

Hip Dysplasia
Hip dysplasia is a problem that is sometimes noticed in babies, and sometimes in children, around the time they’re learning to walk. … Usually, the ball at the top of your baby’s thighbone (the femoral head) is held in a cup-shaped socket in the pelvis. The ball is held in the socket by ligaments and muscles.
It is sometimes called ‘clicky hips’, because if you move the hips of a baby with hip dysplasia, you can feel a little click.
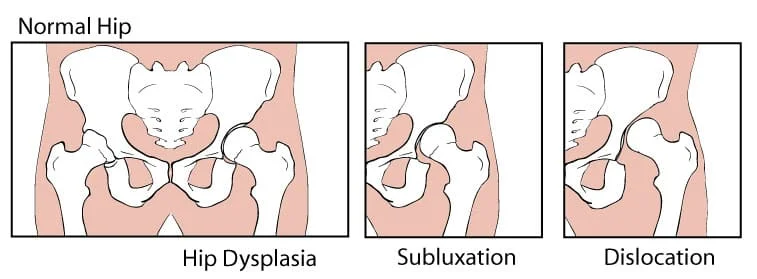
A hip problem in infants is known as developmental dysplasia of the hip (DDH). It is when the ball of the hip joint does not fit well in the socket. Often, this means that the hip joint is loose and prone to injury. DDH can lead to dislocation of the hip or other health issues.
Usually, the ball at the top of your baby’s thighbone (the femoral head) is held in a cup-shaped socket in the pelvis. The ball is held in the socket by ligaments and muscles.
If your child has hip dysplasia, then the femoral head can move away from that normal position and your baby’s hip will not develop correctly.
Nobody really knows what causes hip dysplasia. It is more common in babies who were in a breech position before birth, meaning they were head up instead of head down. It is more common in girls than boys and can run in families.
It can also be caused by wrapping your baby tight or swaddling them, if it’s not done the safe way. If you swaddle your baby, make sure they can bend their legs.
Sometimes hip dysplasia is not obvious. It is easy for you to miss it. Doctors and early childhood nurses do regular checks so that they don’t miss it either.
They are looking for a baby who:
has uneven skin creases near the buttocks has legs which are a different length doesn’t move their legs normally has a turned-out foot And they look for an older child who:
- sits or walks late
- leans to one side when standing or walking
- waddles when they walk
Your doctor, midwife, or early childhood nurse can check your baby’s hips at any time, but often will check them during baby checks done:
- at birth
- one week after birth
- six weeks after birth
- six months after birth
- when they begin to walk
Table of Contents
Causes of Hip Dysplasia:
The exact cause of hip dysplasia is not easy to pin down, as there are thought to be several factors that contribute to the development of this condition. Hip dysplasia occurs in about 0.4% of all births and is most common in firstborn girls. Some known risk factors for a child to have hip dysplasia include:
Children with a family history of hip dysplasia
Babies born in breech position
Babies born with other “packaging problems”
Oligohydramnios (lack of intrauterine fluid)
“Packaging problems” are conditions that result in part from the in-utero position of the baby; for example, clubfoot and torticollis. Hip dysplasia most commonly occurs in first-born children, is much more common in females (80%), and occurs much more commonly on the left side (60% left hip only, 20% both hips, 20% right hip only).
Signs and Symptoms of Hip Dysplasia
Hip dysplasia in babies is most frequently discovered at the time of newborn examinations by physicians but dysplasia and dislocation can develop after this time in some children. This is why hip dysplasia is greatly considered developmental. It is also hard to detect because hip dysplasia is known as a “silent” condition. It does not cause pain in babies and doesn’t normally prevent them from learning how to walk at a normal age.
Asymmetry
Swayback posture is one of many possible signs of hip dysplasia
A baby with Swayback. Note the strong curve in the lower back.
Asymmetrical buttock creases can suggest hip dysplasia in infants but, like a hip click, an ultrasound or x-ray study will need to be done to determine whether the hips are normal or not.
Continue reading about Asymmetry.
Hip Click
Hip clicks or pops can sometimes suggest hip dysplasia but a snapping sound can occur in normal hips from developing ligaments in and around the hip joint.
Continue reading about Hip Clicks.
Limited Range of Motion
Parents may have difficulty diapering because the hips can’t fully spread.
Pain
Pain is normally not present in infants and young children with hip dysplasia, but pain is the most common symptom of hip dysplasia during adolescence or as a young adult.
Diagnose
Doctors use a combination of physical exams and imaging such as ultrasound or X-rays to diagnose hip dysplasia. Standard practice in the developed world is to do hip exams for newborns and babies for hip dysplasia at well-baby checkups.
Babies are at increased risk for hip dysplasia in the following situations:
The baby is a twin or multiple or was in a breech position at birth.
There is a family history of hip dysplasia.
The doctor is concerned about the results of the physical exam.
There are signs and symptoms of a possible hip problem, such as a limp in a child of walking age.
The American Academy of Pediatrics recommends an ultrasound study at six weeks of age for almost all baby girls who were in the breech or bottom-first position. Babies with other risk factors may also benefit from an ultrasound, especially when the pediatrician has any concerns about the examination of the hips. An x-ray at four months of age or older is sometimes recommended.
Hip dysplasia can be difficult to diagnose, especially if it is bilateral (both hips are affected) because the hips are symmetrical. The hips could be a little loose, but otherwise fine, and then get progressively worse as the baby gets older, especially if they slip farther out of the socket when the baby is relaxed, such as while sleeping. When both hips are dislocated, the exam is symmetrical.
When a baby with dislocated hips walks, he or she has a waddling gait that is a little more exaggerated than a normal toddler gait. If only one hip is affected, it is easier to spot the affected hip because it can be compared to the other hip. In some cases, hip dislocations have developed in older babies even when the infant exam was normal and the ultrasound was normal at six weeks of age. The cause of these late-developing cases is unknown.
Physiotherapy Treatment of Hip dysplasia
The treatment of hip dysplasia depends on the age of the child. The goal of treatment is to properly position the hip joint (“reduce” the hip). Once an adequate reduction is obtained, the doctor will hold the hip in that reduced position and allow the body to adapt to the new position. The younger the child, the better capacity to adapt the hip, and the better the chance of full recovery. Over time, the body becomes less accommodating to the repositioning of the hip joint. While treatment of hip dysplasia varies for each individual baby, a general outline follows:
Birth to 6 months
Generally, in newborns, hip dysplasia will be reduced with the use of a special brace called a Pavlik harness. This brace holds the baby’s hips in a position that keeps the joint reduced. Over time, the body adapts to the correct position, and the hip joint begins normal formation. About 90% of newborns with hip dysplasia treated in a Pavlik harness will recover fully. Many doctors will not initiate Pavlik harness treatment for several weeks after birth.
6 months to 1 year
In older babies, Pavlik harness treatment may not be successful. In this case, your orthopedic surgeon will place the child under general anesthesia. This usually allows the hip to assume the proper position. Once in this position, the child will be placed in a spica cast. The cast is similar to the Pavlik harness but allows less movement. This is needed in older children to better maintain the position of the hip joint.
Over age 1 year
Children older than one year old often need surgery to reduce the hip joint into proper position. The body can form scar tissue that prevents the hip from assuming its proper position, and surgery is needed to properly position the hip joint. Once this is done, the child will have a spica cast to hold the hip in the proper position.
The success of treatment depends on the age of the child and the adequacy of the reduction. In a newborn infant with a good reduction, there is a very good chance of full recovery. When treatment begins at older ages, the chance of full recovery decreases. Children who have persistent hip dysplasia have a chance of developing pain and early hip arthritis later in life. Surgery to cut and realign the bones (hip osteotomy), or a hip replacement, may be needed later in life.
Movements of the hip and gentle stretching exercises are recommended because motion may help lubricate and nourish the joint surfaces. Try to maintain hip motion in all directions unless there is pinching in one particular position. Stretching exercises can be performed to move your leg away from your body in the lying position and in the sitting position. Also gently roll your legs in and then out as far as possible to stretch hip rotation. When lying down, pull one knee to your chest while the other leg is lying as flat as possible on the floor, then repeat with the opposite knee. All stretches should be held for 15-30 seconds in the most stretched position. Stretching for as little as 10 minutes a day can make a big difference in flexibility.

When working on hip strengthening exercises concentrate on hip abduction (moving your leg, at the hip, out to the side, away from the body) and external rotation (rotation of your hip away from the body)
Examples of Hip Abduction exercises:
Lying Hip Abduction Standing Resisted Hip Abduction Bent Knee Hip Abduction Resisted with Band
If you have a leg length discrepancy, a heel lift may be added to your shoe to reduce pain and help with your walking pattern. A physician’s prescription may be required for an orthotist to appropriately prescribe an orthotic. The Physical Therapist can then manage the muscle strengthening, walking pattern, and home program for the patient.
If you have a leg length discrepancy, an insole can be inserted in your shoe or a heel lift may be added to your shoe. Up to 3/8 inch can usually be placed inside a shoe without any problem. When more is needed you should probably obtain a prescription from a physician to have the lift added to the heel of your shoe. A shoe lift occasionally helps reduce pain and improve walking pattern. Other everyday recommendations would include taking the elevator to avoid using stairs and using ice after a busy day to help reduce pain and possibly allow you to better manage your symptoms.
As a general rule, heat is preferred before activities and ice afterwards (like a warming up and cooling down a race horse), However, heat in the evening helps some people because heat helps muscles relax and increases blood flow to the area. Cold is always used to reduce swelling for the first few hours after a fresh injury, but there isn’t a right or wrong answer about heat or cold for pain relief for arthritis. Other everyday recommendations would include taking the elevator to avoid using stairs and using ice after a busy day to help reduce pain and possibly allow you to better manage your symptoms. Depending on the level of dysplasia this may require one or two visits with a local Physical Therapist to teach you the correct way to exercise without causing damage to your hip.



3 Comments