
Femur Bone
Table of Contents
Introduction
The longest, most oblong, and strongest bone in the human body is the femur. The spherical head at the apex and the cylindrical shaft at the base are joined at the proximal end by the pyramid-shaped neck. Additionally, two primary bony protrusions connect to the forces that move the hip and knee: the larger trochanter and the smaller trochanter. The inclination angle, also known as the curve between the neck and shaft, is approximately 128 degrees for the typical adult. The inclination angle, on the other hand, decreases with age.
The acetabulum of the pelvis, which encompasses the femoral head, forms the hip, a ball-in-socket joint. The head is shown from the best, medial, and slightly anterior positions. The acetabulum is connected to the fovea capitis femoris, a crater on the head, by the ligamentum teres femoris.
The post has a slight turn in the front. The medial and lateral condyles form a cuboidal base at the distal femur, where the shaft spreads out in a cone shape. The femur and tibia, including the knee joint, are joined by the medial and sideward condyles.
The synovial joints in the hips and knees are covered in cartilage to prevent friction and increase the range of motion. For measuring the axis that runs along the femur, bony parts are junctures.
Structure and Function of Femur Bone
The femur has two round futures and a long shaft in the middle. It’s the classic shape employed for bones in funnies: A cylinder with two rounded bumps at the individual end. Though it’s one long bone, your femur is created up of several parts. These contain: Femur proximal aspectThe upper (proximal) end of your femur attaches to your hip joint.
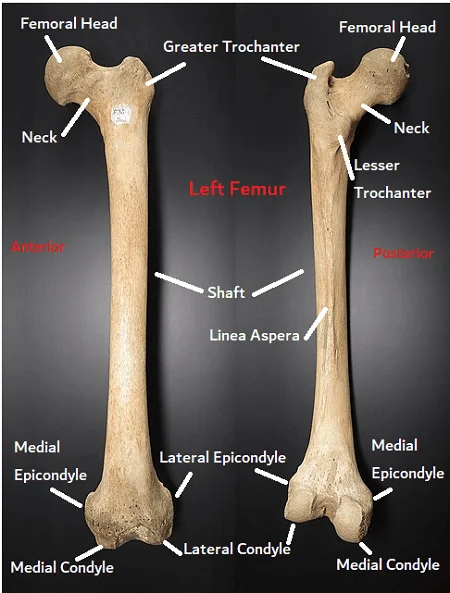
The proximal end (aspect) contains the:
- Head.
- Neck.
- Greater trochanter.
- Lesser trochanter.
- Intertrochanteric line and crest.
Femur shaft
The thigh’s structure is supported by the long portion of the femur known as the shaft. It has a slight inclination toward your center. Your femur’s shaft includes the following:
- Linea Aspera.
- Gluteal tuberosity.
- Pectineal line.
- Popliteal fossa.
Femur distal aspect
The lower (distal) end of the femur forms the top of the knee joint. It meets the tibia (shin) and patella (kneecap). It includes the:
- Medial and lateral condyles.
- Medial and lateral epicondyles.
- Intercondylar fossa.
Most of the time, your healthcare provider will use all of these parts and labels to explain where you’re having problems or pain. If you ever suffer a femoral fracture, also known as a femoral fracture, your doctor might use some of these terms to describe the location of the damage to your bone. The femur is the body’s largest bone. The average length of an adult femur is 18 inches. Additionally, the femur is the body’s strongest bone. It can uphold as much as multiple times the heaviness of your body.
The femur’s primary function is to support weight and stabilize gait. Two femoral heads bear the weight of an upper body. The acetabulum, periosteum, and proximal femur are all covered by a robust, thick sheath known as the capsular ligament. It secures the femoral head within the pelvic acetabulum. The capsular tendon cutoff points inside turn yet consider the outer pivot.
The knee is a hinge joint that connects the proximal tibia and the distal femur. Average and horizontal meniscus settle and pad the tibiofemoral enunciation. Valgus or varus deformity is prevented by medial and lateral ligaments. The anterior and posterior cruciate ligaments keep the tibia from moving either anteriorly or posteriorly within the knee joint, allowing for some rotational movement of the knee. In knee extension, the patellofemoral joint is used.
Blood Supply and Lymphatics
The primary blood supply to the lower extremities comes from the femoral artery. After the external iliac artery crosses the ilioinguinal ligament, this is the major branch. The average circumflex and anastomoses mostly supply the femoral head with the parallel circumflex course and obturator artery. Average and sidelong circumflex are parts of the femoral vein. However, the internal iliac artery branches off into the obturator artery. As a supporting blood supply to the femoral head, the foveal artery comes off of the obturator artery that runs through the ligamentum teres femoris, but it is not the primary source. The femoral artery divides into the deep and superficial femoral arteries at the level of the lesser trochanter. The femur’s shaft and distal portion are supplied by perforating branches of the deep femoral artery.
Muscles related to Femur Bone
The anterior, medial, posterior, and gluteal compartments make up the thigh muscles. The femur sits inside the foremost compartment.
The muscles in the anterior compartment are mostly used for hip flexion and knee extension. The pectineus, iliopsoas, and sartorius muscles are all hip flexors. Except for the iliopsoas, all of the hip flexors are innervated by the femoral nerve. The psoas major and iliacus muscles make up the iliopsoas muscle, which is the strongest hip flexor. The psoas major muscle joins the pelvic iliacus muscle at the lesser trochanter of the femur. It comes from the posterior abdominal wall.
Back compartment muscles are chiefly hip extensors and knee flexors. It is comprised of bicep femoris, semitendinous, and semimembranous muscles. Except for the bicep femoris, most posterior thigh muscles are innervated by the sciatic nerve’s tibial division. The long and short heads of the bicep femoris are its two heads. The sciatic nerve’s tibial branch supplies the long head. The sciatic nerve’s common peroneal (fibular) division innervates the short head.
Muscles in both shallow and deep layers organize the gluteus. The superficial layer is made up of the gluteus maximus, medius, and minimus. The primary functions of the superficial gluteal are hip extension, abduction, and internal rotation. The gluteus medius and minimus are innervated by the unrivaled gluteal nerve. The inferior gluteal innervates the Gluteus maximus. The piriformis, obturator internus, quadratus femoris, and superior and inferior gemellus make up the deep layer.The largest and longest nerve in the body is the sciatic nerve. It travels through the storied and piriform Gemelli. These gluteal muscles, which are more numerous and smaller, support the exterior rotation of the hip.
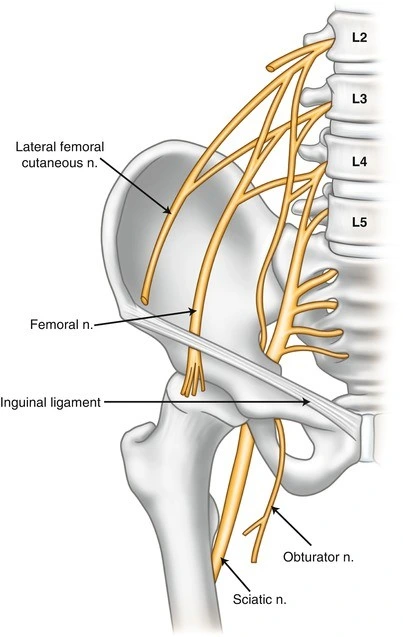
The primary function of the medial compartment is leg adduction. It includes the gracilis, obturator externus, adductor longus, adductor brevis, and adductor magnus. The obturator nerve, which originates in the lumbar plexus, is the primary nerve that innervates the medial compartment.
Ligaments
Stability is improved by the hip joint’s ligaments. They fall into one of two categories: intracapsular or extracapsular.
Intracapsular
The only intracapsular ligamentcle is the femur head ligament femur’s fovea and is relatively small. It contains a minor arterial supply to the hip joint-supplying branch of the obturator artery or artery to the head of the femur.
Extracapsular
There are three fundamental extracapsular tendons, consistent with the external surface of the hip joint container:
The iliofemoral ligament: The divides at the anterior inferior iliac spine before inserting into the femur’s intertrochanteric line. It has a shape resembling a “Y” and stops the hip joint from being too stretched out. Of the three ligaments, it is the strongest.
The pubofemoral: strengthen the capsule anteriorly and inferiorly by joining the superior pubic rami to the femur’s intertrochanteric line. It has a triangular form and avoids excessive abduction and extension.
Ischiofemoral: This ligament connects the ischium’s body to the femur’s greater trochanter, supporting the capsule posteriorly.
It holds the femoral head in the acetabulum, prevents hyperextension, and has a spiral orientation.
Movements and Muscles
The primary muscles responsible for each movement are listed below, along with the movements that can be performed at the hip joint:
- Extension – gluteus Maximus;
- Flexion – iliopsoas, rectus femoris, sartorius, and pectineus are all involved in flexion;
- Abduction involves the gluteus medius, gluteus minimus, biceps femoris, and tensor fascia latae.
- Adduction involves the adductors longus, brevis, and magnus, pectineus, and gracilis.
- Lateral rotation involves the biceps femoris, gluteus maximus, and piriformis, with assistance from the obturators, gemilli,
Tensor fascia lata and the anterior fibers of the gluteus medius and minimus are involved in the medial rotation. The degree to which the hip can be flexed depends on whether the knee is flexed, which makes the hamstring muscles more flexible and expands the range of flexion.
The joint troche and iliofemoral ligament restrict hip joint extension. During extension, these structures become taut to prevent further movement.
Femur fractures
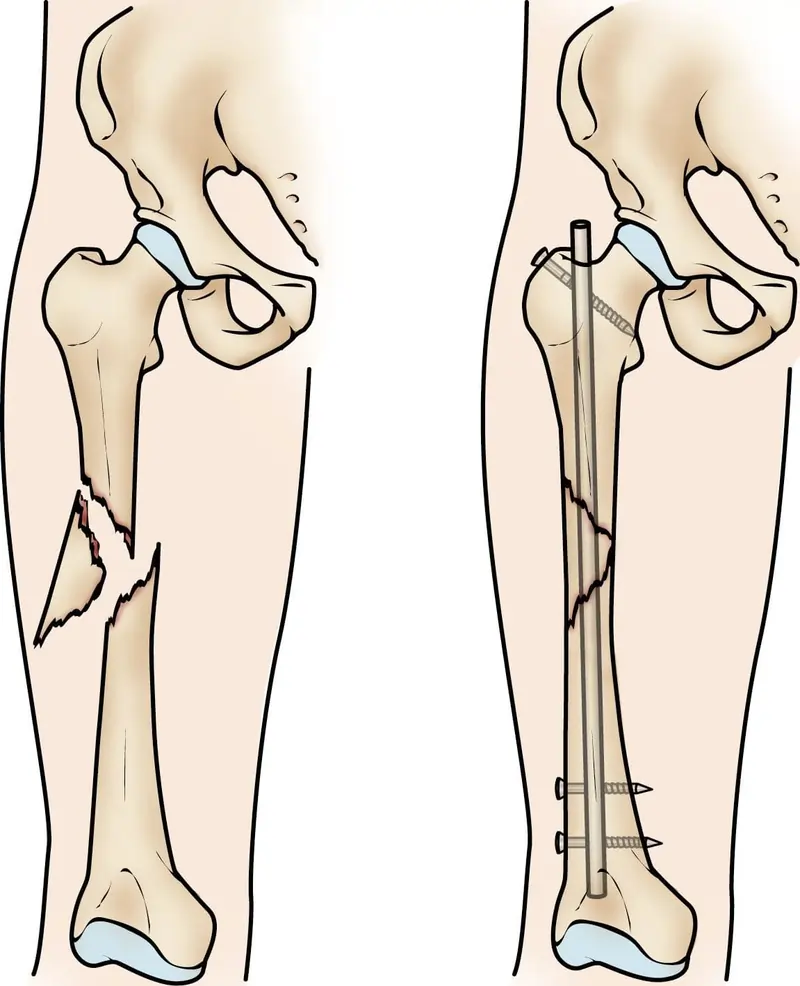
Breaking a bone is referred to as a bone fracture in medicine. Femurs are only typically broken by severe injuries like car accidents, falls, or other traumas due to their strength. Among the signs of a fracture are:
- Pain.
- Swelling.
- Tenderness.
- incapacity to move your leg as normally.
- swollen or discolored skin.
- A deformation or knock that is not typically on your body.
- If you’ve been hurt or think you have a fracture, go to the hospital right away.
Osteoporosis
Bones become weaker as a result of osteoporosis, increasing their susceptibility to sudden fractures. A lot of people don’t realize they have osteoporosis until they break a bone. There normally aren’t clear side effects. Osteoporosis is more likely to affect women, people who were born female, and adults over 50. Ask your doctor about getting a bone density test, which can detect osteoporosis before it leads to a fracture.
Patellofemoral pain syndrome
Pain under and around your kneecap (patella) is known as patellofemoral pain syndrome (PFPS). It is sometimes referred to as jumper’s or runner’s knee. Overuse of the knees or purchasing new shoes can all lead to PFPS.
Pain when bending your knee, such as when squatting or climbing stairs, is one of the PFPS symptoms.
When you sit with your knees bent, pain.
When you stand up or climb stairs, your knee makes crackling or popping sounds.
Changes to your usual playing surface, sports equipment, or activity intensity cause pain to worsen.
If you’re experiencing new knee pain, talk to your doctor.
A bone density test is the most common way to check your femur’s health. Occasionally, it is referred to as a DEXA or DXA scan. Using low doses of X-rays, a bone density test determines how strong your bones are. It is a method for evaluating bone loss with age. If you have a femoral fracture, your doctor or surgeon may require imaging tests, such as: What kind of treatment is given to your fracture and what caused it? For your bone to heal from Osteoporosis treatment, you will need some form of immobilization, such as a cast or splint, and you may need surgery to realign (set) it. Exercise, vitamin and mineral supplements, and medications are all options for osteoporosis treatment.
Most of the time, all you need to do to prevent osteoporosis is exercise and take supplements. A treatment plan that is tailored to your needs and your bone health will be developed with your provider’s assistance.
Surgical Considerations
Older female patients are more likely to have osteoporosis, which makes them more likely to break their bones when they fall to the ground. Young patients frequently suffer femur fractures as a result of high-energy trauma like car accidents or fall from a significant height due to the strength of the femur bone. Except if the patients have high careful dangers or extreme comorbidities, all femur breaks are overseen operatively to permit patients prior ambulation and work on personal satisfaction. Aseptic nonunion, periprosthetic fracture and avascular necrosis are the most common complications that necessitate a revision.
The fracture pattern and characteristics influence the choice between arthroplasty and internal fixation for a proximal femur fracture. A femoral neck intracapsular fracture is more likely than an extracapsular fracture to cut off blood supply to the deep branch of the medial femoral circumflex artery. Since intramedullary (IM) nails and screws run the risk of avascular necrosis, arthroplasty with femoral head replacement is preferable.
Using the Garden classification, plain film X-rays are used to evaluate femoral neck fractures. Garden I is a minimally displaced or valgus-impacted incomplete femoral neck fracture. Garden II is a fracture that is complete and only slightly displaced. Garden III is a complete fracture with a displacement of less than 50%. Garden IV is a complete fracture that has been displaced by more than half. However, femoral neck fractures are typically classified as displaced (Garden I and II) or nondisplaced (Garden III and IV) due to the difficulty of X-ray classification. Cancellous lag screws or sliding hip screws are utilized for the treatment of nondisplaced fractures. The outcomes and complications of the two methods are roughly comparable. Less blood loss and a shorter operating time are associated with cancellous lag screws. However, as the femoral neck naturally shortens after surgery, cancellous lag screws also have a higher revision rate than sliding hip screws. This is because the lag screw head frequently irritates soft tissue.
Because more than half of distal femur fractures are intra-articular and the type of surgical treatment depends on whether there is involvement in the joint space, distal femur fractures are complex injuries that require a CT scan to evaluate. Anterograde or retrograde intramedullary (IM) nails, plates, blades, or screws are used to treat extra-articular fractures. When compared to open reduction internal fixation with a plate, blade, or screw, retrograde IM nail has superior outcomes and lower rates of revision and infection. The outcomes of an anterior IM nail and a retrograde IM nail are comparable. Retrograde intraarticular nails can be used to treat some stable and undisplaced intra-articular fractures, but total knee arthroplasty (TKA) should be used to treat most of them. However, patient selection is crucial because elderly patients undergoing TKA have a high rate of morbidity and mortality. The outcomes of TKA revisions are worse than those of primary TKA.
Clinical importance
Adolescent Hip Disorder
A hip disorder of the femoral head known as slipped capital femoral epiphysis (SCFE) is most common in overweight male adolescents. SCFE is a metaphysis-to-epiphysis displacement that occurs anteriorly and superiorly. SCFE has been linked to endocrine dysfunction, renal failure, or radiation therapy, although the cause is typically idiopathic. A common complication of SCFE is a femoroacetabular impingement. Although early treatment with a single screw through the growth plate has been shown to prevent progressive slippage, preventative treatment for SCFE is controversial. As of late, the adjusted Dunn technique has been read up for serious SCFE. The modified Dunn procedure involves fixing the femoral head with screws and removing a wedge from the femoral neck to correct the deformity. With the modified Dunn procedure, common post-surgical complications included persistent hip pain and avascular necrosis.
A rare childhood condition known as Vascular Legg-Calve-Perthes disease (LCP) occurs when the blood supply to the femoral head is disrupted. Hip pain and limping are symptoms. Boys are five times more likely than girls to develop LCP, which typically appears between the ages of 4 and 8. According to twin studies, environmental factors like low social class increase the likelihood of LCP. It is likewise connected with innate deformities like genitourinary anomalies, inguinal hernias, or Down condition. The board relies upon the youngster’s age and infection stage. LCP treatment options include acupuncture, exercise, braces, bisphosphonates, and hip arthroscopy.
The characteristic long bone deformity that characterizes environmental rickets is caused by an inability to mineralize bone. The primary method by which the growth plate calcifies and encourages long bone growth is through endochondral ossification. However, in rickets, this process is diminished or absent. Rickets is typically brought on by a lack of vitamin D. A lack of calcium or phosphate intake, insufficient sun exposure, and abnormal phosphate metabolism are additional causes.
Keeping your femur healthy You can keep your bone and overall health in good shape by eating well, exercising regularly, and going to your doctor for regular checkups. A bone density scan is something you should discuss with your doctor if you are older than 50 or have osteoporosis in your family.
Follow these overall well-being tips to decrease your gamble of a physical issue:
- Always buckle up when driving.
- Wear the right defensive hardware for movements of every kind and sport.
- Clutter that could impede your safety or that of others should be removed from your workspace and home.
- At home, always use the right tools or equipment to reach things. Never stand on countertops, chairs, or tables.
- You can maintain good bone health by following a diet and exercise plan.
- If you have trouble walking or are more likely to fall, use a walker or cane.
- A note from Cleveland Center
Your femur gives you any grounds to be taken seriously, in a real sense. It’s the greatest, most grounded, and most significant bone in your body. Converse with your supplier about your osteoporosis risk. Your bones will stay strong no matter what you do to improve your overall health.
FAQs
The femur has two adjusted closes and a long shaft in the center. It’s the standard shape that cartoon bones take: a cylinder with two ends that have round bumps.
The following is at the proximal end (aspect):
Head.
Neck.
The trochanter is larger.
smaller trochanter
Crest and intertrochanteric line.
Not only does the femur have a cool name, but it is also a fantastic bone.
The body’s longest bone is the femur.
A bone that supports weight is the femur.
For the gluteal muscles and other muscles that rotate the thigh, the greater trochanter provides leverage.
The name “thigh bone” comes from the Latin word for “femur,” which means “thigh.” The femoral head is the end of the thigh bone that is closest to the heart (the proximal end). The ball of the ball-and-socket hip joint can be found here.
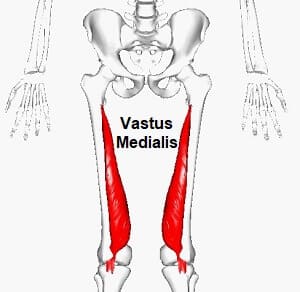
The rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius are the four major muscles that make up the quadriceps. One of the body’s strongest muscle groups, the quadriceps femoris covers the anterior aspect of the femur. This gathering of muscles has a typical capability. At the knee joint, they extend their leg.
The profound femoris, which is the deep penetrating branch of the upper thigh, supplies the majority of the blood supply to the head of the femur through the medial and lateral circumflex branches of the femoral artery.


17 Comments