to complete the full range of lumbar rotation on the right side. Do ten repetitions in one session. Do three sessions in one day.
Active range of motion exercise
What is the active range of motion exercises?
- This type of exercise helps in increasing joint function. A range of motion is how far a patient can move the joints in different directions. These exercises help a patient in moving the lumbar through its full range of motion. The motion may assist to keep the lumbar joints flexible, reduce pain, and improve balance as well as strength.
What does a patient need to know regarding the active range of motion exercises?
- Do these exercises a physiotherapist teaches the patient about active range of motion exercise. Practice these exercises with the healthcare provider before the patient tries them by himself. Lumbar range of motion exercises are done daily, or as often as directed by a healthcare provider. Do lumbar joint exercises in the same order day. Go from flexion to extension to side flexion on both sides to rotation on both sides to assist the patient to remember the series of moves. Move slowly, gently, and smoothly. Avoid fast or jerky motions. Stop if a patient feels pain. It is absolutely normal to feel some discomfort while the movement at first. Regular exercise can help to reduce discomfort over time.
Some benefits as well as instruction of active range of motion exercise
- The patient has been provided with these exercises to assist in improving the neck stiffness as well as pain condiction.
- These exercises are intended as a guide and prior to starting a patient should have had some instruction from a clinician or even medical professional. If a patient experiences worsening symptoms during completing these exercises a patient may want to seek guidance from a physical therapist. Progress at a patient’s own pace, as a pain or even stiffness, allows, under the supervision or even guidance of the physiotherapist or medical professional.
Exercises
- Knee to chest
First of all, the therapist should tell the patient to lie on the back with the knees bent
as well as the feet on the ground. After that, lift one knee towards the chest, place the hands behind a knee and draw it into the chest. Repeat this action ten times per session. Do three sessions per day.

- Active lumbar left side rotation
To begin with, tell the patient to lie on the back with knees together as well as bent. After that, slowly roll the knees to the left side. Then, keeping the upper trunk still. Repeat ten times per session. Do three sessions per day. - Active lumbar right-side rotation
To embark with, the therapist tells a patient to lie on the back with knees together and bent as well. Next, slowly roll the knees to the right side. After that, keep the upper trunk straight. Repeat ten times in one session. Do three sessions in one day. - Active lateral flexion on the left side
First of all, tell the patient to stand straight. Next, the therapist instructs the patient to bend on the lift side meaning, touch the left side of the knee as far as possible. Repeat ten times per session. Do three sessions per day. - Active lateral flexion on the right side
To begin with, the therapist tells a patient to stand straight. After that, a clinician gives the instruction to the patient to bend on the right side meaning, touch the right side of the knee as far as possible. Repeat ten times in one session. Do three sessions in one day. - Active flexion in sitting
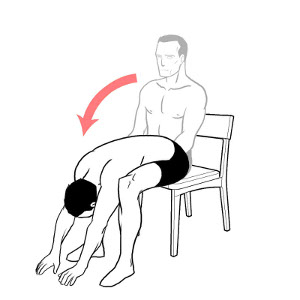
First of all, the patient should sit on the chair with the legs apart. After that, bend the head as well as trunk down between
the knees rounding the upper body as far as possible. Repeat ten times per session. Do three sessions per day.
- Extension in supine
To begin with, the patient should lie face down, leaning on the elbows/forearms. Moreover, arch the small of the back by pressing the pelvis as well as the stomach to the ground. Now bend the upper back upwards keeping forearms on the ground. Repeat ten times per session. Do three sessions per day.



One Comment