
Effect of Positional Release Therapy and myofascial trigger point treatment on pain, range of motion and flexibility in the Hamstring muscle
Table of Contents
ABSTRACT:
Objective: To compare the effect of positional release therapy and myofascial point treatment on pain, range of motion and flexibility in patients with hamstring trigger point pain.
Design: Experimental/comparative study
A hyperirritable point or spot, usually within a taut band of skeletal muscle or in the muscle fascia, that causes referred pain and motor dysfunction when compressed is known as a myofascial trigger point (MTrP). According to research, MTrPs can be treated with a range of massage techniques Positional release technique and myofascial trigger therapy used for hamstring trigger point treatment
Method: 30 subjects with calf trigger points pain were selected. They were divided into 2 groups. Group A (n=15) participants were given positional release therapy. Group B (n=15) participants were given myofascial therapy. Outcomes measures score of NPRs, ROM of the knee, Passive Knee Extension Test (PKET) were taken before and after the treatment.
Result: The results were obtained using paired and unpaired t-test via SPSS. Both treatments were shown to be effective in reducing pain (NPRS-p value-0.00), improving flexibility (p value-0.00), and increasing range of motion(p value-0.00).
Conclusion: positional Release Therapy and myofacial trigger point Therapy were found to be equally effective in trigger point pain in this study.
Keywords: hamstring trigger points, positional release therapy, myofascial trigger point therapy
ABBREVATIONS
PRT: POSITIONAL RELEASE THERAPY
MTrp: MYOFACIAL TRIGGER POINT PAIN
ROM: RANGE OF MOTION
ADLs: ACTIVES OF DAILY LIVING
INTRODUCTION:
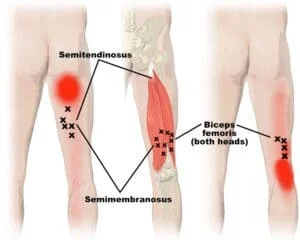
The superficial muscles that run along the back of the leg are known as the Hamstring muscles.

- Biceps femoris.
- semi membranous
- Semitendinosus.
This muscle are mainly use for running, stairs climbing ,walking ,squats etc
These trigger points are characterized as follows:
- Active trigger points: In active trigger points the player usually complains of
pain without any symptoms of weakness, parenthesia or temperature change.
The might complain of referred pain. - Latent trigger points: In latent trigger points, the player comes with the complaint of pain while applying external pressure. This is sometimes associated with muscle shortening. This trigger points might get activated when there is poor posture, overuse of muscle or muscle imbalance
A myofascial trigger point (MTrP) is termed as a hyperirritable spot that is located within a taut band of a skeletal muscle that hurts when you compress or stretch it, resulting in a typically referred pain pattern, as well as an automatic phenomenon. Abnormal stress on the muscle from sudden stress on the shortened muscle, leg length discrepancy, or skeletal asymmetry is the common cause of myofascial pain. Moreover, poor posture & assumption of a static position for a long period are also a cause of it. Acute trauma or repeated microtrauma, according to many studies, may contribute to the formation of a trigger point. Lack of exercise, prolonged poor posture, vitamin deficiencies, sleep disturbances, and joint disorders may all cause micro-trauma. Occupational or recreational behaviors that impose repetitive stress on a single muscle or muscle group, resulting in trigger points, are the most common causes of chronic stress in muscle fibers. Acute trauma or repeated microtrauma may cause muscle fiber stress and the formation of trigger points
Flexibility: in this, flexible joints can move freely in a range of motion without any pain and being limited.
Flexibility can be divided into two categories:
1) Dynamic flexibility or active mobility: This refers to how far an active muscle movement can pass a body segment across the joint’s range of motion.
2) Passive versatility or passive mobility refers to the extent to which a body segment can be rotated across the full range of motion without actively moving it. It is determined by the muscle’s extensibility One of the important physiological components of physical fitness is flexibility. the muscle extensibility might get affected very commonly in various individuals who are perfectly healthy. The safety and optimal physical activity depend on the ability of an individual to move smoothly. as flexibility is an important physiological component of physical fitness and reduction in flexibility may lead to inefficiency at the workplace and may also become a risk factor for hamstring Pain. whereas, the tightness of the muscle and balance of the individual is correlated to each other. The muscle inflexibility leads to the presence of exquisite tenderness at the nodule in a taut band of muscle which is palpable. hamstring muscle frequently hypertrophies by running due to the propulsive gait performed in running by the hamstring muscle complex. This may lead to the inflexibility in the hamstring muscle
Nocturnal night cramps are a symptom of active remembrances of MTrP, whereas
Nocturnal night cramps are a symptom of active semitendinosus MTrP. There has been a report of referred heel pain and restricted knee extension ROM. It can also cause increased stress concentration as well as hip, knee, and lower back pain.
Spray and Stretch, ultrasonography, coercive therapy, and injection are all used to inactivate TrPs. positional release therapy myofascial trigger therapy dry needling, intense transverse pressure massage, and other treatments for the release of trigger points have all been shown to be successful in studies. The other physiotherapy techniques are also used to release this trigger. In these studies, positional release therapy(PRT) and ischemic compression therapy(ICT) techniques are used to relieve the hamstring points The PRT technique’s basic concept is to assess the (ideal) location of optimal articulation comfort while decreasing the sensitivity of the pain point.
This procedure involves put sg the affected tissue in a comfortable position, which in this case was determined using surface electromyography. PRT involves positioning the patient so that the origin and insertion points of hypertonic muscle are as close together as possible. Pressure on a comfortable position(90 seconds for orthopedic patients and 3 minutes for neurological patients) causes a therapeutically important physiological response in the tissue, resulting in relief from pain, increased mobility, and the resolution of dysfunction. The muscle spindle activation is occupied as a result, and the efferent impulse is reduced. These efferent impulses were usually sent to the muscle to protect it from excessive stress. As a result, this course is broken by allowing the muscle to relax and return to its usual resting tone. After 90 seconds, the patient is brought to a neutral position slowly and passively without firing the muscle spindle.
This brings the PRT process to a close. PRT was improved posture and ADLs by reducing muscle tension in the hamstring and musculoskeletal pain. In art, the term “trigger point pressure release” was coined, and it was described as follows: “Slowly growing, non-painful pressure application” over a trigger point before a tissue resistance barrier is reached stumbled upon After that, contact is retained until the tissue is removed. The barrier is broken down, and pressure is raised to achieve a new level. To remove trigger point stress and tenderness, create a barrier. MRT can reduced the Hamstring muscle pain, improve the ROM and ADLs. PRT and MRT therapy are important protocols for treating HAMSTRING trigger point pain. There are several studies that show that PRT and MRT therapy are both successful techniques. No research has been done to compare the two methods. As a result, the aim of this study is to determine and compare the efficacy of PRT and MRT
NEED OF STUDY
Hamstring trigger point pain is managed using a variety of treatment protocols such as passive stretching, foam roller stretching, massage, strengthening exercise, taping technique, spray and all. Several studies and researches have been conducted to assess the pain relief, expanded range of motion, and flexibility of hamstring trigger point pain. These study is conducted for collate the effectiveness of positional release therapy and myofascial trigger point therapy on hamstring trigger point pain, range of motion, and flexibility in patients with hamstring trigger points. There is no research that collate positional release therapy and myofascial trigger point , according to a previous report. The purpose of this study is to determine which exercise is more effective as a treatment for patients with hamstring trigger points.
Aims and objectives
Aims:
The aim is to find out the effectiveness of positional Release Therapy versus Myofascial trigger point therapy on hamstring triggers pain, ROM, and flexibility in a patient with hamstring muscle trigger point.
Objective:
- To find out the effect of PRT on pain, ROM and flexibility in patients with hamstring
trigger point. - To find out the effect of MTRon pain, ROM and flexibility in patients with Hamstring
trigger point. - To compare the effect of a PRT and MTR on trigger pain, ROM and flexibility
in patients with hamstring Trp.
Hypothesis:
- Null hypothesis:
There is no significant difference between positional release therapy and myofascial trigger point therapy on pain, ROM and flexibility in hamstring muscle trigger point Pain. - Alternate hypothesis:
There is a significant difference between positional release therapy and myofascial trigger point therapy on pain, ROM and flexibility in hamstring muscle trigger point Pain.
Review of literature:
- Rehabilitation of Proximal Hamstring tedinopathy Utilizing Eccentric Training, Lumbo pelvic Stabilization, and Trigger Point Dry Needling: 2 Case Reports AUTHORSD
- The Effectiveness of Myofascial Release Techniques in the Treatment of Myofascial Pain: A Literature Review By John Werenski June 17, 2011
- Himanshi ruparelia et al (2019) studied the impact of muscle energy technique and positional release therapy on SLR 90°-90 dorsi flexion was investigated. In this study 30 subjects with 18-30 years of age were selected and randomly divided into the two groups. Muscle energy technique was used in Group A while positional release therapy was used in Group B. It concluded that MET is more effective than positional Release therapy for tight muscles
- Nirali M. jain et. (2020) studied on a runner with a gastro-soleus trigger point the effective of two techniques that are PRT and ART therapy. Total 30 subjects with 20-30 Years of age participate in the study and Two groups were for me tad random. Active Release Technique was given to Group A, while Positional Release Therapy was given to Group B. As a result it is concluded that positional release therapy is more effective than the active release technique.
- Carlos Alberto Kelencz et. (2011) studied positional release therapy with electromyographic on the trapezius trigger point. Total 6 subjects with trapezius tension selected for study. It concluded that PRT can improve the life quality in patients with trapezius trigger points.
- M Doley et. (2013) studied on Gluteus Medius Trigger Points, researchers compared the effectiveness of positional Release Therapy and deep transverse friction massage. Total 30 subjects were selected for study Were randomly divided into either of the two groups. Group A Positional Release Therapy was given and Group B Deep Transverse Friction Massage was given. It concluded that the DTFM is more effective than positional Release therapy in pain threshold in subject
- Babara Cagnie et. (2013) studied the short term effectiveness of positional release therapy on neck and shoulder trigger points. Total 19 Office worker subjects with neck pain and shoulder pain selected for the study. Protocols were applied for a total 4 week and outcomes measured by NPRS, NDI, neck mobility, muscle strength. It concluded that 4 week treatment of IC had significant improvement in neck and shoulder pain, mobility and strength.
- Sahem AM AL-Shawabka et.(2013) studied On the upper trapezius muscle, researchers compared the efficacy of positional release technique versus manual pressure release. 45 patients were randomly divided into 3 groups. Group A was a control group, group B received MPR and group C received PRT. It concluded that MPR is more effective than PRT for decreasing pain and increased CROM
Material and Methodology:
Material:
- pen
- paper
- Goniometer
- plinth
- contest form
- NPRS scale sheet
- Measure tape
Collection of data:
Source of data: sports club
Sample design: convenient random sampling
Sample size: 20(10 in each group)
Study design: A comparative design
Duration of study: 3 time per session per week for 2 weeks Sundays and holiday
will be included
Inclusion Criteria:
- Age: Between 18-30 yeas old
- Male and female
- Patients who are having ankle dorsiflexion ROM less than 20 degrees.
- Pain intensity on NPRS is greater than 4 and lasts at least for 6 months.
Exclusion Criteria:
- Patients who are having congenital deformity of knee & hip
- Patients with fibro myalgia syndrome, tumors, lower limb fracture, diabetic neropathy, peripheral vascular disease & recent injury.
- Unwillingness of patients to participate in the study
- Using any other treatment other that prescribed protocols during the study
Evaluation of tools:
Outcome Measure:
- pain – NPRS
- hip joint range of motion – goniometer
- flexibility
For pain : Nprs scale
The Numeric Pain Rating Scale (NPRS) is a one-dimensional measure of severity of pain intensity. In this scale, patients selects a numbers between 0 to 10, that representing the intensity of his/her pain. The 11-point numeric scale ranges from ‘0’ representing one pain to ’10’ representing the extreme pain. The subject will be asked to mark the numeric value on the scale according to their pain intensity. These scale has 0.94 of reliability
![Fig. 3. The Numeric Pain Rating Scale. https://www.google.co.il/search?q=numeric+pain+rating+scale+(nprs) [pictures].](https://www.e-jer.org/upload/thumbnails/jer-11-2-67f3.gif)
PASSIVE KNEE EXTENSION TEST(PKET):
PURPOSE
To measure joint flexibility and end feel of joint and measure tightness of hamstring muscle
This test also use for to monitor patient of ACL injury and hamstring injury for recovery purpose
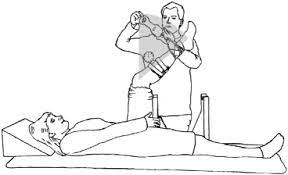
TECHNIQUE
The patient is positioned lying on plinth with the hip of the tested leg in 90 degrees of flexion. The opposite leg hold on the examination plinth. The clinician extends the knee until reaching the maximal tolerable stretch of the hamstring muscle as indicated by the patient with the opposite hip remaining in 90 of flexion. The last 3 trials should be done for each limb was included for statistical analysis. As a result, smaller than 9-10
cm is considered a restricted, shortened hamstring muscle. The distance measured for the weight bearing lunge test had an inter-rater reliability of
R=0.99. The measurement’s inter-rater reliability was also excellent in hamstring injury patient
goniometer Placement
- axis : lateral epicondyle of femur
- moving arm: lateral malleolus
- stationary :towards the greater trochanter
Procedure
A total of 30 subjects were selected according to the criteria of inclusion and exclusion. The consent form and information form were taken after explaining the treatment. The study’s objectives, the need for the analysis, and the procedure were all properly explained to the participants. Two groups of participants were created:
- Group A – Positional release therapy(prt)
- Group B: myofacial trigger point therapy
Group A – Positional release therapy(prt)

Once trigger point gets located, therapist apply i compression. He should apply it with his thumb over trigger point the patient was feel pain. Which gets referred around knee or ankle joint therapist should communicate with patient to check weather patient can tolerate pain or not. Hold this position for at least 20 sec to 60sec. ask patient weather the pain intensity gets decreased or not. Under pressure and after that gradually release the pressure. After locating all trigger points and treating them apply few efflurage stroke to flush out the area and then apply passive stretch to muscle this should be done for 4 times/ session for 2weeks.
Subject should be placed in prone lying position hip and knee should be in neutral position.Therapist should palpate the trigger point in hamstring muscle. After palpating trigger point, deep manual pressure over it should be applied by therapist and maintain for 90 sec. It should be perform 3 times/day &3 session/week for 2 weeks After 2weeks outcome measured by range of motion hip flexion using goniometer & flexibility of hamstring muscle using measure
GROUP B: myofacial trigger point therapy

Subject should be placed in prone lying position hip and knee should be in neutral position.Therapist should palpate the trigger point in hamstring muscle. After palpating trigger point, deep manual pressure over it should be applied by therapist and maintain for 90 sec. It should be perform 3 times/day &3 session/week for 2 weeks After 2weeks outcome measured by range of motion hip flexion using goniometer & flexibility of hamstring muscle using measure
Statistical analysis:
The Statistical package for Social Science (SPSS) was used to conduct the statistical research. It is found that the data was normally distributed. To compare the data within and between groups A and B, the unpaired and paired ‘t’ tests were used. The result was concluded from the sample test of the post values of the outcome measures of the both groups
Result
A comparative study for the positional release therapy and myofascial trigger point therapy was which consisted of 20 subjects, divided into two categories randomly. Positional release therapy was offered to Group A, which consisted of 10 people. Positional therapy was provided to Group B, which consisted of 10subjects. Paired and Unpaired ‘t’ test was used to find significant changes in pre and post treatment score, as well as, compare the groups for effectiveness. The mean, standard deviation, and t value were used to report the data. Minimum and maximum values of variable were analyzed by statistical for social science (SPSS)
| Groups | MEAN | SD |
| GROUP A | 20.56 | 1.89 |
| GROUP B | 24.54 | 2.44 |
TABLE 2: BASELINE COMPARISON OF PRE – INTERVENTION OUTCOMES OF BOTH THE GROUPS
| OUTCOME | GROUP A | GROUP B | T VALUE | P VALUE |
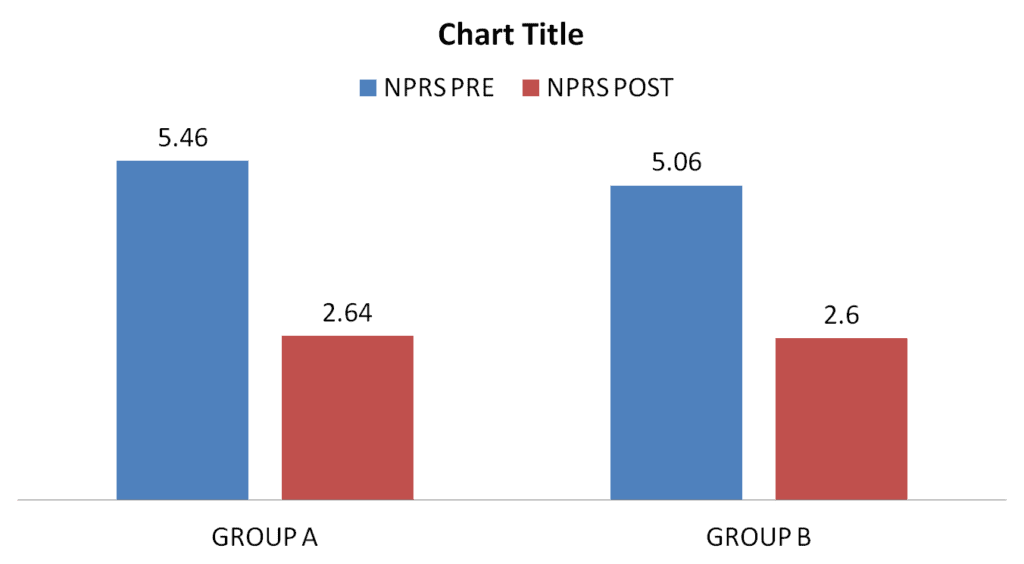
| NPRS | 5.46±1.12 | 5.06±0.70 | 1.00 | 0.33 |
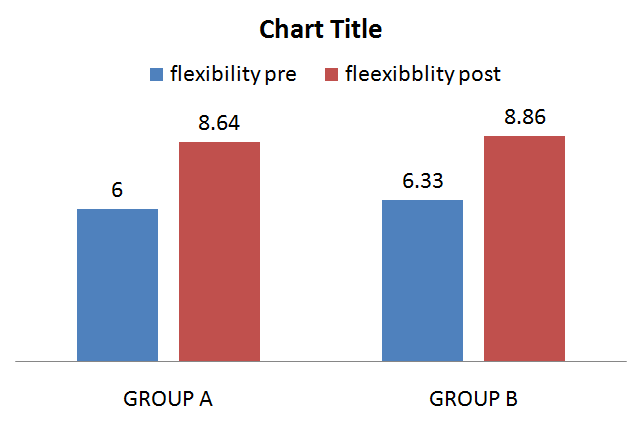
| FLEXIBLITY | 6.00±0.75 | 6.33±0.15 | 1.32 | 0.20 |
| ROM | 15.9±1.09 | 15.46±1.06 | 1.13 | 0.27 |
TABLE 2: COMPARISON OF OUTCOMES WITHIN GROUP ANALYSIS
| OUTCOME | MEAN | SD | T VALUE | P VALUE | |
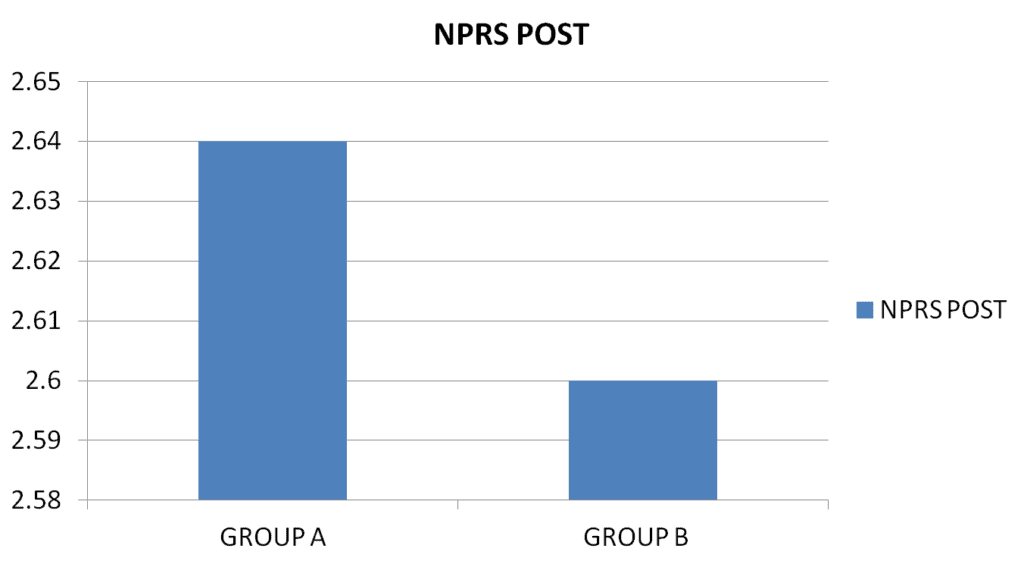
| NPRS | PRE | 5.46 | 1.12 | 18.5 | 00 |
| POST | 2.64 | 0.99 | 00 | 00 | |
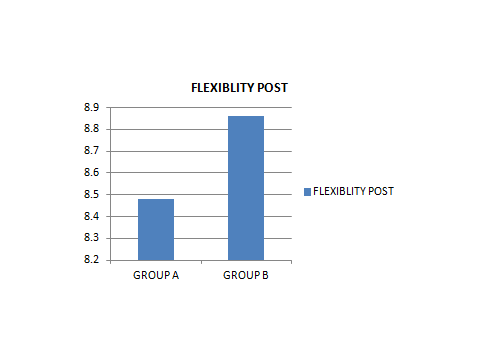
| FLEXIBILITY | PRE | 6.00 | 0.75 | 17.8 | 00 |
| POST | 8.48 | 0.60 | 33 | 00 | |
| ROM | PRE | 15.9 | 1.09 | 12.5 | 00 |
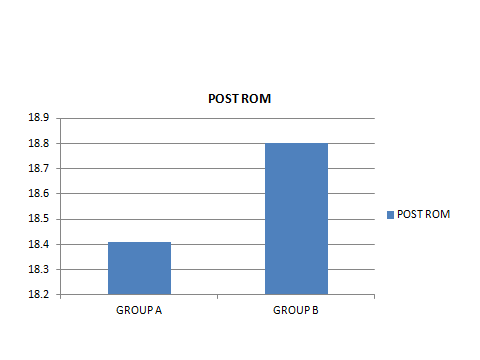
| POST | 18.41 | 0.95 | 50 | 00 |
| OUTCOMES | MEAN | SD | T VALUE | P VALUE | |
| NPRS | PRE | 5.06 | 0.70 | 14.9 | 00 |
| POST | 2.60 | 0.98 | 29 | 00 | |
| FLEXIBILITY | PRE | 6.33 | 0.15 | 19 | 00 |
| POST | 8.86 | 0.19 | 00 | 00 | |
| ROM | PRE | 15.46 | 1.06 | 17.3 | 00 |
| POST | 18.80 | 0.94 | 49 | 00 |
Graph 1.1:Comparison of NPRS within the group analysis Graph 1.3: Comparison of Flexibility within group analysis
Graph 1.2: Comparison of ROM within group analysis
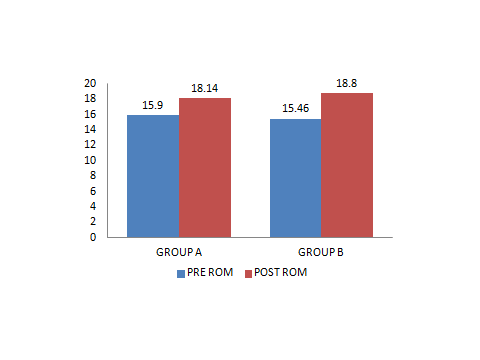
TABLE 2: BETWEEN GROUP COMPARISON OF OUTCOMES IN GROUP A
| OUTCOMES | MEAN | SD | T VALUE | P VALUE | |
| NPRS | POST | 2.64 | 0.99 | 1.10 | 0.57 |
| FLEXIBILITY | POST | 8.48 | 0.60 | 0.53 | 0.62 |
| ROM | POST | 18.41 | 0.95 | 0.98 | 0.33 |
It was proposed that there was a non-statistically important discrepancy between Group comparisons of results for improvement in post Intervention outcome
TABLE 2: BETWEEN GROUP COMPARISON OF OUTCOMES IN GROUP B
| OUTCOMES | MEAN | SD | T VALUE | P VALUE | |
| NPRS | POST | 2.60 | 0.98 | 1.10 | 0.57 |
| FLEXIBILITY | POST | 8.86 | 0.19 | 0.53 | 0.62 |
| ROM | POST | 18.80 | 0.94 | 0.98 | 0.33 |
DISCUSSION:
At some American pain clinics, the prevalence of myofascial pain syndrome has been registered as high as 85%. MTrPs are treated in a variety of ways, according to several reports. Physical therapy ( posture correction and body mechanics), IC, Massage, MET strain counter strain (SCS), and electrical modalities such as laser, ultrasound therapy, TENS and electrical and invasive methods like acupuncture, trigger point injection of treatment.
The study involved 20 patients divided into two groups of 10 each. Positional release therapy was given to Group A, while myofascial trigger point therapy was given to Group B. Pain severity was assessed using a NPRS scale, flexibility was measured using (PKET) and range of motion was measured using goniometer before treatment (preRx) and after 2 week of treatment.
The first objective of the study was to see if positional release therapy could reduce pain, improve flexibility and increase range of motion in the HAMSTRING trigger points pain. After 2 week of treatment, the overall effectiveness of Group A on NPRS score was determined using the paired t-test, which shows P value is 0.00. Significant effect for flexibility was found using paired t-test which shows P value is 0.00. Range of motion was found using paired t-test which shows P value is 0.00. This means that positional release therapy is effective for reducing pain, improve flexibility and improve range of motion
The study’s second objects was to determine the effectiveness of myofascial trigger point therapy (Group B) on hamstring trigger point pain. After 2weeks of treatment the overall effectiveness of myofascial trigger point therapy on NPRS score was found using the paired t-test, which showed P value is 0.00. which is important. After 2 week of treatment, flexibility was found using a paired t-test, which shows P value is 0.00.which is significant for hamstring muscle flexibility. Range of motion was found using a paired t test, which shoes P value is 0.00 which is significant for ankle dorsi flexion rang
The study is third objective was to compare the effectiveness of positional release therapy (Group A) verses myofascial trigger point therapy (Group B) treating hamstring trigger point pain. When comparing NPRS scores between Group A and Group B statistical analysis indicates the same decrease. There is no significant change in pain reduction. According to statistical analysis, group A and group B both were showed an
improvement in hamstring trigger point pain. When comparing in flexibility between groups A and B, it can be shown that both Groups have a same improvement in flexibility at the end of the treatment. When comparing in Range of motion between Groups A and B, it can be shown that both groups have a more increase in range of motion at the end of the treatment
Result of this study goes with the study conducted by Sabby et al. The trigger points in this region may be subjected to ischemic pressure, which prevents blood from flowing into the affected area, rendering it is ischemic (deprived of oxygen). As if pressure is being released after 8 to 20 seconds, and the supply of blood, oxygen and nutrients to the region improves. In addition, general massage of the hamstring trigger point surrounding muscle is necessary for keep the ankle joint working properly and speed up the rehabilitation process
The results revealed that both groups i.e. Group A and Group B were statistically successful in their respective treatments. Furthermore, the t-test performed with SPSS revealed that both treatments were equally successful. As result, it can be concluded that the effects of positional release therapy and myofascial trigger point therapy are similar in treating hamstring trigger points pain
The study’s main flaw was that it used a small sample size and only looked at the short-term effects on discomfort, range of motion, and endurance, rather than the long-term effects. Future research should look into the long-term effects of positional release therapy and myofascial trigger point therapy on the trigger points, as well as different age ranges.
CONCLUSION:
It is concluded that the Positional release therapy is equally effective to myofascial trigger point therapy in decreasing pain, improving hamstring flexion knee extension ROM, and flexibility for hamstring trigger points pain. Both of these techniques should be used as a treatment of the hamstring trigger points pain
CLINICAL IMPLICATION
The data suggest that the physiotherapy treatment is effective in patients with hamstring trigger points. The treatment is given in a specific sequence with other treatment protocols, positional release therapy or myofascial trigger therapy proved to be more effective than any of the other protocols or interventions that were given alone to the patients with hamstring trigger points. Furthermore, the procedure offers significant relief to the patient with hamstring trigger points, as shown by the results. This research aimed to see whether there was a substantial difference in pain, range of motion, or responsiveness in patients with hamstring trigger points.
SUMMARY:
In this study, participants in the age group of 18-30 years with hamstring trigger points were compared to two treatments: positional release therapy and myofascial trigger point therapy. A total of 20 patients were randomly divided into two groups based on the inclusion and exclusion criteria. Positional release therapy was given to group A, while myofascial trigger point therapy was given to group B. outcome measures included
NPRS, ROM of ankle joint and flexibility of hamstring muscle. Both treatments are significant for relieving pain, improving ROM and for flexibility in hamstring trigger points. Also it is concluded that both of these treatments were equally effective and significant for the hamstring trigger points pain
LIMITATIONS AND RECOMMENDATION
LIMITATIONS:
- Small samples are used for the study.
- Duration for the study was short.
- A limited area is selected for the study.
RECOMMENDATION
- More study should be conducted with large sample sizes.
- Study can be done for a longer duration of period.
- Study should be done for the long term effect of treatment.
- Modern technologies or treatment protocols end out to improve the result.
REFERENCES:
- Human anatomy; B.D.Chaurasia Volume2; sixth edition
- AL-shawabka SA, Shenouda MM, Balboa AA, Positional release technique versus manual pressure release on the upper trapezius muscle in patients with myofascial pain, dysfunction syndrome. Bulletin of faculty of physical therapy.2013;18(1).
- Huguenin LK. Myofascial trigger points; the current evidence. Physical therapy in sport. 2004Feb1; 5(10:2-12.
- Simons DG, Travel J, Simons LS. Myofascial pain and dysfunction: the trigger point manual. 2nd Ed, vol.1. upper upper half of the body. Baltimore: Williams and Wilkins; 1999..
- Han SC, Harrison P. Myofascial pain syndrome and trigger-point management. Reg Anesth.1997;22:89-101
- Trigger points: Diagnosis and Management PDF PRINT COMMENTS David J. Alvarez, D.O., and Pamela G. Rockwell, D.o., University of Michigan medical school, Ann Arbor, Michigan. 2002Feb
- A Comparative study on the immediate Effect of co-Contraction of hamstrings versus slows Eccentric Isotonic stretch on hamstrings Flexibility among Healthy Young Individual; Thakker Sonal Rajeshkumar
- Jesudas Mazumdar, Jitendra Kumar Shriwas; a comparison between Mulligan traction straight leg raise technique vs muscle energy technique on hamstring tightness in asymptomatic male; Int J physiotherapy res 2014, vol 2(2):412-17
- Carol A. Oatis; Kinesiology – The mechanics and pathomechanics of the human movement, 2nd edition, Lippincott Williams & Wilkins, 2009-pg-845-849.
- Yasuhiro Endo, PT, Ph.D., Masaaki Sakamoto, PT, Ph.D., the relationship between lower extremity tightness and star excursion balance test performance in junior high school baseball players. Phys.Ther. sci.26:661-663,20ANNEXURES
- Voss DE, lonta MK, Myers BJ. Proprioceptive neuromuscular facilitation, patterns and technique. 3rd ed. Philadelphia: Harper and Row;1985.
- Amini, Ameneh, sakineh Goljaryan, seyed Kazem Shakouri, and Elapheh Mohammadimajd. “The effects of Manual passive Muscle Shortening and Positional Release therapy on latent myofascial trigger points of the upper trapezius: A double- Blind Randomized Clinical Trial.” Iranian Red Crescent Medical Journal 19,no.9(2017).
- Simons DG, Travell JG. Chronic myofascial pain syndromes. Mysteries of thehistory, chapter 6. In: Fricton JR, Awad EA, editors. Myofascial pain and fibromyalgia, Advances in pain Research and therapy. Vol. 17. New York: Raven Press; 1990.p. 129-3
- Measurement of joint motion; Cynthia C. Norkin and D.Joyce White; Fourth edition.
- Michener LA, Snyder AR, Leggin BG. Responsiveness of the numeric pain rating scale in patients with shoulder pain and the effect of surgical status.Journal of sport rehabilitation. 2011 Feb1:20(10):115-28.
- Gopal Nabi, Ronak sharma, Dipika Inbasekaran, Apeksha Vaghesiya, Urmi Bhatt. Difference in effects between ischemic compression and muscle energy technique on upper trapezius myofascial trigger points.
- Wang SS, Whintney SL, Burdett RG, Janosky JE, Lower extremity muscular flexibility in long distance runners. Joumal of Orthopaedic & sports physical therapy. 1993Feb; 17(2):102-7.
- Grieve R, Barnett S, Coghill N, et al. Myofascial trigger point therapy for triceps surae dysfunction: A case series. Manual therapy. 2013 Dec 1;18(6):519-25
- The Effect of static stretching of the calf muscle- Tendon Unit of Active Ankle Dorsiflexition Range of motion- James W, Youdas, David A, Krause, Kathleen S, Egan, Terry M, Therneau.
- Kelencz, Carlos Alberto, Victor Alexandre F. Tarini and Cesar Ferreira Amorim. “trapezius upper portion trigger points treatment purpose in positional release therapy with electromyographic analysis.” North American journal of medical science 3, no.10 (2011):451.
- Etnyre BR, Lee EJ. Comments on proprioceptive neuro muscular facilitation stretching techniques. Res Q Exerc sport. 1987;58:184-188.
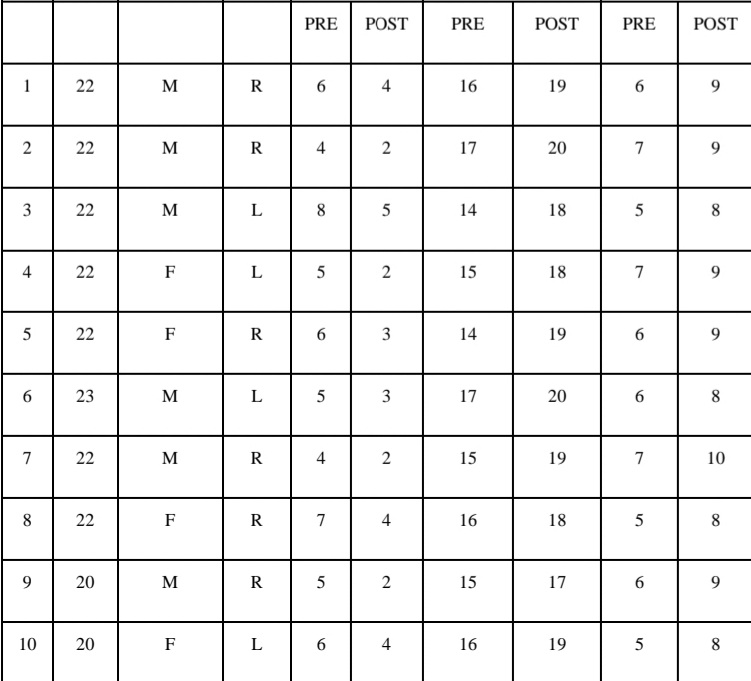
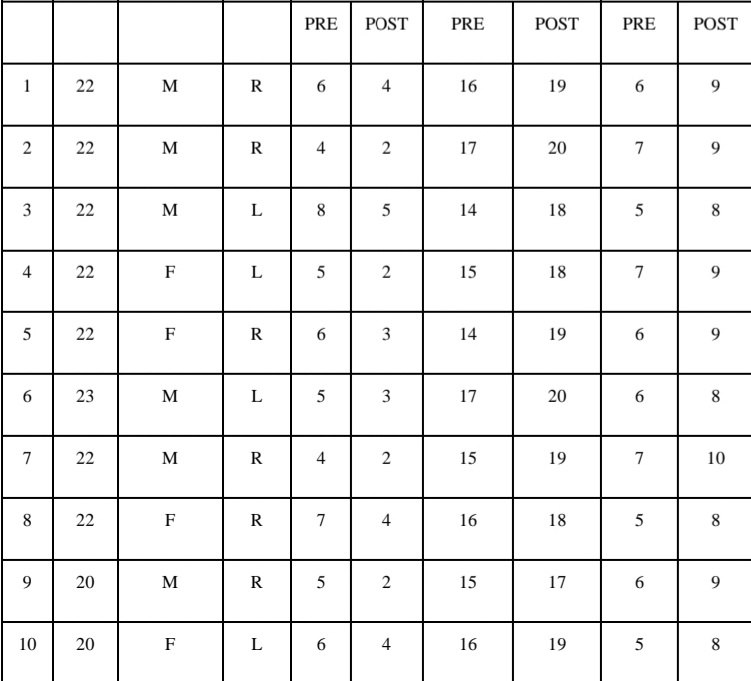
ANNEXURES :1
| ANNEXURES | ||||||
| SR NO | AGE | GENDER | SITE OF PAIN | NPRS SCALE | HIP FLEXION ROM | FLEXIBLITY |
ANNEXURE 2:
INFORAM CONSENT FORM:
Everything about this study has been explained to me in detail and I have been given a chance to ask questions about this research study. These questions have been answered to my satisfaction. And if there would be any further doubt or questions regarding the study. I am asked
to contact respected members of study. I understand that my participation in this study is voluntary. I may quit the study at any time without giving any reason. If I have any questions about my rights as a research subject I may contact respected members of the study. I understand that Ethics Committee and Regulatory Authorities will not need my permission to examine my records. I agree not to restrict the use of any data or result of the study provided as such a use is only for scientific purposes. By signing the consent form I have not waived any of my legal rights.
I am assured that I will be given a copy of this form
Contributors Name:
Signature:
ANNEXURE 3
PERFORAMA:
- Serial No:
- Patients detail:
- Name :
- Age :
- Gender :
- Occupation :
- Address :
- Contact no :
- Referred by :
- Chief complaint :
- History of present illness:
- Past history :
- Medical history :
- Surgical history :
- Personal history :
- Investigation :
- PAIN HISTORY:
- Side :
- Site :
- Onset :
- Duration:
- Type :
- Aggravating factor :
- Relieving factor :
- 24 hours pattern :
- Numeric Pain rating Scale:
- At rest:
- At activity
HEALTH AND MEDICAL INFORMATION
Are you currently receiving treatment for your pain?
Are you currently taking prescribed medications for your pain
OBJECTIVE EXAMINATION:
● Tenderness : SITE :
GRADE:
● Spasm/swelling/ atrophy:
● Gait :
AT REST:
AT ACTIVITIES

