EFFECT OF OPEN KINETIC CHAIN EXERCISE AND CLOSE KINETIC CHAIN EXERCISE ON PAIN AND FUNCTION IN PATIENTS WITH BACK PAIN
Table of Contents
Abstract:
Objective: To compare the effect of open kinetic chain exercise and close kinetic chain exercise on pain and function in patients with Low Back Pain.
Design: Experimental/comparative study
Background: LBP is the leading cause of occupational injury and disability. According to research Low back pain can be treated with kinetic chain exercises. OKC exercises and CKC exercises were used to treat the low back pain in this study
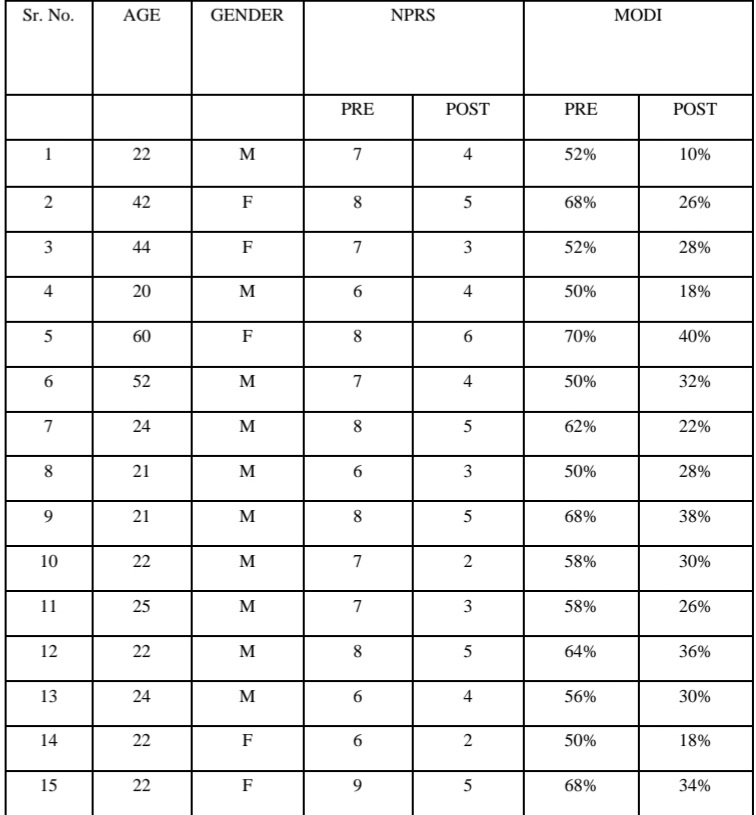
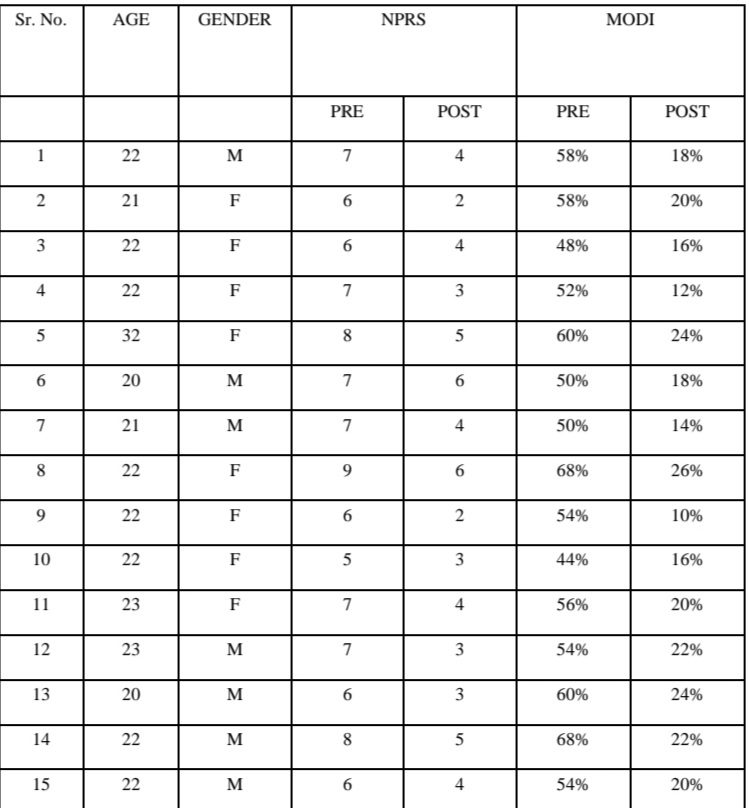
Method: 30 subjects with low back pain were selected. They were divided into 2 groups. Group A (n=15) participants were given OKC exercises. Group B (n=15) participants were given CKC exercises. Outcomes measures score of NPRs and MODI was taken before and after the treatment
Result: The results were obtained using paired and unpaired t-tests via SPSS. Both treatments were shown to be effective in reducing pain (NPRS-p-value-0.00) and improving function(p-value-0.00)
Conclusion: CKC exercises are more effective than OKC exercises for low back pain and function.
Keywords: low back pain,OKC exercises, CKC exercises
Abbreviation:
OKC: OPEN KINETIC CHAIN
CKC: CLOSE KINETIC CHAIN
LBP: LOW BACK PAIN
CLBP: CHRONIC LOW BACK PAIN
Introduction:
The section surrounded by the base of the rib cage and also the buttock creases is known as the lumbar spine. Some people with non-specific low back pain may also feel pain in their upper legs, but the low back pain usually predominates. Symptoms may be caused by a variety of structures, which may include joints, discs, and connective tissue
(1). Back Ache is described as “pain and discomfort situated between the lower rib cage and gluteal folds, with or without discomfort in the lower limb.”
(2) The most frequent type of low back pain is referred to as “Negligent low back discomfort.” and isn’t caused by an identifiable, well-known pathophysiology
3)The lumbar spine, the discs between the vertebrae, the ligaments around the spine and discs, the spinal cord and nerves, the muscles of the low back, the internal organs of the pelvis and abdomen, or the skin covering the lumbar region may all cause pain in the lower back
4). Since many people with low back pain experience peaks and valleys in their symptoms, a rigid classification system cannot always be sufficient. The popularity of backache varies widely, with estimates ranging from 33% for a single episode to 65% for 12 months and 84 percent for the whole life
5. Each year, approximately one-third of the adult population in the United Kingdom suffers from low back pain. Around 20% of these people (1 in 15 of the population) will see a doctor for their back pain. After a year, 62 percent of people with back problems still experience pain, and 16 percent of those who were previously unable to work are still unemployed. Pain and disability typically increase rapidly within the first month (58 percent decrease in both pain and disability scores), with no further progress after three months
(6). The prevalence of chronic back pain in the adult population is estimated to be 11% for the past 12 weeks, 23% of people had crippling back pain, 23% had low back pain that lasted more than 12 weeks and 18% had at least slightly bothersome discomfort.

Over 90% of people diagnosed with healthcare have non-specific back pain, and this is the number of people who seek physiotherapy for their back pain.
(7) physiotherapy evaluation aims to find abnormalities that could have led to the development of stress or increased the risk of experiencing chronic pain. Biological (e.g., fatigue, tightness), neurological (e.g., agitation, fear, anxiety), and economic circumstances also play a role (e.g., work environment)
(8)The evaluation should not rely on defining structural features (including the vertebral bodies) as the cause ofthe discomfort, as it would in multi forms like the knee
(9) Earlier studies and foreign recommendations say that identifying the precise tissue cause of pain is neither feasible nor appropriate for successful mechanical back pain relief.
(10) As a result, diagnostic imaging is not advised, especially in the first month. Diagnosing intervention should be used only if back pain does not lead to prescribed guidelines and the treatment of the affliction needs to be improved, or more severe activity is detected. Acute, sub-acute, and chronic low back pain are three subtypes of low back pain. This division is dependent on how long the back pain has been there.
(11) Acute back pain lasts less than one-month, sub-acute low back pain lasts for 1 to 3 months, and chronic low back pain lasts 3 months or longer since the movement of one joint in the kinematic chain necessitates motion of all other joints in the kinematic chain both proximal and distal part undergo resistance training at the same time while distal part is fixed. since the ckc technique emphasizes sequential
(12) since the ckc technique is frequently used to strengthen core muscles and maintain proper posture. can have the advantages of promoting a movement that makes everyday activation making more efficient.
Need of study:
Many different types of treatment approaches is used to treat low back pain. Most commonly used therapy consists of TENS, Inferential therapy, Electrical stimulation, Ultrasound, massage, and Exercise.
Many studies and researches show the benefits of OKC exercise and CKC exercise or assess the effectiveness of OKC ex and CKC ex for LBP. As previous research had givstatedat OKC exercises are beneficial for isolating a muscle and strengthening the muscle group whereas CKC exercises are exercises and functional.
OKC and CKC exercises are more reliable measures to check function in low back pain patients. So here we are comparing these two, OKC and CKC exercises to check the effectiveness of both the exercises in patients with LBP. Thus, the study will be done to find out the effectiveness of both tests.
Aims and objectives :
Aims:
To determine the effect of open kinetic exercise and close kinetic exercise on pain and function with Back pain.
Objective:
The purpose of this study was to see how successful the OKC exercise was at reducing pain and improving function in patients with low back pain. The purpose of this study was to examine the effects of OKC and CKC exercises on pain and function in adults with low backache.
Hypothesis:
1. Null Hypotheses: There is no significant difference in the effects of open kinetic exercise and close kinetic on pain and function with Low Back Pain.
2. Alternative Hypotheses: There are significant differences in the effects of open kinetic exercise and close kinetic on pain and function with Low Back Pain.
Review of literature:
1. Hestbaek L, et al, March 2015 studied lifestyle factors in adolescence predictors for adult low back pain. A cross-sectional and prospective study of young twins. BMC musculoskeletal disorders. The outcome measure for validation and reliability were concluded by Nordic Back Pain Questionnaire. Has taken age 12-22 years to participate in the study. There were two groups randomly divided Group A present LBP (cross-sectionally) and Group B the risk of future LBP (longitudinally). The study failed to confirm the significance between smoke and LBP.
2. Caleb Ademola et al, 2013, Comparative Efficacy of Open-chain and Closed chain Kinematics on Proprioception, Muscle Strength, and Functional Performances in Knee Osteoarthritis Patients. A total of 25 participants were taken for this study. They were divided into two groups. Group A was an open-chain exercise and Group B was Close chain exercise. The outcome measure for open versus close chain exerciser concluded by pain using the VAS scale, for function Functional index questionnaire, and active range of motion. A close chain is more effective than an open-chain exercise.
3. Tan K1, et al. 2009 concluded that the Oswestry Disability Index has satisfactory validity and reliability in patients with low back pain in Shandong. Outcome measures taken was the Oswestry Disability Scale for the patients to check patients with low back pain. Participation of 86 patients in this study and was taken for reliability and validity for chronic low back pain. The Oswerty Disability index has satisfactory reliability and index. It is an instrument which can be used for assessing chronic low back pain disability.
5. O’Sullivan PB, et al, 1997 studied that in the treatment of persistent LBP with a radiologic diagnosis of spondylolysis or spondylolisthesis, a special stabilizing exercise was evaluated. A total of 44 patients were taken for the study and were divided into two groups. Group A was a specific exercise group and Group B was a Controlled group. The specific exercise group showed a reduction in pain and function disability levels while the control group showed no reduction in intervention.
6. Sang wk Lee, (2) 2015 investigated that hip exercises are more effective than typical therapeutic exercises for CLBP patients with lumbar instability, according to the study “Effects of hip exercises for CLBP patient with lumbar instability.” in patients with low back pain and lumbar instability. Outcome measures taken were the VAS scale for intensity and KODI questionnaire for functional disability. A total of 78 subjects was taken for the study which was divided into 2 groups. Group A has 45 patients and Group B had 33 patients. Group a was the Lumbar stability Group and Group B was the Lumbar Instability group. Lumbar instability was more effective than lumbar stability in chronic low back pain.
7. Abdel Rahim Eliel, et al, 2017, Exercise regimes of open and closed chains: an ultrasound study of the impact of exercise on the architecture of the vastus of edialis oblique. Ultrasound was used to check the muscle while the goniometer was used to check the degree of movement in the joint. Total 23 patients were taken in this study. They were divided into two groups. Group A was an open-chain exercise and Group B was a Close chain exercise. It was concluded that both the exercises are equally affected vastus medialis.
8. Jonathan R. Blackburn et al, 2021, The relationship between the lower limb’s open and closed kinematic chain strength and jumping results. They are divided randomly into two groups. Manual muscle testing was used as an outcome for strength. Group A open chain and Group B is a closed chain. Closed chain exercise is more effective than open-chain exercise.
9. Carolyn A. Richardson, Ph.D. et al (12) 2002 conducted a study “The Transverse Abdominis Muscles, working of SI joint, and Backache” this study examined the effect of the exercise on low back pain, Targeting the transverse abdominis and multifidus muscles. Thirteen healthy individuals were included the user in the study. the SI joint laxity values were r means of Doppler imagining of vibrations and muscle patterns were verified by electromyographic recordings and ultrasound imagining. This study concluded that contraction of trans versus abdominal muscles creates bracing action which significantly reduces the laxity of the SI joint. This finding was independently used for treating LBP with the use of activating transverse abdominis.
10. B. Mengiardi, et al, 2006 investigated the Quantification of MR spectroscopy used to examine the fat content of the lumbar paraspinal musculature in patients with persistent low backache and asymptomatic volunteers in Radiology. Total of 50 Patients were taken for the study. They are divided into two was total. Group A had 25 patients and Group B had 25 patients. Group A was of chronic low back pain patients and Group B with was asymptomatic patients. It demonstrated that higher fat content in multifidus muscle in patients with chronic low groups backs pain than in asymptomatic pain.
11. Ershad, N., et al,2009 concluded the Evaluation of trunk muscle activity in chronic low back pain patients and healthy individuals during holding loads. Journal of Back and Musculoskeletal Rehabilitation. EMG was used as an outcome measure to check the patients with chronic low back pain. Total 20 Patients were taken in this study. Group A with 10 female patients and Group B with ten healthy subjects were taken. Group A with chronic low back pain and Group B with healthy patients. HA higher levels of the global and lower and local level of local activation of abdominal muscles with CLBP may represent that pain changes neuromuscular control systems.
12. S. Kumar, et al 2009 studied the Efficacy of dynamic muscular stabilization methods in chronic low back pain compared to traditional techniques. 2651-2658 in Journal of Strength and Conditioning Research, 23(9). The outcome measure used was VAS for pain and Response dependent variable for Function. A total of 30 players were taken in the age group of 18-22 years having subacute and chronic low back pain. They were assigned to 2 different groups. OKC Group was examined with conventional therapy and the CKC group was examined by dynamic muscular stabilization techniques. It was concluded that DMST is more suitable than conventional therapy for early treatment.
13 E B Bynum et al, 1995, After anterior cruciate ligament repair, open versus closed chain kinetic exercises were compared. A prospective randomized controlled trial. The study was divided into two groups randomly. The outcome measure used is the Lysholm knee scoring scale and the Huston clinic questionnaire was used. Group A and Group B. Group a had an open-chain exercise and Group B had a close chain exercise. The closed chain exercise was more effective than the open-chain exercise.
14. Karen D.Kendallae, et al, Carolyn A “The effects of incorporating hip strengthening to a lumbopelvic complexity exercises program for the treatment of non-specific low backache,” according to a systematic review experiment. was performed by Wiley, Reed Ferberad (November 2015) and found that in persons with non-specific low backache, adding hip-strengthening exercises to a motor skills training process had no impact.
Material and methods:
Method of collection of data:
- Study design — Comparative design
- Study Subject – Patient with low back pain
- Sample size – 30 patients Period- 4 weeks – 4 days/week (excluding Sundays and holidays)
- Sample design – convenient random sampling
- Source of Data –Ahmadabad
Material:
- Consent form
- Plinth
- Pen
- Pencil
- Paper
- Pillow
- Comfortable clothes
inclusive criteria:
- A patient who can follow the command.
- Patients of age group from 20 to 60 years.
- A patient who can do exercise.
- Patient with sciatica from lumbar intervertebral disc herniation.
- Both males and females are included in this exercise.
Exclusive criteria
- History of Psychological Disorder has no choice
- Patient of age group 60 or above has no choice
- Unhealthy Patient has no choice
- Pregnant lady has no choice
- Patient with RA has no choice
- Patient with a spinal tumor has no choice.
- History of any operation related to spine. Ex. Vertebral fracture or dislocation has no choice.
- Severe neurological deficit or symptoms including nerve compression. Ex. Cauda equina Syndrome has no choice
Outcome measure
Numeral pain rating scale:
The Numeric Pain Rating Scale is subjective. It’s an improved version of the Visual Analog Scale, which had 0-10 numeric values in 10 cm rows, with 0 denoting “no pain,” 10 denoting “worst pain,” and 5 denoting “reasonable pain severity.”
Over the line, the patient was asked to mark or show the severity of pain. The ICC Inter class Co-relation Co-efficient value for NPRS reliability is 0.92–098; this indicates excellent reliability
Modified oswerstry disability index:
This is a functional scale that was created to include details about a patient’s back pain and how it affects their ability to perform everyday activities. Several things are included in the questionnaire. Grade each operation on a scale of 0 to 5, with a maximum of 50 points.
The MODI is calculated using a percentage ranking method, with the higher the percentage value, the lower the love for everyday activities
Methodology:
Following Institutional Ethics acceptance, participants were divided into the following groups based on inclusion criteria. Group A received open kinetic exercises (n = 15), while Group B received closed kinetic exercises (n = 15). The objective of the test and the test procedure were explained to the subjects. Before the study, a written consent form was obtained.
Procedure:
A total of participants were divided into two groups. each group was divided into 15 patients with low back pain.
Open kinetic chain exercises:
- SLR
- Hip abduction
- Knee to chest
- SLE in prone
- Partial curl ups
1) SLR:
When performing the SLR, the patient is positioned supine without a pillow under his/her head, the hip medially rotated and adducted, and the knee extended. The clinician lifts the patient’s leg by the posterior ankle while keeping the knee in a fully e ended position. The clinician continues to lift the patient’s leg by flexing at the hip until the patient complains of pain or tightness in the back or back of the leg
2) Hip Abduction:
A patient will be in a side-lying position. The lower leg will be flexed from the knee to 90°. The patient is asked to raise the other leg. The patient is asked to raise the leg as much as possible. Perform 3 repetitions.
3) Knee to chest:
Lie down on your back, knees bent and feet parallel to the ground. Keep one foot level on the floor while bringing one knee to your chest. Relax and lower the knee to the starting position. Repeat 2 to 4 times with each leg
4) Sle in prone:
Hold your straight leg up in the air for two seconds, and then slowly lower your leg back to the floor. Be sure you do not rotate your back or your pelvis while lifting your leg. Perform the exercise slowly for 10 to 15 repetitions, and then repeat the exercise for the opposite leg.
4) Partial curl ups:
Cross your arms loosely. Tighten your abdomen and curl halfway up, keeping your head in line with your shoulders. Hold for 5 seconds. Uncurl to lie down. Repeat 2 sets
Closed chain exercises:
- Bridging
- Prone bridge
- Lateral brige
- Back extension in prone
- Cat&camel exercises
1) Bridging:
The patient was lying in a crook position with his knees and hips flexed. Both patients’ palms are facing the floor or plinth to provide support. The patient was lying in a crook position with his knees and hips flexed. Both patients’ palms are facing the floor or plinth to provide support. Both of the patients’ feet were placed on a flat surface, and the patient was advised to progressively raise the pelvis by pressing both feet at the same time, while maintaining both hands should be under the same amount of pressure. After the patient has been raised, instruct them to clench and then release their gluteal muscles until carefully dropping to the plinth or ground. The patient was lying in a crook position with his knees and hips flexed. Both patients’ palms are facing the floor or plinth to provide support. Rest for a few seconds before repeating the process 15 times in a row. Three sets of 15 repetitions were completed
2) Prone bridging:
The prone bridge begins in the same way as a push-up, except the elbows are bent and the forearms are flat on the floor. The palms may either lie on the floor or be interlaced together with the fingertips. Then, lift your body off the floor with your elbows and toes. Two sets of 7 repetitions each
3) Lateral bridge:
Keep your body in a straight stance on your side, supported only by one arm and the side of one foot. As core stability muscles, strong obliques can be extremely beneficial. Two sets of 5 repetitions each
4) Back extension in prone:
Lie on a mat on your stomach and straighten your legs behind you. Place your elbows on the ground and slide your shoulders down. Lift your upper back, pressing your hips into the mat. Keep your head and neck neutral. Hold for 30 seconds. Lower to starting position. Complete 3 sets
5) Cat & camel exercise:
Make sure your hands are under your shoulders, your knees are under your pelvis, and your back is in a linear direction before getting down on your hands and knees.
Cat: Sink your back towards the floor and lift your head at the same time, sticking your tailbone out to make a curve with your spine. Take a big breath out at the
Camel: Tuck your head and tailbone in, arching through your spine as to mimic a camel hump. Take a big breath in at the same time
Statistical analysis:
The statistical analysis was carried out using the SPSS statistical kit. The data was found to be naturally distributed. The unpaired and paired ‘t’ tests were used to compare data ithin and between groups A and B. The sample evaluation of the post values of the outcome variables of both groups yielded the conclusion.
Result:
A comparative study for the open kinetic chain exercises and close kinetic chain exercises was conducted which consisted of 30 subjects, divided randomly into two groups. OKC Exercises were offered to Group A, which consisted of 15 people. CKC Exercises were provided to Group B, which consisted of 15 subjects. To find important differences in pre and post-treatment scores, and also assess the groups for efficacy, paired and unpaired ‘t-tests were used. The data were reported using the mean, normal distribution, and t value.
| group | mean | SD |
| A | 21.56 | 11.36 |
| B | 28.64 | 16.90 |
TABLE 2:BASELINE COMPARISON OF PRE INTERVENTION OUTCOMES OF BOTH GROUPS
| OUTCOMES | OKC GROUP | CKC GROUP | T VALUE | P VALUE |
| NPRS | 6.2±0.9411 | 6.80±1.01419 | 0.972 | 0.348 |
| MODI | 58.40±7.67929 | 55.60±6.72734 | 1.002 | 0.33 |
TABLE 3: COMPARISON OF OUTCOMES WITHIN GROUP
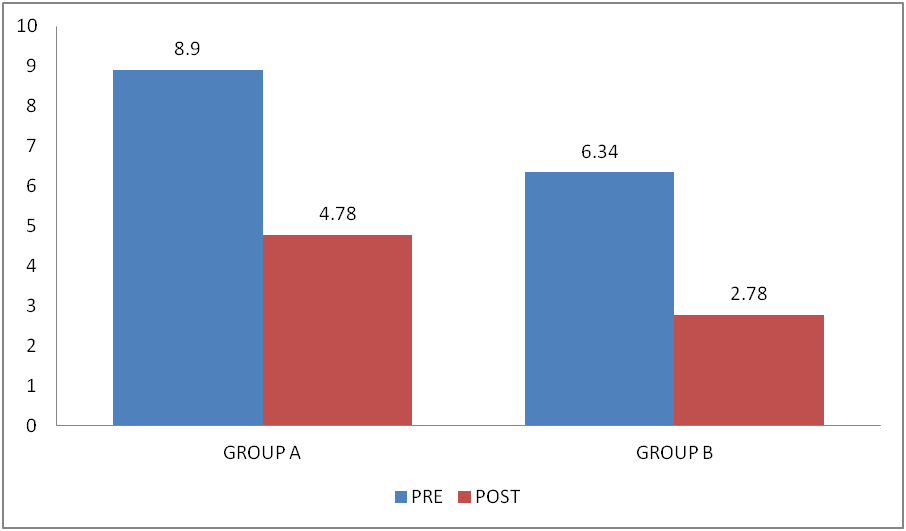
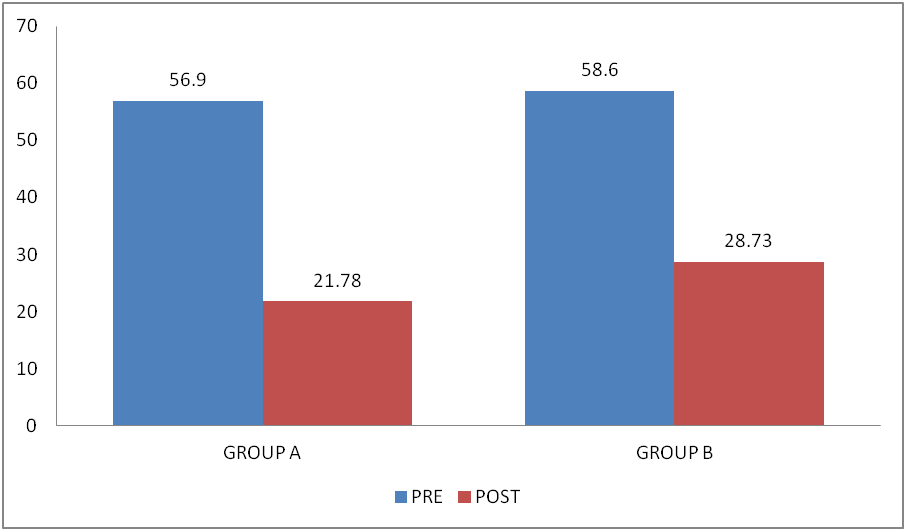
GROUP A
| outcome | mean | sd | T | P | |
| NPRS | PRE | 8.90 | 1.30 | 13.56 | 0.00 |
| POST | 4.789 | 1.09 | |||
| MODI | PRE | 56.90 | 4.89 | 28.02 | 0.00 |
| POST | 21.78 | 7.67 |
GROUP B
| OUTCOME | MEAN | SD | T | P | |
| NPRS | PRE | 6.34 | 0.89 | 14.56 | 0.00 |
| POST | 2.78 | 1.97 | |||
| MODI | PRE | 58.60 | 8.19 | 17.12 | 0.00 |
| POST | 28.73 | 7.12 |
Graph 1: Comparison of NPRS within the group analysis
Graph.3: Comparison of MODI within group analysis
Discussion:
A kinematic chain refers to the motion that these joints and segments provide on one another when moving. when one runs along, a chain of events occurs that affects the movement of adjacent joint segments. Physicians, chiropractor, and personal trainers use kinematic chain driss to help in accident prevention and recovery as well as body sculpting.
while there is a large body of research on vocational training using a range of approaches, reviews on educating patients for the low back problem have largely concentrated on written content. there is no data such publications are the most successful way to achieve instructional objectives
some previous work has asserted that ckc rehabilitative exercises are safer in terms of pain. the result of the present study was consistent results suit with results found in the evidence. to the author’s knowledge, there where insufficient evidence within the literature pool that either supports or dispels this opinion.
the primary goal of this study was to test the hypothesis that the comparative effect OKC exercise and can exercise on low back pain function of patients effects C with low back pain overall result of the study indicated that the ckc exercise has a more significant effect than OKC exercise on low back pain on functional outcomes.
An experimental study was conducted to find out the effectiveness of OKC and can exercise on pain and function in low back pain. the study implemented for four weeks a numeric pain rating scale Modified Oswestry low back pain disability index (MODI) were the outcome measures of the study. After four weeks re-assessment of all outcome measures was carried out and analyzed by SPSS. The baseline comparison of data was made for the group A- OKC and group B- CKC group for the age, sex, and all other outcome mean sures. The normality of distribution was checked and both the groups were found compatible. The findings of this analysis revealed clinically relevant changes in NPRS, and functionality was measured using the procedure of the 16th session MODI following the procedure of the 16th sessio.
Beyond et al, 2009, demonstrated that CKC exercises and OKC exercises provide improvement in the strength of the muscle which is responsible for the alteration of joint stresses, and increase the ability to redistribute the load,bearing, and aring capacity of joints (26). According to Gregory Minnis et al. the lateral leg lifts (SLA) work on the hip abductors muscles. The primary function of the muscle is to provide support to the pelvis and divert pressure on the back, keeping these muscles strong is essential as they help a person maintain their balance and can affect mobility. Performing straight leg raise exercises to activate a different group of muscles can prevent injury, increase stability, and improve flexibility.
Gregory Minnis stated that performing knee to chest stretch can help to elongate the lower back muscles, relieving tension on the muscle and reducing pain by activating stretch receptors. Furthermore, the author stated that the cat and camel exercises can also provide stretch to the back muscle, and contraction help to provide strength to the back muscle. Which are responsible for generating tension in the muscle which can help to reduce the pain and improve mobility of the segments. The findings of the present study are consistent with the findings of Gregory Minnis. Thus, it can be hypnotized that the same mechanism can help to reduce pain and improve function in the present study.
C. Richardson et al conducted an EMG study on core muscle activation patterns. The conclusion of the study suggested that targeted core muscle strengthening via drawing in maneuver help to improve the strength of local and global muscles which can lead to improvement in endurance, flexibility, pain, and function. the finding of the study was similar to F, France et al. literature, where the author suggested that strengthening the core and pelvic floor muscles can help to reduce low back pain and improve the quality to the activity of daily living. The finding was consistent with the present study which suggested that various forms of open kinetic exercises and close kinetic exercises can target the specific group of muscles that redistribute the weight-bearing capacity of the joints of joint by providing stability and strength to the surrounding muscle. (Beynon et al, 2009)
Brett Sears, stated that performing the prone hip SLR exercise during rehabilitation benefits, after lumbar surgery of benefit in pain, mobility and function. (18) Dannelly et al. (2011) reported that the sling exercise is a variation of the kinematic chain exercise system that leads to improvement in balance by using both local and global muscles. Godfrey et al. studied the effect of partial curl-ups and found that it has an effect on the recruitment pattern of the abdominal muscles which enhances the performance of the muscle
Mooney et al. also examined activation patterns for torso rotation exercise shows the finding of the study show abnormal muscle activation patterns in symptomatic participants compared to the control group. Post-intervention with progressive resistance training analysis of the torso rotation via device was carried out and found that the activation pattern had been returned to the normal level in asymptomatic participants. The mechanism responsible for the proper mechanism was probably the same which was explained by Beynon et al, 2009 and C. Richardson et al.
The results of the present study revealed that both groups i.e., Group A and Group B were statistically significant in their respective treatments. However, the mean of the c se kinetic chain exercises were compare to the open kinetic chain was higher. Thus, it can be concluded that the effects of close kinetic exercise were more effective in treating patients with low back pain compared to the open kinetic chain.
Conclusion:
This study concludes that close kinetic chain exercises are more effective than open kinetic chain exercises in decreasing pain and improving function for low back pain.
Clinical implication:
Low back pain is the most common ailment among today’s population. LBP is caused by various reasons such as muscle or ligament injury. Improper lifting, poor posture, a lack of physical exercise, and arthritis are all common causes of LBP. So extra precautions should be taken in patients with lower back pain. Various forms of exercise are used to treat low back pain. Currently, exercises that are related to open and close kinetic chains are used to relieve pain and improve functions in low back pain. Both exercises can help to strengthen the muscles in the lower back. According to the present study, open kinetic chain exercises are used to isolate a muscle or improve a specific muscle group function and strength, whereas close kinetic chain exercises are safe and effective for reducing LBP. Closed kinetic chain exercises are more functional and beneficial in patients with LBP because they are more closely related to everyday activities.
Summary:
An experimental study looked at the “In patients with low back pain, the effects of open kinetic exercise and closed kinetic exercise on pain and work “. A total of 30 patients were involved in this study. A convenient random sampling technique was used to select all of the subjects.
A total of 30 patients were taken in this study. They were divided into two groups. Each group consists of 15 patients. Group A was assessed with open kinetic exercise and Group B was assessed with Close kinetic exercise. Then the patients were assessed using the NPRS and MODI for the pre-intervention outcomes measures. The interventions were carried out four days a week excluding weekends and holidays. The statistical analysis results were produced using the SPSS 26 software
Limitation and further scope:
Limitation:
- The study’s limitation is that the sample size was small.
- A limited area is selected for study.
- The duration of study was short
Recommendation:
- More research with large sample sizes should be performed.
- Study should be done for the long-term effect of treatment.
- The use of modern technology or care protocols improves the outcome. Ex: acupuncture, IMS (intramuscular stimulation).
- Larger sample size is needed for a more reliable result
Reference:
1. National Collaborating Centre for Mental Health (Great Britain), National Institute for Health, Clinical Excellence (Great Britain)2009 May. Alcohol use disorders: The NICE guideline on the diagnosis, assessment and management of harmful drinking and alcohol dependence.
2. Burton AK. European guidelines for prevention in low back pain. COST B13 Working Group. 2004: 1-53.
3. Kinkade S. Evaluation and treatment of acute low back pain. Am Ac of Family Phys. 2007: 1182-1188.
4. Aure OF, Nilsen JH, Vasseljen O. Manual Therapy and Exercise Therapy in Patients with Chronic Low Back Pain: A Randomized, Controlled Trial With 1-Year Follow-Up. Spine. 2003;28(6):525-532.
5. Walker BF (1996). J Spinal Discord (2000). The prevalence of low back pain, a systemic review of literature from 1996 to 1998.
6. Pengal LH, Herbert RD, Maher CG et al. 2003, Acute low back pain, systemic review of its prognosis. BMJ. 327(7410):323[PubMed].
7. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2017; 166: 514-530.
8. Van Wambeke P, Desomer A, Ailliet L, et al. Summary: Low back pain and radicular pain: assessment and management. KCE report 287Cs. Brussels: Belgian Health Care Knowledge Centre (KCE), 2017.
9. Foster N.E, Hill J.C, O’Sullivan P, Childs J.D, Hancock M.J. Stratified models of care for low back pain. WCPT Congress, Singapore, 2015.
10. Koes BW, van Tulder MW, Thomas S. Diagnosis and treatment of low back pain. BMJ 2006; 332:1430–34.
11. M.Hancock. Approach to low back pain. RACGP, 2014, 43(3):117-118.
12. Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD, Maher CG, Refshuage KM. Comparison of General Exercise, Motor Control Exercise and Spinal Manipulative Therapy for Chronic Low Back Pain: A Randomized Trial. Pain. 2007; 131:31-37.
13. Chou R, Qaseem A, Snow V, Casey D, Cross TJ, Shekelle P, Owens DK. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007; 147:478-491. 14. Stochkendahl MJ, Kjaer P, Hartvigsen J, et al. National Clinical Guidelines for non-surgical treatment of patients with recent-onset low back pain or lumbar radiculopathy. Eur Spine J 2018; 27: 60-75
14. Stochkendahl MJ, Kjaer P, Hartvigsen J, et al. National Clinical Guidelines for non-surgical treatment of patients with recent-onset low back pain or lumbar radiculopathy. Eur Spine J 2018; 27: 60-75.
15. Daniel Bubnis, M.S., NASM-CPT, NASE Level II-CSS — Written by Anna Schaefer — Updated on January 31, 2019.
16. Akuthota V, Herring SA. Nerve and vascular injuries in sports medicine. Springer, 2009.
17. McCaffery, M., Beebe, A., et al. (1989). Pain: Clinical manual for nursing practice, Mosby St. Louis, MO.
18. Modified by Fritz & Irrgang with permission of The Chartered Society of Physiotherapy, from Fairbanks JCT, Couper J, Davies JB, et al. The Oswestry Low Back Pain Disability Questionnaire. Physiotherapy. 1980; 66:271-273.
19. Comparative Effectiveness of Straight Leg Raise and Slump Stretching in Subjects with Low Back Pain with Adverse Neural Tension January 2012 International Journal of Health and Rehabilitation Sciences (IJHRS) 1(1).
20. How to Do Back Extension Exercises. Medically reviewed by Daniel Bubnis, M.S., NASM-CPT, NASE Level II-CSS — Written by Kirsten Nunez on April 1, 2019.
21. Gregory M, Bethany C.; How to strengthen the lower
back;(medicalnewstoday.com) January 24,2020.
22. How to Perform the Prone Straight Leg Raise Exercise. By Brett Sears, PT Medically reviewed by Laura Campedelli, PT, DPT on November 25, 2019.
23. Gregory M, Bethany C.; How to strengthen the lower
back;(medicalnewstoday.com) January 24,2020.
24. A. Luque-Suárez, E. Díaz-Mohedo, I. Medina-Porqueres and T. Ponce García (May 2016) Physiotherapy Department, Malaga University, Spain. Stabilization Exercise for the Management of Low Back Pain.
25. Best stretches for lower back flexibility and pain relief Medically reviewed by Daniel Bubnis, M.S., NASM-CPT, NASE Level II-CSS — Written by Aaron Kandola on July 23, 2020.
Annexure1:
- Introduction: We Hereby invite you to participate in a study designed to know about the Effect of open kinetic exercise and close kinetic exercises on patients with low back pain.
- Purpose of the study: The purpose of this study is to examine the “Effect of open kinetic exercise and close kinetic exercises on patients with low back pain”.
- Procedure: Patients with low back pain will be recruited, assessed divided into two groups, and the effects of the above-mentioned techniques will be seen. The first group received an open kinetic exercise and the second group received with close kinetic exercise for the low back.
- Benefits: There may be a reduction in pain and improvement in function after the interventions.
- Risk: There is no risk in this study
- Financial incentive for participation: You will not receive any payment for participating in this study. It is a voluntary study.
- Authorization to publish results: Results in this study may be published for scientific purposes and/or presented to scientific groups; however, your identity will not be disclosed.
Proforma:
- Name :
- Age :
- Gender :
- Occupation :
- Address :
- Contact no :
- Referred by :
- Chief complaint :
- History of present illness :
- Past history :
- Medical history :
- Surgical history :
- Personal history :
- Investigation :
- PAIN HISTORY:
- Side :
- Site :
- Onset :
- Duration:
- Type :
- Aggravating factor :
- Relieving factor :
- 24 hours pattern :
- Numeric Pain rating Scale:
- At rest:
- At activity:
HEALTH AND MEDICAL INFORMATION:
- Are you currently receiving treatment for your patient
- Duration of the study was short
- Are you currently taking prescribed medications for your pain?
OBJECTIVE EXAMINATION:
- SITE :
- GRADE:
- Spasm/swelling/ atrophy:
- Gait :
- Tenderness:
Master chart: