Valgus Stress Test
Table of Contents
What is a Valgus Stress Test?
The Valgus stress test is a clinical examination technique used by healthcare professionals, primarily in the field of orthopedics and sports medicine, to assess the stability and integrity of a specific joint, typically the knee or elbow. This test involves the application of a valgus force, which is a lateral (outward) stress applied to the joint, in order to evaluate the presence of any ligamentous or structural injuries.
The test aims to detect and diagnose conditions such as ligament sprains, tears, or other joint-related issues, helping guide treatment decisions and rehabilitation protocols. The valgus stress test plays an important role in the comprehensive evaluation of joint injuries and contributes to the development of targeted treatment plans for patients.
Introduction
The purpose of the valgus stress test, also known as the intermediate stress test, is to assess the integrity of the medial collateral ligament (MCL) of the knee. Medial collateral ligament injuries are common in athletes and can occur independently or in combination with other structural injuries.
Technique
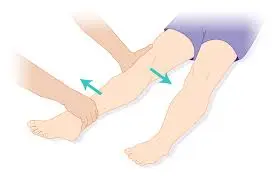
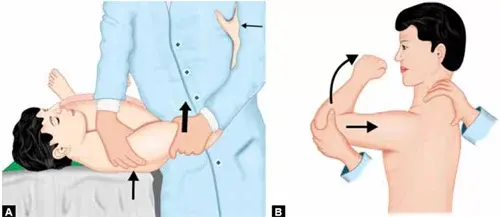
Before starting the technique, start with the patient in the supine position. The leg can be relaxed during the test. During the test, the examiner places one hand on the outside of the knee as a pivot point and the other on the leg. The researcher simultaneously applies an abduction force to the leg and a sliding force through the knee joint to palpate the medial joint line.
The test is usually performed with the knee flexed at 30 degrees and 0 degrees. When performed at a 30-degree angle, the average cruciate ligament differs from other average joint patterns, with a sensitivity of 0.86-.96 for an MCL tear. Another version of this test, which can be performed at 0 degrees of knee flexion, allows evaluation of other medial joint structures.
The two versions are summarized as follows:
- 0° knee valgus: The medial joint capsule, medial collateral ligament, anterior cruciate ligament (ACL), and posterior cruciate ligament (PCL) of the knee are all under tension.
- 30° knee valgus: The primary structure to assess is the medial collateral ligament, which acts as the primary stabilizer of posture. In this position, the medial joint capsule is under stress.
Positive findings
Positive findings include an excessive gap in the medial joint and/or pain, which may indicate damage to the medial collateral ligament. This may indicate capsular or even cruciate ligament laxity, depending on the level of knee flexion at which the test ends. It is worth noting that opening the joint at an angle of 30 degrees is considered normal. At 0 degrees, there may be no gaps.
The importance of this test
The medial safety assumes most of the stiffness of the knee and acts as an important light limiter in the flexed knee. With light forces, the anterior cruciate ligament is more stretched than the medial cruciate ligament is twisted, causing excessive knee motion (especially at 45 degrees of knee flexion). As a result, people with lax medial cruciate ligaments should take care to reduce the possibility of further injury, especially to the anterior cruciate ligament.
Interpretation
Positive findings may include an excessive gap in the medial joint and/or pain suggestive of an MCL injury. It may also indicate capsular or cruciate ligament laxity, depending on the degree of knee flexion at which the test is performed.
It should be noted that at an angle of 30 degrees, a certain common space is considered normal. There should be no difference at 0 degrees.
The meaning of the test
Overall, the MCL plays an important role in the stability of the knee and acts as the primary limiter of the flexed knee. When the hypermobility of the knee is due to an MCL sprain, the ACL is subjected to greater tensile loads with light forces (especially at 45 degrees of knee flexion).
Therefore, individuals with open MCL cancer must take special precautions to reduce the risk of further injury, especially to the ACL.
Diagnostic Accuracy: at 30 degrees: Sensitivity: 0.86-.96 (“Medial Collateral Ligament Tear: MRI Findings and Associated Injuries”, “Evaluation of Knee Instability in Acute Ligament Trauma”).
Significance of the test
The medial collateral ligament is an important light force resistance in the knee because it is connected to the femur, glenoid, and tibia. The MCL also plays an important role in limiting the external rotation of the tibia. Surgical excision of the superficial portion of the MCL has been shown to increase tibial external rotation approximately threefold at 90 degrees (Ellenbecker, 2000). According to Neumann, the MCL connects proximally to the medial epicondyle and posteriorly to the distal attachment of the peso anserinus distally to the anteromedial tibia.
The deeper fibers of the MCL are shorter than the superficial fibers and also attach to the posteromedial capsule, meniscus, and semimembranous tendon. Because the deeper fibers are shorter than the superficial fibers, they are more likely to be injured when loaded with light force, even though the superficial fibers resist the light force the most! On the other hand, the superficial fibers are more likely to be under tension during femoral tibial external rotation (or tibial internal rotation).
If the MCL is attached to the meniscus, be sure to also check for meniscal injuries if the mechanism of injury affects the MCL. At 0 degrees, there is usually no gap in light tension, so if there is a gap during the test, a serious injury is suspected, i.e. ACL, PCL, MCL, capsule (there is no difference, as the MCL, posteromedial capsule, hamstrings, oblique patellar ligament, and ACL parts are densest at full extension).
There is some gap in the 30-degree position because the MCL and other structures are no longer maximally stressed, but the MCL is the main stabilizer in this position. The MCL joint is one of the most important ligaments in terms of knee stability. With a hypermobile knee with a sprained MCL, it is important to take extra precautions to reduce the risk of further injury. With a lax MCL, the ACL is increasingly stressed by lateral forces, especially at 45 degrees of flexion (Ellenbecker, 2000). Remember that the MCL is the primary light restriction of the flexed knee; without it, the ACL is prone to injury.
FAQ
What is a positive valgus stress test knee?
Interpretation. Positive findings may include an excessive gap in the medial joint and/or pain suggestive of an MCL injury. It may also indicate capsular or cruciate ligament laxity, depending on the degree of knee flexion at which the test is performed.
What does the valgus stress test test for?
Your provider may perform a mild or moderate stress test if you have pain in your knee or elbow, or if you’ve injured your leg or arm. These tests help them check for damage to the ligaments that support the joints. Damaged ligaments are one of the most common sports injuries.
What are the findings of a valgus stress test?
Positive findings may include an excessive gap in the medial joint and/or pain suggestive of an MCL injury. It may also indicate capsular or cruciate ligament laxity, depending on the degree of knee flexion at which the test is performed. It should be noted that at an angle of 30 degrees, a certain common space is considered normal.
Which ligament in the knee is stressed by a valgus force?
Recently, patients have had excessive light force applied to the partially flexed knee (e.g., cutting injury in football). A common triad of injuries (especially in athletes) when light is applied to the knee is damage to the MCL, medial meniscus, and anterior cruciate ligament.
What injuries is the valgus test used to identify?
Damaged ligaments are one of the most common sports injuries. Damage to the ligament is called a sprain or tear. Many sprains are minor, but a torn ligament can be a serious injury. Mild stress tests are used to diagnose MCL injuries.
What causes valgus stress?
A combination of traction forces on the medial stabilizing structures, compression of the lateral compartment, and posterior shear forces can cause mild instability. Chronic problems are related to repetitive motions and overuse, but acute and chronic injuries also occur.
Why does knee valgus occur?
Knee valgus is caused by a combination of movements of the femur and tibia, which can affect the proximal and distal joints of the knee, including the body, hip, and ankle. Lack of femoral control can lead to excessive adduction and internal rotation, which can strain the ACL.
What muscles are involved in knee valgus?
A common inaccurate movement pattern when squatting is knee flexion (knees bending inward). This is usually because the strong hip adductors (located on the inner thigh) overpower the weak hip abductors (gluteus minimus and gluteus medius).
What ligaments prevent valgus?
Both the medial collateral ligament (MCL) and the anterior cruciate ligament (ACL) have been reported to prevent luminal instability of the knee. This study investigated experimentally the anatomical mechanisms by which these connections prevent light instability.
Reference
Valgus Stress Test. (n.d.). Physiopedia. https://www.physio-pedia.com/Valgus_Stress_Test
Valgus Stress Test. (n.d.). The Student Physical Therapist. https://www.thestudentphysicaltherapist.com/valgus-stress-test1.html
Valgus stress test. In Wikipedia. https://en.wikipedia.org/wiki/Valgus_stress_test