“A COMPARATIVE STUDY OF HOLMICH V/S COPENHAGEN EXERCISE PROTOCOL IN ADDUCTOR-RELATED GROIN PAIN IN MALE FOOTBALL PLAYERS.”
Table of Contents
LIST OF ABBREVIATION
• ARGP : Adductor-related groin pain • HAGOS : Hip and Groin Pain Outcome Score • HHD : Hand Held Dynamometer
• SD : Standard Deviation
ABSTRACT
TITLE: “A Comparative Study of Holmich vs. Copenhagen Exercise Protocol in Adductor Related Groin Pain in Male Football Players.”
BACKGROUND: Football is the most popular sport play worldwide. Due to repetitive rotational movements like turning, kicking there is a higher chance of groin injuries. Adductor-related groin pain is a common football injury but it is most often neglected by players. Adductor longus muscle is highly affected during groin injuries. Strengthening of adductor longus and structure around it is very important; otherwise, there are higher chances of great injuries. The squeeze test is widely used to examine adductor-related groin pain, a handheld dynamometer is the best device to check the strength of hip muscles and HAGOS is a valid and reliable outcome questionnaire for the young to middle age physically fit individual with hip and groin pain.
Copenhagen and Holmich are the most reliable exercise protocols for the patient with adductor related groin pain. Copenhagen adductor exercise focuses on eccentric muscle contraction which helps to improve the strength of the adductor muscles. Holmich exercise protocol includes high-intensity strengthening, core stability exercise, isometric contractions, and functional activities that will help to improve functional activity of hip muscles and decreases the pain. ARGP can be prevented significantly through better exercise protocol by motivating players to perform exercise regularly.
METHOD: The study was conducted at football court Total 32 players with adductor-related groin pain (examine by squeeze test) took part in the evaluation program. They were randomly categorized into two groups. [Group 1 (Holmich exercise protocol) and group 2(Copenhagen exercise protocol)] Exercise protocols were given for two weeks (alternative days) to the players. Dynamometry and the HAGO’s questionnaire were used to assess improvement before and after exercise.
RESULT: The age of players is between 18 to 30. The data were analyzed using the Mann Whitney U Test in SPSS version 20. There is a significant improvement in the hip adductors strength and hip muscle function (hip and groin pain outcome score) through Copenhagen exercise protocol in male Football players with ARGP. For Holmich exercise program (pre-HHD=26.25±3.87,post-HHD=32.504.47 and pre
HAGOS=72.94±10.31, post-HAGOS=90.37±4.24) and for Copenhagen exercise protocol (pre-HHD=24.37±5.74, post-HHD=36.56±5.98 and pre HAGOS=75.81±10.52, post-HAGOS=82.81±7.34). In the Mann-Whitney test, HHD for the Copenhagen exercise protocol is 19.63 and for the Holmich exercise protocol, it is 13.38 that suggests that using the Copenhagen exercise protocol there is significant improvement seen in the strength of adductors(U=78.00,sig.=0.06). In the same test HAGO’s for Copenhagen exercise protocol is 11.66 and for Holmich exercise protocol, it is 21.34 that suggest that using the Holmich exercise protocol, there is significant improvement seen in parameters included in HAGOS.
CONCLUSION: This study shows, in the Copenhagen exercise protocol, there is marked increase in hip adductors strength, and in Holmich exercise protocol, there is marked increase in hip and groin outcome score.
KEYWORDS: Adductor strengthening, squeeze test, HHD, HAGOS, Copenhagen exercise, Holmich exercise, Groin pain.
INTRODUCTION
Football, also known as soccer, is one of the most popular sports in the world. Football is played by 200.000 professional and 240 million amateur players worldwide.1
Football is a high-contact, high-intensity sport. The sport’s high impact and repetitive rotational motions, such as kicking and spinning, can leave players sidelined with a number of football injuries.2
Football injuries are common, even when proper protective equipment is worn, and can range from mild aches and pains to severe, traumatic injuries. Overuse injuries can occur in any sport that involves running, but football players are regularly exposed to being tackled, dropping, and abrupt changes in running direction, both of which increase the risk of acute injuries.3
Ankle sprains and knee injuries are also common football injuries. Strains of the quadriceps, hamstrings, and groin, hip pointers, shoulder dislocations, AC joint sprains, wrist and hand injuries, and football concussions are all common injuries.2In football, adductor strain, also known as groin strain, is most likely due to sudden starts and stops while running and jumping.
Groin injuries are common in sports, accounting for two to five percent of all injuries, and they can vary in severity depending on the athlete’s age, gender, and sport.4
The three most common entities assessed in a population of 207 athletes included adductor-related, iliopsoas-related & abdominal-related pain.
There are 20(10%) patients found with Rectus abdominis related dysfunction but it is associated with adductor related pain in 18 of these patients, iliopsoas related dysfunction was found in 36 percent of the patient and 69(33%) patients were found with multiple clinical entities and 16 patients have three clinical entities.5
While adductor-related pain is the most common, there are no clear diagnostic guidelines or definitions for these issues. Adductor-related groin pain may be acute, resulting from a strain of the myo-tendinous junction, or chronic, resulting in pubic bone tenderness.6
Adductor related pain was more common in male football players and athletes. Interestingly, adductor related pain was observed to be rare in the female athletes. This could be due to the anatomical variation of a wider pelvis. Which may make the female athlete more susceptible to hip and iliopsoas related presentation.
The most common cause of acute groin pain is a strain of the adductor muscle group (adductor longus, brevis, gracilis, pectineus, and obturators externus). Their primary function in a closed kinetic chair is to stabilize the lower extremity and pelvis, as well as adduction of the thigh in an open kinetic chain and assisting in femoral flexion and rotation.
Strain are common with sudden eccentric loading. The adductor longus is most likely affected due to its lack of mechanical advantage.
Macintyre did study of soccer player found that preseason hip abduction ROM was decreases in players who were subsequently injured.
Evaluation of Groin pain :
The complexity of groin anatomy and groin injury to make challenge to be diagnosed.9
There are three evaluation tools used in this study:
• Adductor Squeeze Test
• Adductor Muscle Strength Test by HHD
• HAGOS Questionnaire
In the evaluation of adductor-related groin pain and injuries, the Adductor Squeeze Test (ICC-0.92) is widely used. Verrall et al.10characterize it as requiring the patient to grip the examiner’s fist, which is positioned between the patient’s knee and the examiner’s fist, with the hip joint in 45 degrees of flexion and the feet resting on a plinth, and basically consists of an isometric adduction against the examiner’s fist with the athlete lying supine.
HHD (ICC-0.62-0.70) is widely used to assess adductor muscle ability. HHD is a compact and easy-to-use device that is used in clinical practice to measure isometric muscle strength.11It has been shown by many researchers to have significant advantages in terms of portability and ease of use.
Assessment of maximal hip muscle strength in patients with Acute hip and/or groin pain has been commonly used in clinical settings to measure strength profiles, track treatment progression and efficacy, and risk stratification.
For hip adduction person being tested was in the supine position, with the test leg placed at the end of the table and opposite leg slightly flexed and the dynamometer is placed 5 cm proximal to the medial malleolus.
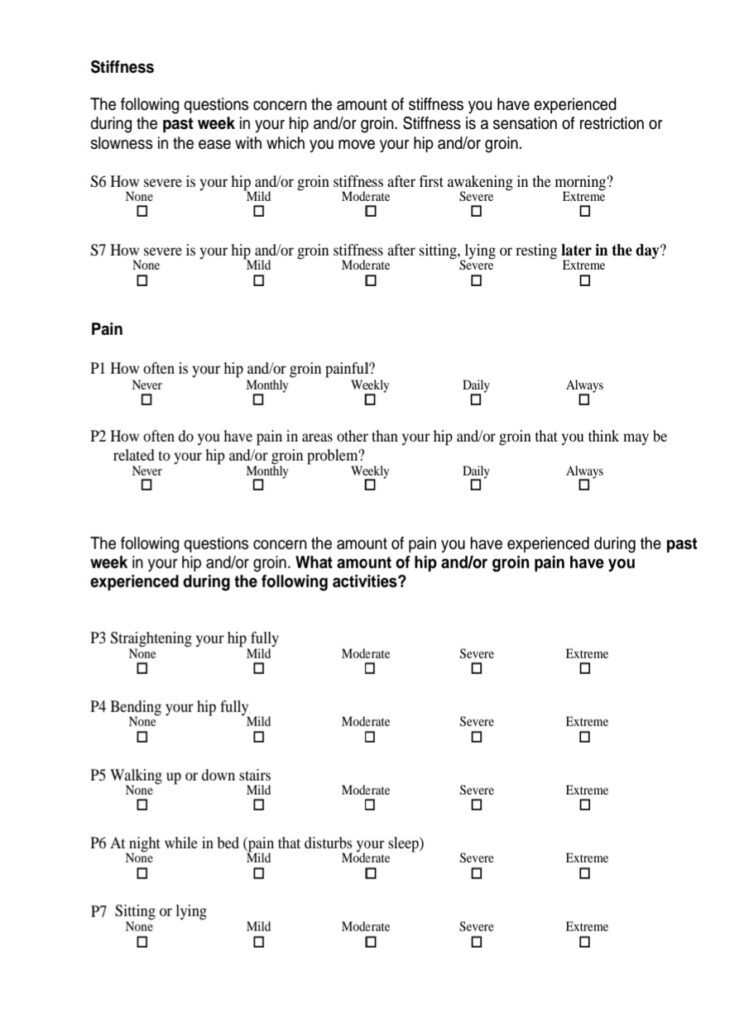
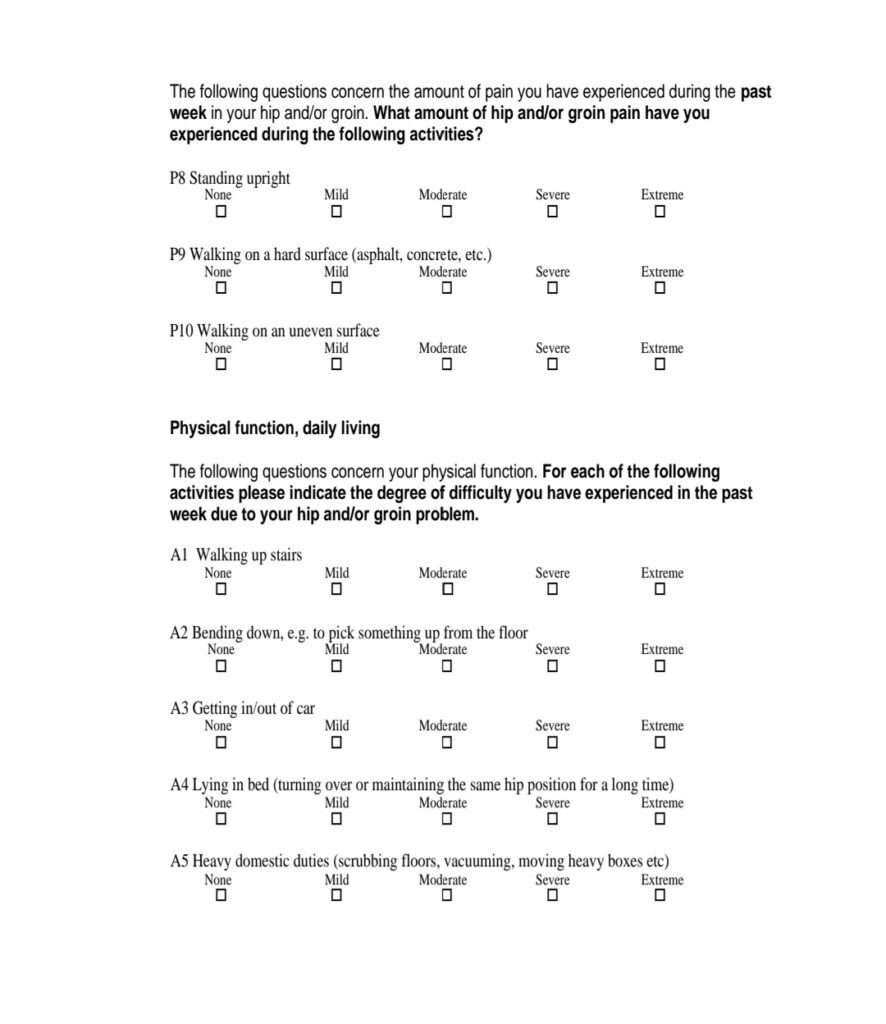
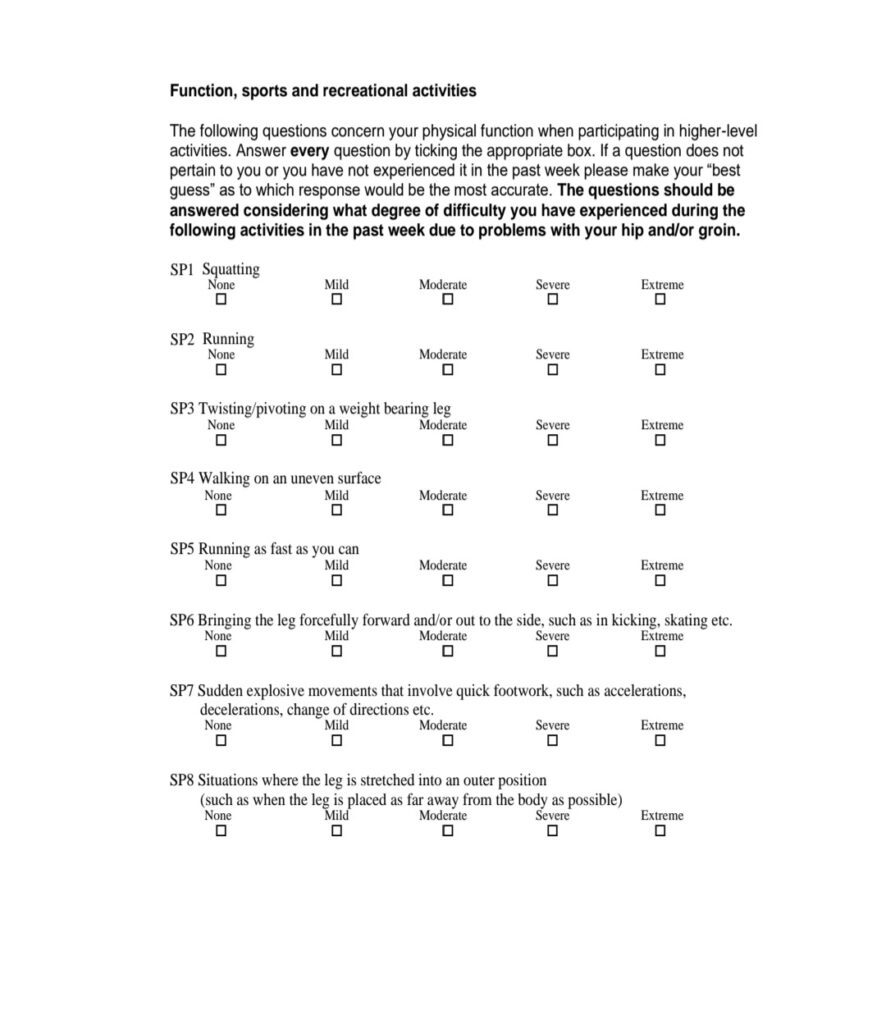
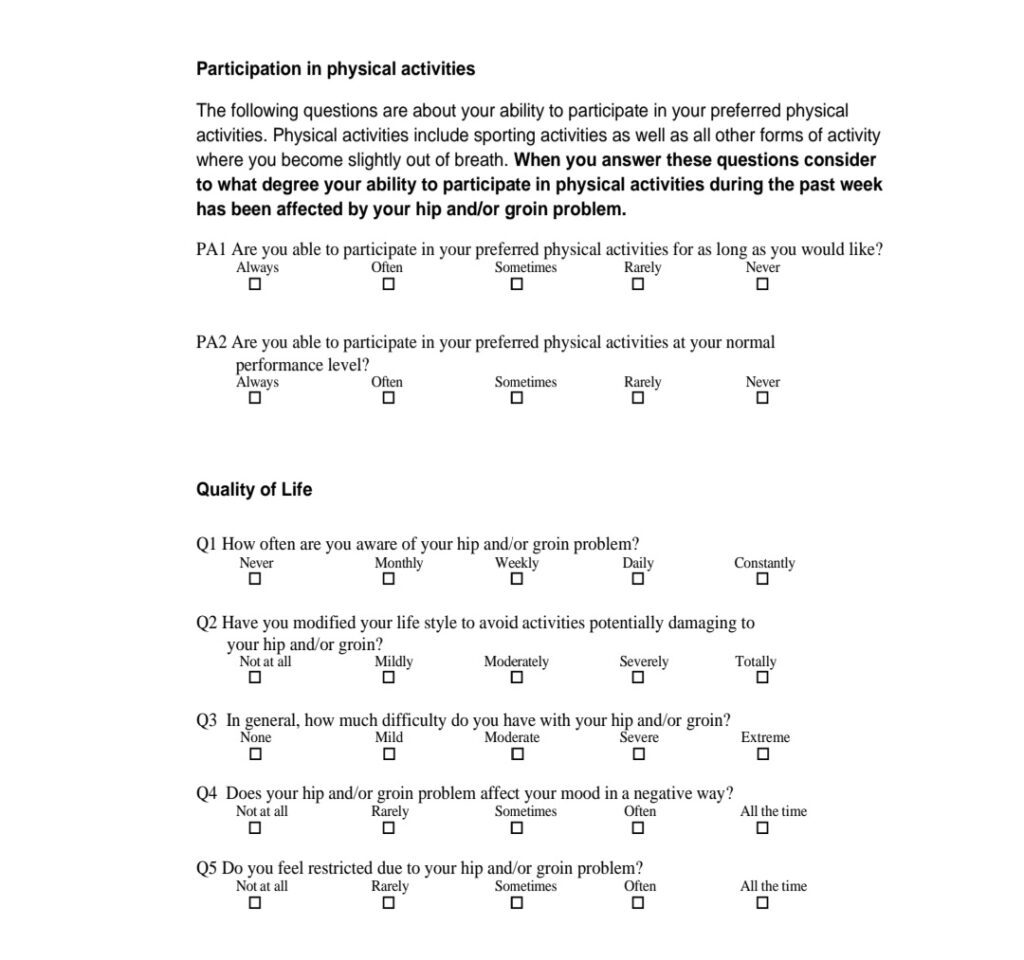
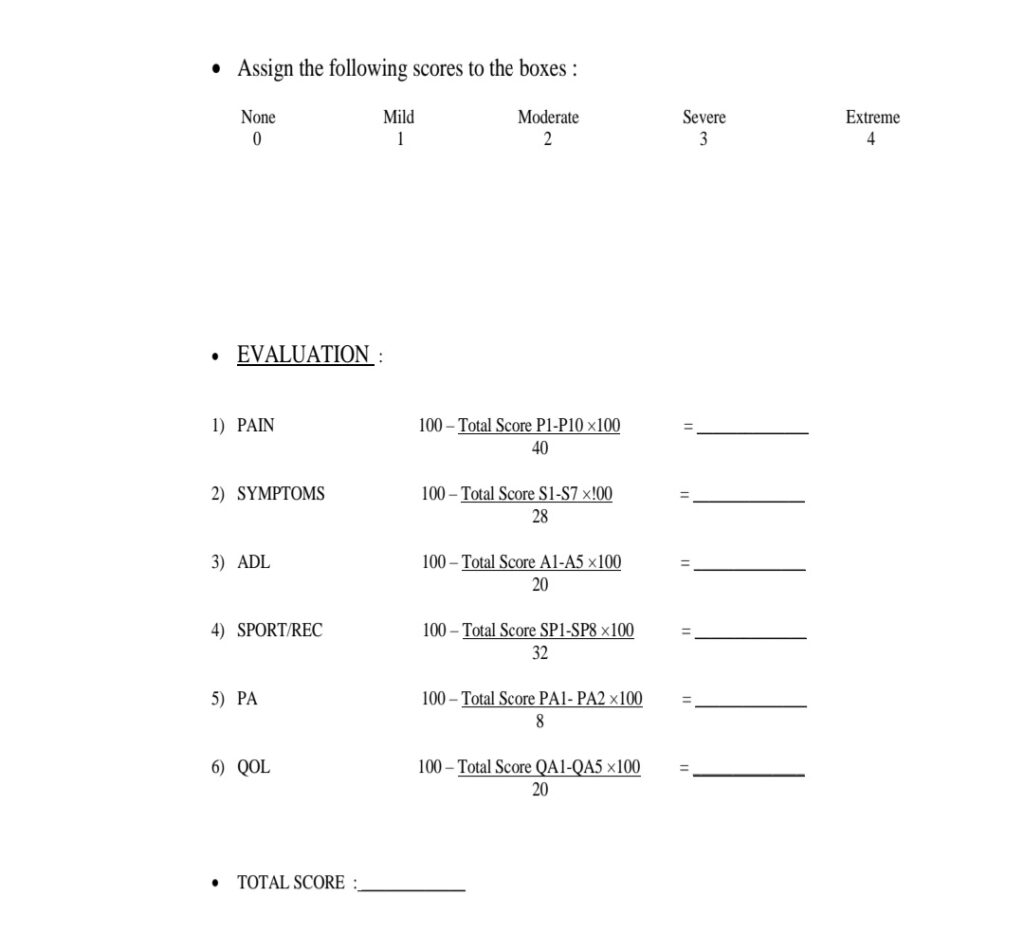
The HAGOS Scale is valid (ICC-0,82-0,91).13 Patient-reported outcome questionnaire for young to middle-aged physically fit individuals with hip and groin dysfunctions. The HAGOS Scale has six subscales to assess Pain (10 things), Symptoms (7 things), Physical Function in Sport and Recreation (8 things), Participation in Physical Activities (2 things), and Hip and/or Groin related Quality of Life (5 things). It has 37 things in total.
Treatment of ARGP :
There are many treatment protocols for ARGP, but the Holmich Protocol and the Copenhagen Protocol are the most accurate. A clinical trial carried out through Holmich and Copenhagen exercise protocol still afford the best evidence for the effectiveness of exercise as a treatment of ARGP.
Copenhagen Exercise Protocol :
The Copenhagen exercise, also known as the adductor strengthening protocol, is a dynamic and high-intensity exercise. It doesn’t require any special equipment and can be done in any training center. The Copenhagen exercise protocol is unique in that it consists of a single exercise with varying degrees of progression. In male football players, it also reduces the chance of groin-related problems.
Holmich Exercise Protocol :
Holmich continues to provide the strongest evidence for the efficacy of exercise as an ARGP treatment.
It was first defined in the Lancet in 1999 by Per Holmich, and it is still one of the most well-validated programs for chronic ARGP. Yousefzadeh, Shadmehr, Naseri, and Khazaeipour validated the protocol in 2018. They discovered the Holmich protocol for acute ARGP.15
The Holmich treatment protocol exercise includes static and dynamic and/or isometric and isotonic strengthening exercises for hip adductors and abductors and also for abdominal muscles.
The total duration of the protocol is 10 weeks in that there are 2 modules of the exercise was used three times a week for two weeks and the duration of each session was about 90 minutes.
A recent research comparing the efficacy of the Copenhagen and Holmich exercise protocols was found to be inconclusive. As a result, the efficacy of both protocols will be compared in this analysis to determine which is the better exercise protocol in acute ARBG
NEED OF STUDY
• The Copenhagen & Holmich exercise protocol is an effective treatment for ARGP. But the comparison of these protocols has not yet been proved. So it will compare both Holmich and Copenhagen exercises to see which is the best exercise protocol in ARGP.
AIMS AND OBJECTIVES
➢ AIMS :
• To compare the effect of Holmich vs Copenhagen exercise protocol on adductor related groin pain in male football players.
➢ OBJECTIVES :
• To see the effect of Holmich exercise on adductor related groin pain in male football players.
• To see the effect of Copenhagen exercise on adductor related groin pain in male football player
HYPOTHESIS
• Null Hypothesis : There is no significant difference in adductor-related groin pain between the Copenhagen and the Holmich protocol.
• Alternative Hypothesis : There is significant difference in adductor-related groin pain between the Copenhagen and the Holmich protocol.
REVIEW OF LITERATURE
1) Armi Arneson, Stefan B Sigurdsson, et.al. (2004) :
American journal of Sports Medicine : Assessing risk factor for injuries in football. They examined 306 male football players as part of a report on risk factors for football injuries. They looked at people’s heights, weights, and ages. Previous injury and body composition They come to the conclusion that older players have a P = 0.05 risk of being injured. Decrease hip ROM (P = 0.05) for groin pain (P = 0.01). According to them, the primary risk factors for football injuries are previous injury and age.
2) Holmich (1997) : Sports Medicine & Arthroscopic Review, Assessing ARGP in athletes and Conducted that adductor-related pain is the most frequent symptom and accurate clinical examination is essential for choosing the right treatment described in this literature. He concludes that the treatment of acute
adductor strain should include ROM exercise, stretching, and strengthening exercises.
3) Zazen Machotka, Saravana Kamar, et.al. (March 2009) : Sports Medicine Arthroscopic Rehabilitation : they did study on systemic on the effectiveness of exercise therapy for groin pain in athletes. There are 468 studies in all, 12 of which are potentially relevant. This analysis includes 5 of those studies. This study provided evidence that exercise produces the best results in sports. Functional and strengthening exercise interventions is used in five to four of the studies. The duration of the intervention ranges from 3.8 to 16 weeks. They came to the conclusion that exercise therapy is the best evidence-based rehabilitation program for football players with groin pain. They also came to the conclusion that strengthening hip and abdominal muscles is an important treatment for groin pai4)
4)Magmas K. Kerrison, R. Duhon, et.al. (August 2014) : The journal of Sports Medicine & Physical Fitness : They studied on occurrence of groin pain in male v/s female football players. In this study, 479 male football players aged 17 to 43 and 144 female football players aged 16 to 47 actively participated. They used a specific questionnaire that contained specific questions about groin pain and athletic history. According to the study, males experience pain at a rate of 55 percent, while females experience pain at a rate of 28 percent. As a result, they concluded that male football players are more susceptible to groin pain.
5) V. Moreno Perez, B. Travessa, et.al. (2019) : Physical Therapy in Sports : Assessing Adductor Squeeze Test and groin injuries in elite football players. During a training session, They conducted research on the relation between groin injury and hip adductor strength in professional football teams. 71 players volunteered to participate in the research. A pre-session squeezing test was performed on n=18 players who had groin injuries and n=53 players who were not injured. As a result, players with groin injuries have significantly reduced adductor strength. They come to the conclusion that the squeeze test is a reliable method of assessing groin pain in football players.
6) Famonn Delahant, Helen Fitzpatrick, et.al. (2017) :
Physical Therapy in Sports, Conduct study on Pre-season adductor squeeze test & HAGO’s function. He takes 55 male elite football players (age 24 ± 2.8 years) from a single senior football team and 137 of them representing groin pain. He concludes that the Pre-season adductor squeeze test & HAGO’s function are useful to identifying the risk of developing groin injuries.
7) Kristian Thorborg, Per Holmich, et.al. (May 2011) :
British Journal of Sports Medicine, Conduct study on validation and development of HAGOS according to COSMIN checklist on 101 physically active patients range 18-63 years. Statistical significant correlation coefficients (0.37, 0.73 P < 0.01) for validity & responsiveness. He concludes that HAGOS
has adequate measurement qualities (6 factors) in young to middle age patients with hip & groin pain.
8) Kristian Thorborg, Thomas Bandholm, et.at. (July 2013) : knee Surgery Sports Traumatology Arthroscopy, Assessing hip and knee strength using HHD and Said that HHD is a reliable way to measure hip strength. He conducts a study on 21 healthy athletes (6 women), 30 (8.6) [mean (SD)] years of age and performed all the hip strength measurements carefully and conclude that this procedure is perfectly suited for evaluation and monitoring of athlete with hip & groin injuries.
9) Abbas Yousefzadeh, Azadeh Shadmehs, et.al. (June 2018) : BMJ-Open Sport & Exercise Medicine : Assessing Holmich exercise on ARGP in athletes. The Holmich Protocol Exercise was replicated before and after the clinical trial to assess the effects of ARGP. They critically assessed its impact on 17 male athletes suffering from ARGP who had undergone a 10- week treatment cycle. They found that the visual equivalent pain scale, hip adductors and abductors muscle power, and functional score all improved dramatically, suggesting that this protocol may be a good therapy for ARGP.
10) Jour Harpy, Benjamin Assen, :june 2017
British Journal of Sports Medicine : The occurrence of groin problems in male football players was investigated using the Copenhagen Adductor Exercise Protocol. They consist of 35 football teams that were cluster-randomized into an intervention group (18 teams, 339 players) and a control group (18 teams, 339 players) (17 teams, 313 players). The intervention group did an adductor strengthening program three times a week during pre-season and once a week during the regular season, using one exercise of three progression levels. During the season, 13.5 percent of the intervention group had groin problems, while 21.3 percent of the control group did. As a result, they came to the conclusion that the Adductor Strengthening Program reduced the self-reported prevalence and risk of groin problems in male football players significantly.
11) Jour Harpy, Kristian Thorborg, et.al. (2017).
American Journal of Sports Medicine : A study was conducted to see whether the Copenhagen adductor exercise could be used in FIFA 11+ for football players. They chose 45 eligible players and divided them into two groups at random. The first group did the regular FIFA 11+ exercise program, while the second did Nordic hamstring exercises with adductor strengthening in Copenhagen. They found that those who performed the Copenhagen adductor exercise in the FIFA 11+ program had a substantial improvement in eccentric hip adductor strength (0.29 Nm/Kg)
MATERIALS AND METHODS
Method of Collection of Data :
- Study Design: Experimental study
- Sample Size: 32 players at Football court
- Sample Design: Convenient sampling
- Duration of Study: 5 weeks
Material/Tools Used in Study :
- Pencil
- Paper
- Writing Pad
- Plinth
- Pillow
- Soccer Ball
- Hand Held Dynamometer
- HAGO’s Questionnaire

Figure 1 PEN, PENCIL, PAPER & WRITING PAD
Figure 2 SOCCER BALL

Figure 3 HHD (SAEHAN)
CRITERIA :
INCLUSION CRITERIA:
Male football players [age 18-30 year]
![]() Groin pain during and after football
Groin pain during and after football
![]() Groin pain more than 4 weeks.
Groin pain more than 4 weeks.
![]() Not able to fully participate in football due to groin pain.
Not able to fully participate in football due to groin pain. ![]() Pain at palpation of the groin .
Pain at palpation of the groin .
![]() Squeeze test positive
Squeeze test positive
EXCLUSION CRITERIA:
![]() Recent Injuries
Recent Injuries
![]() Infection (UTI)
Infection (UTI)
![]() Malignancy
Malignancy
![]() Spinal Pathology
Spinal Pathology
Inguinal Pain (Hernia)
Lower Back Pain
Player on NSAIDs
METHODOLOGY :
The study was undertaken at ARA FC Sindhu Bhavan road, Ahmedabad. Participants were involved in the study with their consent based on inclusion and exclusion criteria. A squeeze test was used to evaluate adductor-related groin pain. It was performed on 47 players out of 150 players in that 39 players had adductor-related
groin pain out of which 7 were excluded according to criteria.
A total 32 participants took part into the protocol.
As per study the participant categorized into 4 different groups.
1. HOLMICH EXERCISE PROTOCOL :
There are 6 Different types of exercises were performed by players who were a participant.
a) In a supine position with the knee completely extended and the first toe pointing straight upwards, perform isometric adduction for 30 seconds against a soccer ball positioned between the feet.
-3 sets of 10 with 15 sec recovery period.
b) 30 seconds of isometric adduction with a soccer ball between the knee and hip flexed at 45 degrees with feet flat on the ground.
-3 sets of 10 with 15 sec recovery period.
c) Sit-ups in a supine posture with the hips and knees flexed at 45 degrees and the feet flat on the floor.
-5 sets of 10 with 15 sec recovery periods.
d) The player performs a series of sit-ups while dragging the soccer ball towards the head in a supine posture with the hip and knee joints flexed at 45 degrees and a soccer ball clamped between the knees. To achieve coordination, move in a rhythmic manner.
-5 sets of 10 with 15 sec recovery periods.
e) Perform an adductor lateral slide for 1 minute using a slide board or paper with an extremely smooth surface and a low friction sock on the sliding foot. f) Forward slide for 1 minute, maintaining the same position as the lateral slide.
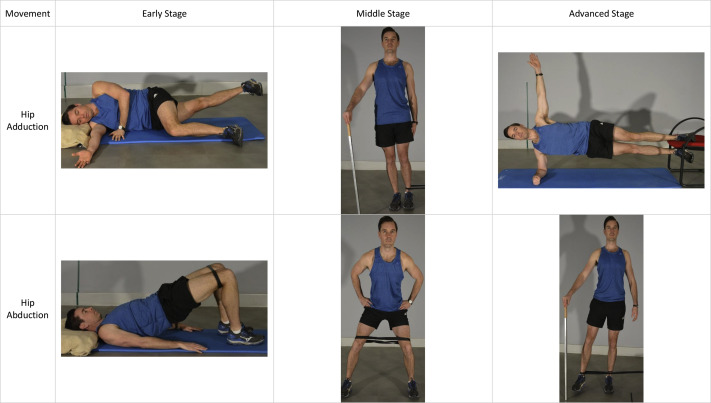
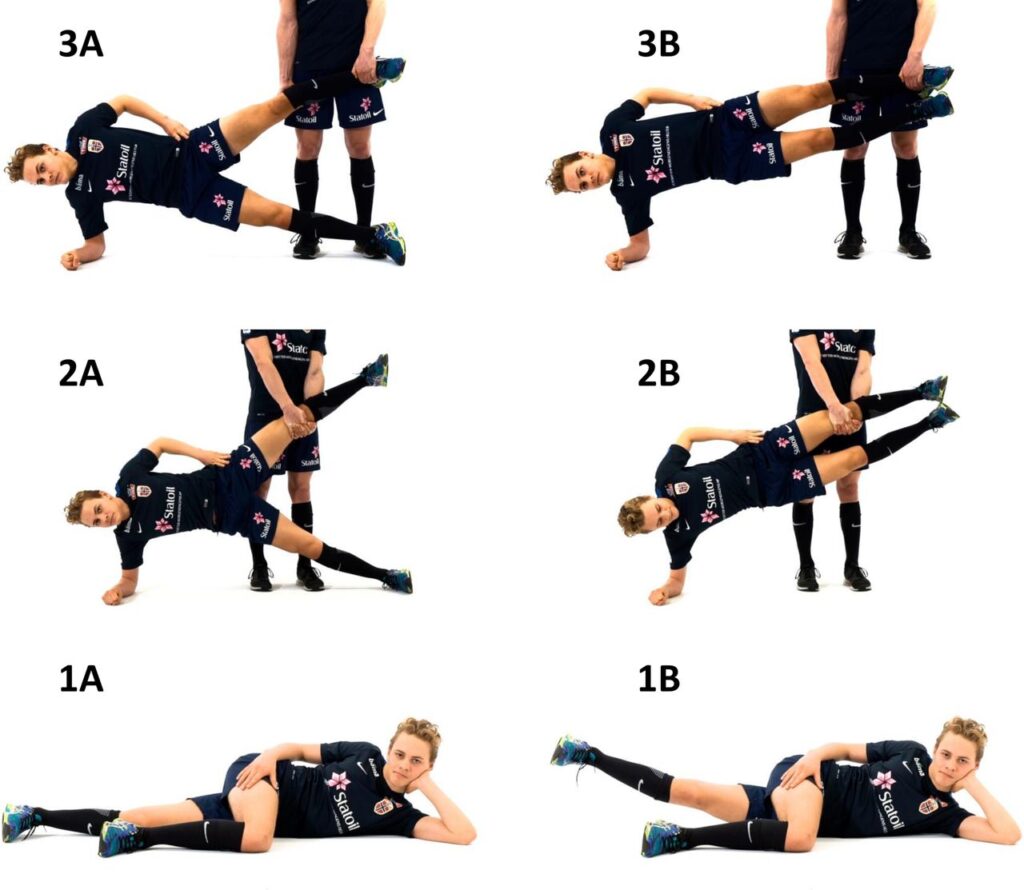
2. COPENHAGEN EXERCISE PROTOCOL :
There are 3 different levels of exercise were performed by players.
Level 1: Side-lying hip adduction exercise.
Level 2: Copenhagen adduction exercise – both arms support at the knee. Level 3: Copenhagen adduction exercise – primary support at the ankle and minor support at the knee.
The dynamometer was used to evaluate the strength of the adductor muscle before and after exercise protocol to see the improvement. The self-administered format of HIP AND GROIN OUTCOME SCORE (HAGOS) was used as a tool to evaluate longstanding hip and/or groin pain before and after the exercise protocol.
The HAGOS Questionnaire was explained thoroughly to all players by the therapist and they were made to fill the form in front of the therapist to avoid chances of errors. only the English version of the HAGOS Questionnaire was used as all the players are professionals.
STATISTICAL ANALYSIS
The data from the collection were analyzed by using statistical package for social science (SPSS) version 20 and Test of Normality was done and found that the data were not normally distributed. So that the non-parametric test was used in data analysis. The Mann Whitney U test was used to compare demographic values between the groups. The threshold for statistical significance was set at p<0.05.
RESULT
The purpose of this comparison analysis was to see how successful the Copenhagen and Holmich exercise protocols were on ARGP male football players. There were a total of 32 subjects in this study, with 16 subjects in each group meeting the inclusion criteria.
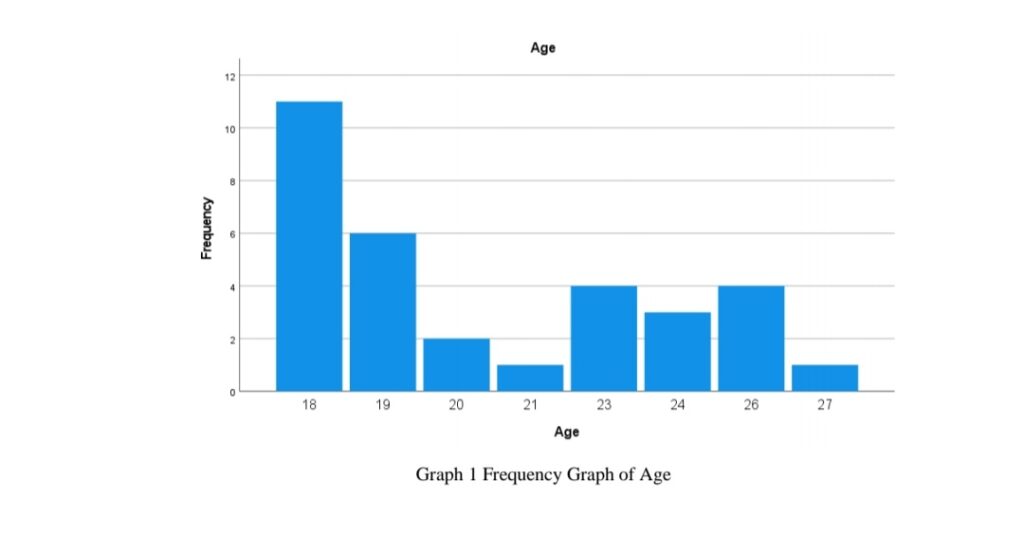
The age group of the male football players was 18-30 years and mean age of players was 20.88±3.13 as show in Table 1.
Table 1 Mean Age and Standard Deviation
| AGE MEAN SD | ||
| 18-30 | 20.88 | ±3.13 |
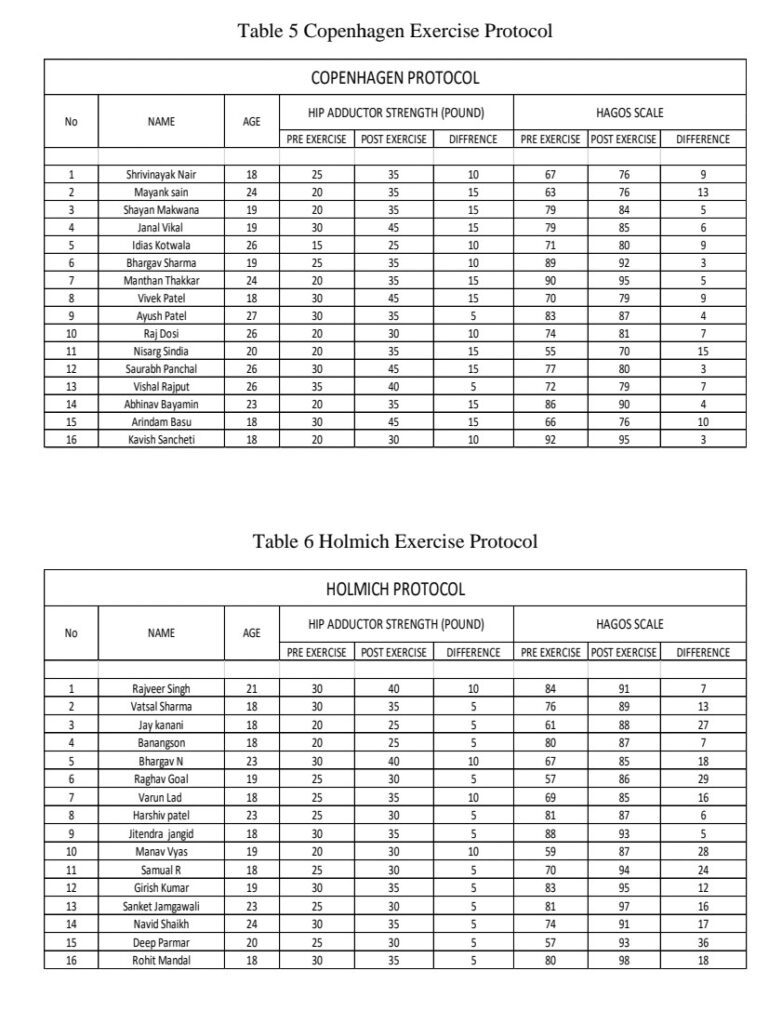
THE COPENHAGEN EXERCISE PROGRAM:
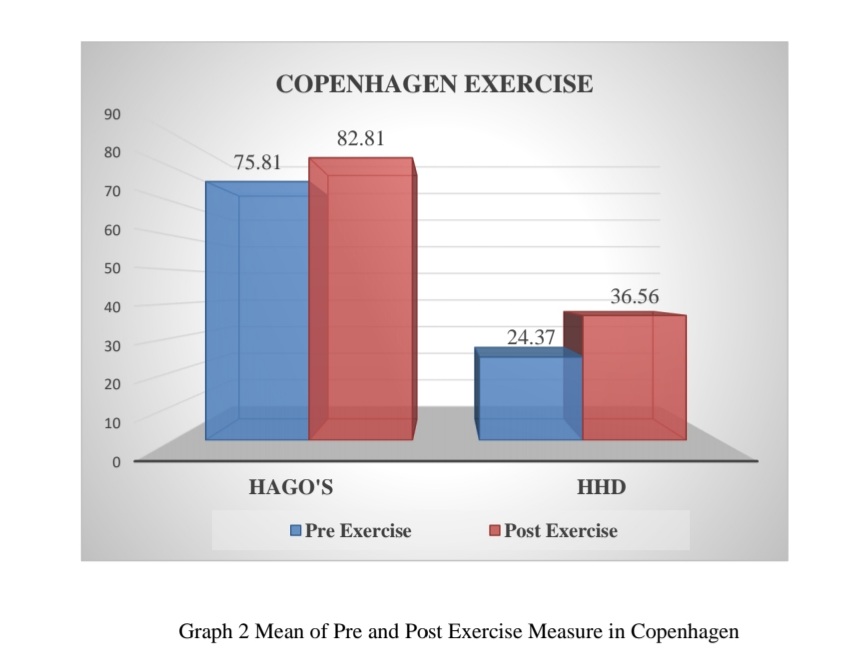
Table 2 and Graph 2 show mean values of pre and post-exercise measures of the Copenhagen exercise program. It also shows the improvement in HAGOS and Hip Strength (HHD) after the exercise program.
Table 2 Mean and SD of Pre and Post Exercise Measure in Copenhagen
| EVALUATION TOOL PREMEAN ± SD POSTMEAN ± SD | ||
| HAGOS | 75.81±10.52 | 82.81±7.34 |
| HHD | 24.37±5.74 | 36.56±5.98 |
THE HOLMICH EXERCISE PROGRAM :
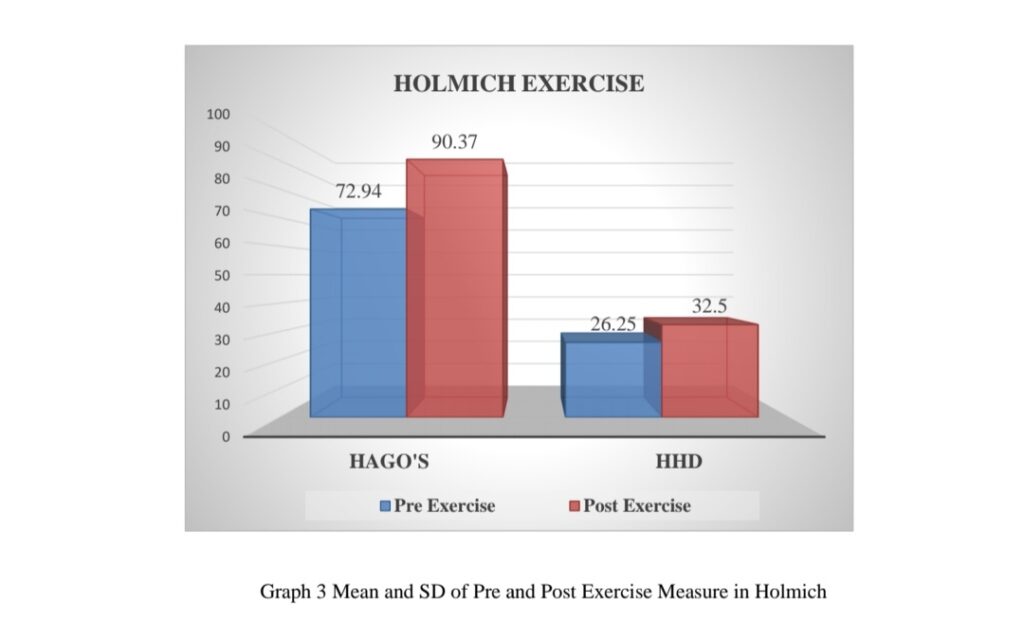
Table 3 and Graph 3 show mean values of pre and post-exercise measures of the Holmich exercise program. It also shows the improvement in HAGOS and Hip Strength (HHD) after the exercise program.
Table 3 Mean and SD of Pre and Post Exercise Measure in Holmich exercise
MANN-WHITNEY U TEST :
Table 4 shows the U value and Significant difference value between Copenhagen and Holmich exercise program. (Level of Significant Set<0.05)
Table 4 Statistical analysis by U Test
| No. U TEST U -VALUE P-VALUE | |||
| 1 | HAGOS | 50.5 | 0.03 |
| 2 | HHD | 78.0 | 0.04 |
The data are not normally distributed so in this study Non-parametric Mann Whitney U Test applied to assess the difference between Copenhagen and Holmic exercise protocol for adductor-related groin pain in football players. There is significant improvement of hip dynamometry and HAGOS questionnaire in both the exercise protocol but when compared Copenhagen exercise protocol shows more improvement in hip strength in compare to Holmich exercise protocol whereas hip function is greatly increased in Holmich exercise protocol.
DISCUSSION
The study is about “Comparison of Copenhagen V/s Holmich exercise protocol on acute ARGP in male football players”. Both the exercise protocols are effective individually but there is no evidence that the initial results of the Copenhagen and Holmich exercise protocols are comparable.
A total of 32 participants were randomly divided into two groups. The mean age of the subject was 20.88±3.13. 2 weeks of exercise sessions were given to see the progression. To evaluation of both exercise programs, pre and post dynamometry (HHD) and HAGOS were used.
In HAGOS, a Score is between 0-100 in that 0 is poor and 100 is good hip and groin outcome parameters.
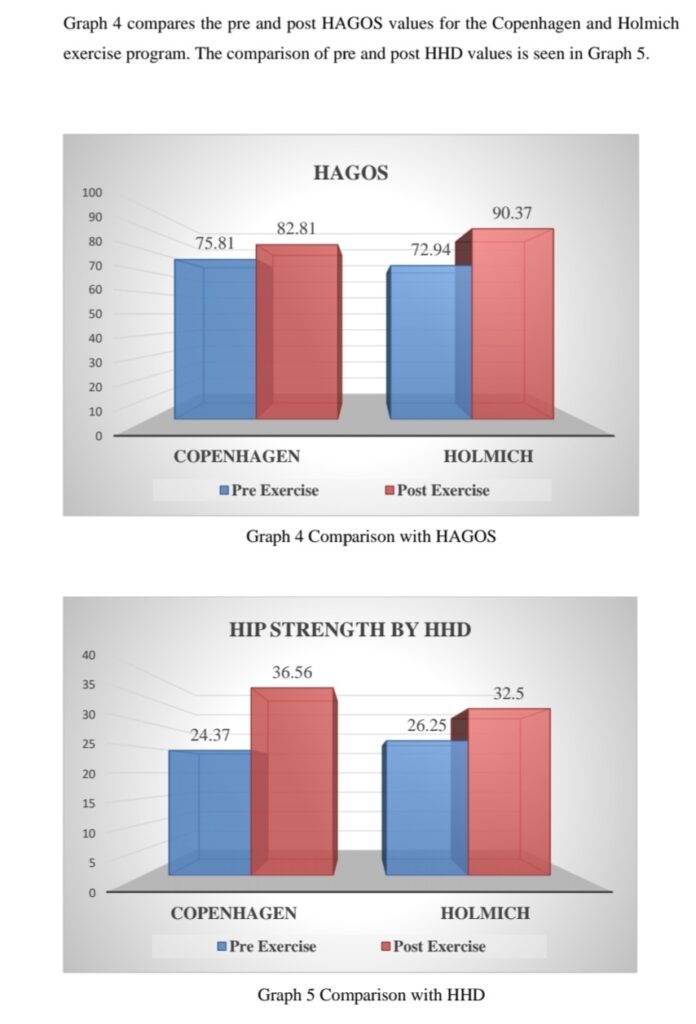
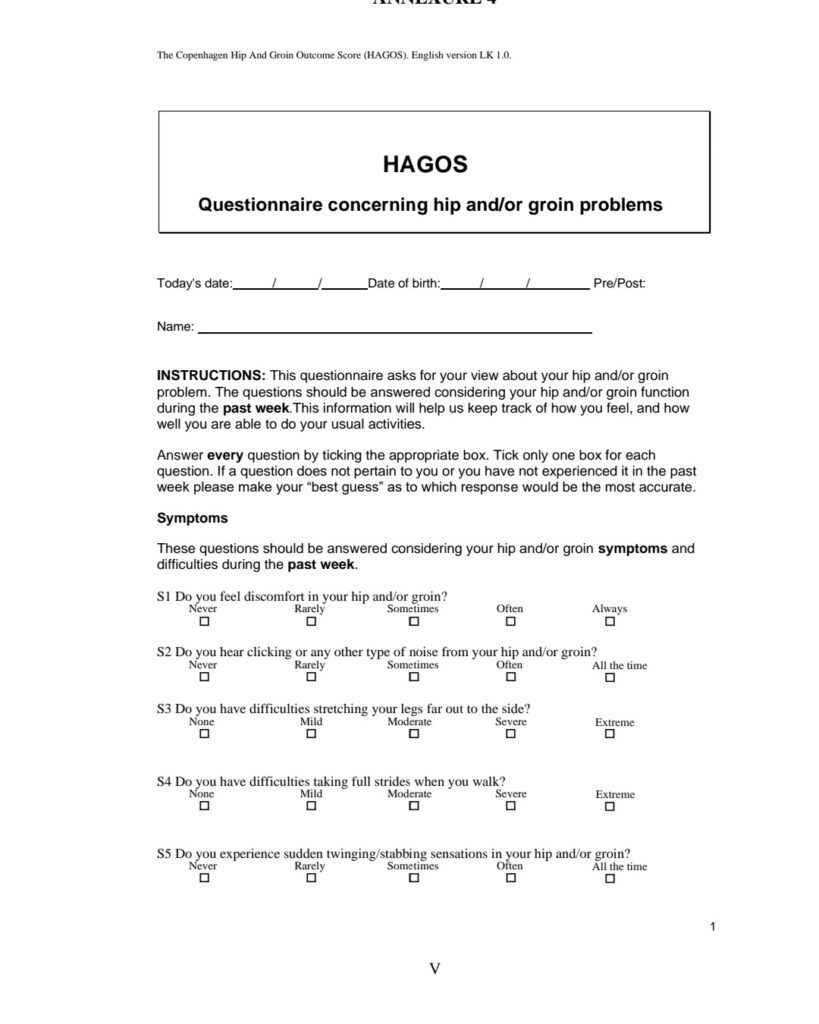
Pre-HAGOS Score for the Copenhagen exercise protocol was 75.81±10.52 and it is 82.81±7.34 after the exercise program. Pre-HHD for the Copenhagen exercise program was 27.37±5.74 and it is 36.56±5.98 after the exercise.
Pre-HAGOS Score for the Holmich exercise protocol was 72.94±10.31 and it is 90.37±4.24 after the exercise program. Pre-HHD for the Holmich exercise program was 26.25±3.87 and it is 32.50±4.47 after the exercise.
In this study, the non-parametric Mann-Whitney U test was used to analyze the difference between two exercise protocols.
In the Mann-Whitney U test, the HAGOS for the Copenhagen exercise protocol is 11.66 and for the Holmich it is 21.34. U value for HAGOS is 50.5 and the significant value is 0.03. that suggests that there is significant improvement in HAGOS in Holmich exercise protocol compare to Copenhagen exercise protocol.
Abbas Yousef Zadeh, Azadeh Shadmehs, et. al. (2018). The Holmich exercise protocol includes strengthening of pelvic and adductor muscle, hip adductor stretching, high intensity strengthening exercise for hip adductors and core stabilization exercises that will help in reduce pain, increase hip adductor muscle strength and improve function of hip muscles.17
In the Mann-Whitney U test, the HHD for the Copenhagen exercise protocol is 19.63 and for the Holmich it is 13.38. U value for HHD is 78 and the significant value is 0.04. that suggests that the Copenhagen exercise is best for improvement in hip strength, and the Holmich exercise is less effective for improvement in hip strength in Compare to the Copenhagen exercise protocol.
Hip adductor muscles are located in the inner thigh and it helps in balance, alignments of body, and move the leg towards the midline of the body.
In soccer, there is repeated movement like turning and kicking so that there are higher chances of groin injuries. For improving athletic performance and preventing injuries it is necessary to strengthen the adductor muscles.
When eccentric hip adduction strength is low there are higher chances of adductor related groin injuries. The Copenhagen adductor exercises include high muscle activity with eccentric muscle contraction that will help to improve in eccentric strength of adductor longus muscle which is highly affected during groin injuries.
Jour Haroy, Benjamin clarsen, et.al (2019) conducted study on adductor strengthening protocol for groin pain. They evaluate the adductor strengthening using Copenhagen exercise protocol on 36 semi-professional team and conclude that strengthening of adductor muscle using Copenhagen adductor exercise will reduce the risk of groin injuries.16
Jour Haroy, Kristian Thorborg, et. al. (2017) found that including Copenhagen adductor exercise in FIFA 11+, help to increase eccentric strength of adductors.
This study shows performing Copenhagen exercise, there is significant improvement seen in strength of hip adductors compare to Holmich exercise, and while performing Holmich exercise, there is significant improvement seen in hip and groin outcome score, compare to Copenhagen exercise.
CONCLUSION
• There is a significant improvement in players with adductor-related groin pain by using the Copenhagen exercise protocol and the Holmich exercise protocol, both exercise protocols have marked efficacy on individual parameters suggest that longer exercise regimen may give more precise results.
SUMMARY
• This study compares the initial effect of Holmich v/s Copenhagen exercise protocol in adductor-related groin pain in male football players. The study was conducted at ARA FC, Ahmadabad. 32 players were randomly divided into 2 groups. Group 1 was the Holmich exercise program and group 2 was the Copenhagen exercise program. Both groups were evaluated before and after the exercise program by using HHD and HAGOS. Both exercises are effective in adductor-related groin pain. In the Copenhagen exercise, there is significant increase in strength and in the Holmich exercises, there is significant
improvement seen in HAGOS.
LIMITATION & FURTHER RECOMMENDATION
➢ LIMITATIONS :
• This study has taken a smaller sample size but it can be also done with large sample size.
• The present study only saw the immediate effects of protocols. • This study only measures the strength of hip adductors on one side in which player have more pain.
➢ FURTHER RECOMMENDATION :
• There is only 2 weeks of protocol used in this study, for further study 8 weeks long protocol can be use in order to achieve more precise results. • Bilateral lower limb muscle strength can be compared. Also the pain variable can be included.
• The Copenhagen and Holmich Exercise Protocols are useful to prevent ARGP.
REFERENCE
1. Junge A, Dvorak J. Soccer injuries: a review on incidence and prevention. Sports Med. 2004;34(13):929–38.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3063461/
2. UPMC sports medicine
https://www.upmc.com/services/sports-medicine/for
athletes/football#:~:text=Recreational%20football%20players%20can%20spra in,Ankle%20sprains
3. Michael Lau, PT, DPT, Elizabeth Quinn. November 28 , 2019
https://www.verywellfit.com/common-football-injuries-3120330
4. Morelli M. Groin injuries in athletes. Am Fam Physician. 200
http://www.aafp.org/afp/2001/1015/p1405
5. Per Holmich, Br J Sports Med. 2007 Apr; 41(4): 247–252.
Published online 2007 Jan 26. doi: 10.1136/bjsm.2006.033373
6. Holmich, M.D., Sports Medicine and Arthroscopy Review: October 1997 – Volume 5 – Issue 4 – p 285-291
7. Bruckner & Khan’s clinical sports medicine. Volume 1 (injuries) 5th edition. McGraw Hill Education (India) Private Limited (2018). P 629-651
8. Nicholas Macintyre, Jim Johnson, Chris DO; Schroeder, Erik L. Current Sports Medicine Reports: December 2006 – Volume 5 – Issue 6 – p 293-299
9. McKee, J. What’s causing a patient’s groin pain? Hip disorders and other coexisting, non orthopedic conditions may be at play. AAOS Now, October 2013. http://www.aaos.org/news/aaosnow/oct13/clinical10.asp
Accessed December 15, 2014
10. NATA Journals: Eamonn Delahunt, Barry L. McEntee, et. al. J Athl Train. 2011 May-Jun; 46(3): 241–245.
11. NATA Journals: Jaqueline Martins, PT, Janaina Rodrigues da Silva, et al. J Athl Train. 2017 Sep; 52(9): 809–819.
12. Lasse Ishoi, Per Holmich, et.al. International journal of sport physical therapy. 2019 Sep; 14(5): 715–723
13. Kristian Thorborg, Per Holmich et. sl. (May 2011) British Journal of Sports Medicine: 45(6):478-91
14. Thorborg K, Holmich P, Christensen R, Petersen J, Roos EM. The Copenhagen Hip and Groin Outcome Score (HAGOS): development and validation according to the COSMIN checklist. British Journal of Sports Medicine. 2011; 45(6):478-491. doi:10.1136/bjsm.2010.080937
15. Holmich P., Uhrskru, et.al.(1999) the lancet 353(9151),439-443. 16. Lasse Ishoi, Kristian Thorborg, British Journal of Sports Medicine, 2021
17. Azadeh Shadmehr, Abbas Yousefzadeh, (March 2018) Rehabilitation Research and practice 2018(2):1-10.
18. Jour Haroy1, Kristian Thorborg, the American journal of sports medicine 45(13), 3052-3059, 2017
ANNEXURE 1
CONSENT FORM
DATE :_________________
STUDY TITLE :A COMPARATIVE STUDY OF HOLMICH V/S COPENHAGEN EXERCISE PROTOCOL IN ADDUCTOR-RELATED GROIN PAIN IN MALE FOOTBALL PLAYERS.
SUBJECT’S NAME : _____________________________
AGE : ____________
I have been explained about the research project entitled “A Comparative Study of Holmich v/s Copenhagen Exercise Protocol in Adductor-Related Groin Pain in Male Football Players”.
I understand that my participation in the study is voluntary and that I will be free to withdraw at any time without giving any reason.
I understand that the data obtained through the study may be used for research paper publication and I also understand that my identity will not be revealed in any information released to publish.
I agree to take part in the above study.
Sign of Subject : Sign of Investigator :
ANNEXURE 2
DEMOGRAFIC DATA OF PARTICIPANT
• Name :- ______________________________ • Age :- _________
• Height :-_________
• Weight :-_________
• Any medical history :- ___________________ • Contact Number :- ____________________
ANNEXURE 3
MASTER CHART