Uterine Artery Embolization
Uterine artery embolization (UAE) is a minimally invasive procedure used in the treatment of various gynecological conditions, primarily uterine fibroids. Fibroids are benign tumors that grow in the uterus and can cause symptoms such as heavy menstrual bleeding, pelvic pain, and pressure symptoms.
Table of Contents
Introduction:
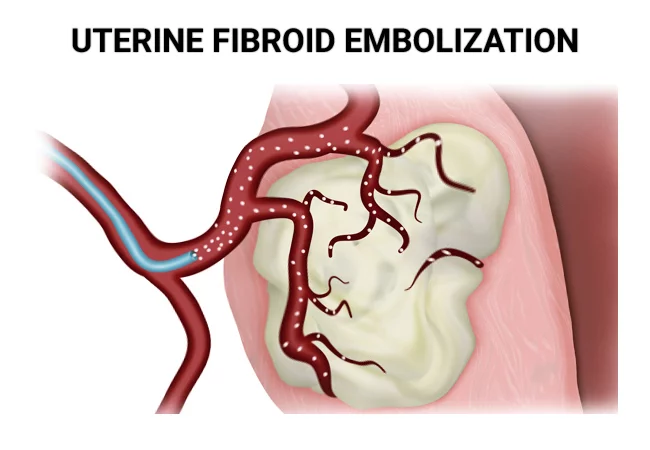
The most popular usage of uterine artery embolization, also known as “uterine fibroid embolization” or “UFE,” is an innovative outpatient procedure for the treatment of irritating fibroids. It can also be used to lessen the symptoms of adenomyosis. The uterus (womb) is the site of development for noncancerous, benign tumours called uterine fibroids.
The fibroids’ blood supply is severed during the operation. Usually, this results in the fibroids shrinking.
By using this minimally invasive treatment method, surgery is avoided while the uterus is preserved. A board-certified interventional radiologist performs this surgery using minimally invasive procedures, real-time fluoroscopy, and pre-operation MRI imaging to stop the fibroids’ blood supply, which causes them to shrink over time. Adenomyosis is caused by tissue displacement brought on by obstructed blood vessels.
The process of uterine artery embolization (UAE) is performed to stop vaginal bleeding. Many conditions, including childbirth, trauma, malignant tumours, and uterine fibroids, may have contributed to the bleeding. UAE functions by blocking off the uterus’s blood flow and is very minimally invasive.
What is Uterine Artery Embolization?
A minimally invasive technique called uterine artery embolization (UAE) is most frequently used to treat vaginal bleeding brought on by uterine fibroids, which are noncancerous tumors inside your uterus. UAE is effective not just in treating fibroids but also in severe bleeding. UAE can treat severe bleeding caused by postpartum hemorrhage, malignant (cancerous) gynecological tumors, and trauma in addition to fibroids.
Doctors usually use the treatment to treat fibroids. The uterine fibroid embolization procedure (UFE) is comparable.
Uterine fibroid embolization (UFE) and uterine artery embolization (UAE) are terminologies that are frequently used interchangeably. But they’re not the same. UFE is a specific type of UAE used to treat fibroids in the uterus. UAE treats a number of illnesses that might result in vaginal bleeding, including uterine fibroids. For weeks or months, fibroids gradually shrink and die due to the blockage of their blood supply.
During uterine artery embolization, a catheter is used by an interventional radiologist to insert tiny particles that obstruct the uterine body’s blood supply. The main reasons for the operation are to cure adenomyosis and uterine fibroids. It’s also commonly known as uterine fibrid embolization because uterine fibroids are the most frequent indication.
For women who want to keep their uterus, uterine artery embolization may be a better option than surgical therapy for fibroids such as a hysterectomy, which involves removing the uterus. Uterine arteriovenous malformations and postpartum bleeding are additional causes of uterine artery embolization.
Medical uses:
The most prevalent kind of benign uterine tumors are called uterine fibroids, and they are made of smooth muscle. They frequently result in bulk-related symptoms, such as abdominal bloating, back pain, and pelvic heaviness. Abnormal or heavy uterine bleeding caused by uterine fibroids, as well as uncomfortable bulk-related symptoms, can be treated with uterine artery embolization.
There are three possible indicators of a successful outcome: the size, quantity, and location of fibroids. According to research, fibroids that are submucosal—that is, just beneath the uterine lining—showed the most size reduction, whereas subserosal tumours—that is, outside the uterus—showed the least reduction.
Treatment for adenomyosis, a condition in which the uterine lining develops abnormally into the uterine muscle, may potentially involve uterine artery embolization. Painful menstrual cycles and heavy or extended menstrual flow are signs of adenomyosis.
In addition to controlling fibroids, uterine artery embolization can also be utilized to treat postpartum obstetrical haemorrhage or other severe uterine bleeding. Tamponade with a uterine balloon is a successful treatment option for many women who suffer from postpartum bleeding. However, uterine artery embolization can be a suitable choice if women are still bleeding.
Treatment of uterine arteriovenous malformations, which can result in abnormal or potentially fatal bleeding, is a less common reason for uterine artery embolization. The remaining women may develop the malformations as a result of surgical procedures or may have uterine malignancies; around half of the women with uterine arteriovenous malformations are born with them.
Who Makes the Best Candidate for Embolization of the Uterine Artery?
An efficient treatment for uterine artery embolization is the reduction of excruciating symptoms brought on by adenomyosis and fibroids. Uterine artery embolization has the following advantages:
- Symptom relief for adenomyosis or fibroid within three to six months
- Effective anemia treatment that does not require iron supplements or blood transfusions
- Protecting healthy tissue, such as the ovaries and uterus
- Short recovery period due to the procedure’s minimum invasiveness
- With this treatment, most fibroid sizes and locations can be addressed. Nevertheless, for the therapy to be effective, their fibroids are either too big or situated in an extremely difficult area of the uterus.
Candidates who fit this description the best for UAE are:
- Are premenopausal age
- Have heavy, regular periods, or experience dysmenorrhea, or pain during the menstrual cycle, as a result of fibroids
- Have no desire to become pregnant again.
- Anemia
- Heavy menstrual periods
- Pain in the abdomen or lower back
- Lower abdominal pressure or a sense of fullness
- Problems with urination and bowel movements
- Enlarged uterus and abdomen
- Issues with pregnancy and fertility
- Discomfort during intercourse
Additionally, doctors could recommend UAE to stop severe pelvic hemorrhage because of:
- Injuries
- Malignant gynecological tumors
- Bleeding following parturition (postpartum hemorrhage)
- Adenomyosis
- UAE may be suggested by medical professionals as a prophylactic strategy to stop bleeding during specific procedures.
- If a patient has tried other therapy to treat their problems or does not wish to get any more ones, they might suggest it.
Procedure of Uterine Artery Embolization (UAE)
Before to a UAE (uterine artery embolization)
Your physician will make a recommendation for the UAE following a complete assessment and medical history. They’ll run diagnostic testing to find out what’s causing your problems.
Several factors could occur prior to the operation, such as:
- A medical history, allergies, prescriptions, and menstruation history will all be reviewed by the doctor. You’ll talk about the goals for getting pregnant as well, as being in the UAE may interfere with getting pregnant.
- The doctor will use hysteroscopy, ultrasonography, or magnetic resonance imaging (MRI) to find the source of the bleeding in the lining of the uterus.
- To find out if you have cancer cells in your uterus, a biopsy (tissue sample) of the inner lining may be performed.
- Your healthcare physician may advise you to stop taking blood thinners, aspirin, and nonsteroidal anti-inflammatory medicines (NSAIDs) prior to UAE.
- Prior to the surgery, there is no allowed food or beverage intake. You and your clinician will talk through the specifics of fasting instructions.
- The night before your UAE treatment, after midnight, you should abstain from eating and drinking. It is not recommended to consume aspirin, Advil, Motrin, or ibuprofen five days before the surgery. These drugs may cause blood thinning. You may, however, take other prescriptions with a little sip of water the morning before the UAE surgery. That being said, please consult your doctor about when to stop taking any drugs you may be taking, such as Coumadin, Plavix, Lovenox, Glucophage, or Heparin.
Process of Uterine Artery Embolization:
Typically, uterine artery embolization (UAE) is an outpatient operation that doesn’t need to be a hospital stay. Usually, the entire process takes 90 minutes to complete.
UAE is typically carried out as follows:
Under conscious anaesthesia, an interventional radiologist performs the procedure. As you lie down on an examination table, devices that track your blood pressure and heart rate will be connected to you. Access is often gained through the groin or wrist via the femoral or radial arteries, respectively. In order to reduce the risk of infection, your groin area will be cleaned and shaved.
Sterile clothes will then be placed over you. The desired artery is punctured with a needle using the Seldinger technique after the skin surrounding it has been made anaesthetic. To make the skin surrounding your groin numb, an anesthetic (pain blocker) is applied. A catheter is then inserted into the artery and used to identify the uterine arteries for embolization under fluoroscopic supervision. After the embolizing agent (spheres or beads, which are usually formed of plastic or gelatin) is released, a contrast-enhanced angiography is carried out to verify the catheter’s position at the level of the uterine artery.
Blood flow will considerably slow down as more embolizing agents are used. The fibroid shrinks over time as a result of the reduced blood supply. The catheter is taken out once it’s done. After the catheter is taken out, this region is compressed for around fifteen minutes. After stopping any bleeding from the puncture site, a bandage is put on. Due to the high failure rate of unilateral UAEs, both the left and right uterine arteries have been embolized. A hospital or surgery center may be a location for the procedure.
Although acceptance for UAE as an outpatient operation has grown recently, many physicians still prefer an overnight hospital stay for pain management. The procedure’s follow-up may vary depending on the institution, although it may involve a clinic visit one to three months after the procedure and also an MRI to see if any fibroids have shrunk from preoperative MRI.
Following the Procedure:
- You might spend the night in the hospital. You could even return home that same day.
- Painkillers will be given to you. After the treatment, you will be told to lie flat for four to six hours.
- Observe any additional guidelines on self-care once you return home.
- The first 24 hours following the treatment are often characterized by moderate to severe cramping in the abdomen and pelvis.
- Most women heal fast, going back to their regular activities in seven to ten days. It’s possible for some of the treated fibroid tissue to occasionally flow into your vagina.
- They could continue for two weeks or a few days. Severe cramps have the potential to last for over six hours at a time.
- Most women heal fast, going back to their regular activities in seven to ten days. It’s possible for some of the treated fibroid tissue to occasionally flow into your vagina.
Benefits of Uterine Artery Embolization
About 90% of patients with fibroids who receive UAE treatment report either complete or partial symptom improvement. Additional benefits of the UAE are as follows:
- It can be done as an outpatient surgery while under local anesthetic.
- Little recovery period due to the lack of major sutures or incisions.
- Minimal bleeding or blood loss afterward.
- The complication rate is lower than with invasive operations.
- It circumvents the negative effects of hormone treatments, which are occasionally employed to treat fibroids.
- It is less invasive than other treatments like myomectomy, which removes uterine fibroids surgically, and hysterectomy, which removes your uterus because it just requires a minor puncture.
Indications of Uterine Artery Embolization
The indications for this operation are as follows:
Strong Indications for Gynecology
- Less than 7-centimeter uterine intramural fibroids, which grow within the uterine muscle layer, are particularly common in women who want not to have surgery or who are medically unfit for surgery because of their excessive obesity.
- Heavy bleeding during the menstrual cycle
- Symptoms of lower abdominal and pelvic pain and pressure, including bloating, increased frequency of urination, constipation, and needing to wake up in the middle of the night to go to the bathroom
- Dysmenorrhea
Gynecological Indications: Less Strong
- Hydronephrosis combined with obstruction of the bladder outflow
- Unusual bleeding in the uterus
- Uterine artery pseudoaneurysms
- The proliferation of the endometrium into the myometrial layer causes adenomyosis, or generalized swelling, in the mass of the uterus. It can result in abnormal uterine bleeding and pain, and it affects up to one-fifth of women. Adenomyosis, which is often treated with a hysterectomy, can also be effectively managed in UAE, particularly in younger women who wish to delay pregnancy or in patients who are anaemic and need assistance in restoring their haemoglobin levels before surgery. Over 98% of cases with UAE for this indication result in success.
- Fetal arteriovenous malformations (AVMs) resulting from uterine curettage, trauma, or congenital abnormalities in the uterine capillary development throughout fetal development. Arteriograms, which have supplanted hysteroscopy, Doppler ultrasonography, and MRI imaging, are used to diagnose these. UAE is currently the recommended therapy for patients with AVMs; this is especially true if the patient hopes to become pregnant after the procedure. Previously, these were treated with a hysterectomy.
- To address contrast extravasation that occurs during angiogram due to another reason
- Fibroid-related infertility without another apparent reason or when alternative treatment options are not appropriate
- Ectopic pregnancies can happen in the uterus or outside the uterus and are fatal. UAE is used to treat interstitial, cervical, abdominal, and scar ectopic pregnancies; surgical removal is the standard of care for tubal and ovarian pregnancies. These are particularly helpful because, in many circumstances, they save the need for surgery, and if methotrexate is not acting as intended, they stop the ectopic sac from bleeding excessively. Furthermore, preventive UAE can lessen bleeding from the highly vascularized implantation site after the removal of an abdominal pregnancy.
- Child Birth-Related Factors
- Uterine atony resulting in bleeding after delivery
- Bleeding inside the uterus as a result of birth trauma (such as cervical lacerations and vaginal hematomas)
- Persistent bleeding following childbirth following a hysterectomy or uterine artery closure
- Deep placental invasion into the myometrium as opposed to the endometrium, or placenta accreta, may help prevent the need for a hysterectomy after childbirth.
- In all of these situations, the treatment has an 80% success rate when performed by skilled doctors; however, the patient should be moved as soon as possible to prevent needless delays brought on by hurried decisions. Either one or both uterine arteries are embolized, and its safety is also confirmed.
Contraindication:
The following is how patients posted for the UAE should be evaluated:
- Normal report on Pap smear obtained no more than a year ago
- Pregnancy test results are negative
- Not a single urinary tract infection or reproductive tract irritation
- Normal levels of creatinine and urea in the kidneys
- Typical blood examinations
- Normal amounts of thyroid hormone
- Normal amounts of C-reactive protein
Relative contraindication:
When there are other options, it is not always advised to use the UAE for certain patients. Among these relative contraindications are:
- Having taken gonadotropin-releasing hormone during the last three months due to the elevated risk of uterine artery spasm (ulipristat acetate does not induce this).
- A submucosal or subserosal pedunculated fibroid could become a possible source of infection if it loses its pedicle due to infarction and lies freely inside the uterus or general abdominal cavity.
- Fibroids whose ovarian artery serves as their main source of blood
- History of adhesions after pelvic surgery
- Fibroids more than 10 cm, or many fibroids combined with uteri larger than what would be expected from a 20-week pregnancy, as UAE will not effectively reduce the size in these situations.
Absolute Contraindications:
There are several circumstances in which the UAE should never be performed:
- Hypersensitivity to the angiography contrast agent
- Malignancy
- Irreversible coagulation problems
- Being pregnant
- Urinary tract or reproductive tract infections or inflammation
- History of radiation to the pelvis
- Overactive thyroid
- Failure of the kidneys
- Women who are unwilling to face the about 3-20% chance of failure and the consequent, unavoidable need for a hysterectomy as a result of unbearable pelvic pain or infection following UAE
Risks of Uterine Artery Embolization
In general, the UAE is secure. But there are risks involved, just like with any other operation. General surgical risks include the following:
- Bleeding
- Response to anaesthesia or medication
- Infection
- Bruises
- Experts deem the process to be both safe and efficient.
Risks specific to the UAE include:
- Damage to the artery or uterus
Infection at the puncture site or uterus - Infection: The catheter’s insertion may result in an infection or harm to nearby blood vessels.
- Blood clot
- Early menopause
- Infertility: Being infertile means that you are unable to conceive
- Delayed identification of rare cancer
- Inadequate blood supply to the leg or buttock
- Premature ovarian failure
- Problems of pregnancy with pulmonary embolism
- Damage to healthy tissue: If the embolic agent is placed in the incorrect blood vessel, it may obstruct the healthy tissue’s blood flow.
- Allergy: A reaction to sedative drugs or X-ray contrast dyes may manifest as an allergy.
- Absence of menstruation: After uterine artery embolization, menstrual periods will stop for good in 1% to 5% of cases.
- An failed surgical procedure It may be necessary to have another UAE or hysterectomy if your symptoms reappear.
Complications
The incidence of severe side effects is similar to that following a hysterectomy or myomectomy. A higher rate of mild problems and a higher chance of needing surgical intervention two to five years after the initial treatment outweigh the benefit of a somewhat faster healing period.
According to an analysis of 15,000 women, those who underwent uterine artery embolization needed more hysterectomies and other treatments to address fibroids during the following five years than those who received myomectomy.
Among the complications are the following:
- A pulmonary embolism or sepsis—the presence of pus-forming or other pathogenic organisms, or their toxins—in the blood or tissues can result in multiple organ failure and, in extreme cases, death. The duration of immobility that patients experience after the surgery is thought to be the cause of a pulmonary embolism since it increases the risk of deep vein thrombosis formation and subsequent pulmonary embolism.
- Infection originating from fibroids’ tissue loss, which causes endometritis (uterine infection) and necessitates a protracted hospital stay for IV antibiotics
- Fibroid expulsion( the pushing out of fibroids through the vagina): This can happen in a variety of ways, depending on where in the uterine tissue the fibroid is located. When it does happen, it usually happens around three months after treatment.
- Post-embolization syndrome: this condition is marked by fevers, malaise, nausea, vomiting, and severe night sweats; it can also cause a foul vaginal odor due to necrotic tissue that has been infected and persists inside the uterus; it can also result in hysterectomy due to embolization failure, infection, or discomfort.
- Misembolization is caused by microspheres or polyvinyl alcohol particles that flow or drift into organs or tissues that are not supposed to be there, harming other organs or body parts like the rectum, bladder, ovaries, and, infrequently, the small intestine, uterus, vagina, and labia.
- Failure: fibroid growth persisted, and it grew again in four months.
- Iatrogenic, abnormal cessation of menstruation, and raised levels of follicle-stimulating hormones to menopausal levels are known as menopause.
- Hematoma, blood clot at the site of the incision, pus, and blood-filled vaginal discharge; bleeding from the site of the incision; bleeding from the vagina, potentially fatal allergic reaction to the contrast agent.
What to expect while recovering?
There is no need for a hospital stay for uterine artery embolization; it is an outpatient surgery. After the procedure, you can usually leave the hospital a few hours later, resume work and light activity a few days later, and recover completely in two weeks. Medication is recommended to you in an effort to reduce swelling and pain.
You will need to lie flat in bed for six hours following the treatment, with the leg where the catheter was inserted straight. Patients vary in how much pain they suffer. Usually, the worst discomfort happens right after the treatment and throughout the next six hours. Menstrual cramps are like this discomfort, according to patients. Certain individuals claim not to be in any pain.
Watery or mucusy vaginal discharge is usual for several weeks following the operation. A few days following the therapy, a small percentage of patients develop post-embolization syndrome, which includes low-grade fever, nausea, discomfort, fatigue, and vomiting.
Most patients see relief from fibroid or adenomyosis symptoms three months following the treatment, and menstruation usually returns to normal.
Recovery issues to keep an eye on: Give your doctor a call if, days after the treatment, you are still experiencing post-embolization syndrome.
To guarantee a speedy recovery, you must follow these guidelines as soon as you get home:
- When you get home, drink eight glasses of liquid—coffee, juice, or water. You can resume your regular diet as soon as you get out of the hospital.
- For 48 hours, abstain from hard labour-intensive tasks like housework and yard work. In a week, the majority of patients can resume their regular activities.
- Drive a car for a full day after that.
- For five days, avoid taking a hot bath. You can take a shower.
Inform the Interventional Radiology office if any of the following take place:
- Bleeding at the point of entrance.
- Any unexpected discomfort in the leg where the catheter was inserted or at the entry site.
- Any variation in the leg’s colour or warmth. It’s normal to get a tiny bruise.
Summary
Uterine fibroids are among the disorders that doctors treat in UAE when they produce severe pelvic bleeding. It is a less invasive process that could be used in place of more invasive ones like surgery.
UAE is generally effective and safe, with little chance of side effects. Still, the process isn’t for everyone. Individuals who are thinking about getting pregnant in the future can decide not to have this operation done because it could make getting pregnant less likely.
UAE is generally useful in reducing fibroids’ associated pain, bleeding, and pressure.
Patients who undergo the procedure report a reduction in symptoms of up to 90%. Over 90% of cases of abnormal uterine bleeding end in resolution. After five years, about 10% of people will require another surgery.
Treatment may occasionally fail to reduce the size of the fibroids or alleviate the patient’s symptoms. In some cases, problems during the operation may necessitate emergency surgery. For instance, 1 in 100 occurrences involves artery perforation, which may necessitate immediate medical attention.
The likelihood that symptoms may recur and eventually necessitate surgery increases with age.
According to a 2021 study, the UAE has an 80% success rate in curing adenomyosis after 52 months. In comparison to a hysterectomy, it is also a less invasive procedure.
FAQs
Do fibroids shrink after embolization?
Fetal fibroids by blocking the fibroids’ blood supply, and embolization causes them to shrink. The sand-like particles that the doctor injects into the arteries supplying the fibroids are tiny. This results in the formation of a clot that cuts off the blood supply.
Is uterine embolization painful?
Pain: It’s common to feel like you’re having a severe menstrual period for a few days following the treatment, with cramps in your abdomen. Narcotic painkillers like Vicodin or Percocet should alleviate symptoms, and heated pads are beneficial for many women.
What makes embolization better to a hysterectomy?
Uterine artery embolization is linked to a shorter hospital stay and an earlier return to normal activities in comparison to hysterectomy, but it also has a higher risk of the requirement for follow-up procedures.
What is the uterine embolization success rate?
With an approximate success rate of 85%, uterine fibroid embolization is a fairly successful operation. The majority of patients have a significant improvement in their symptoms as well as a reduction in the size of their uterine fibroids after the operation.
How safe is embolization of the uterus?
The uterus’s blood flow is briefly interrupted during embolization. This indicates that the chance of the uterus becoming injured and incapable of healing is quite low. After embolization, dead fibroid tissue may also get infected, though this is extremely rare.
Reference
- Uterine Artery Embolization: Indications and Contraindications. (2022, October 11). News-Medical. https://www.news-medical.net/health/Uterine-Artery-Embolization-Indications-and-Contraindications.aspx
- Tee-Melegrito, R. A. (2022, June 29). What is uterine artery embolization? https://www.medicalnewstoday.com/articles/uterine-artery-embolization#summary
- Uterine Fibroid Embolization. (n.d.). Fibroid Treatment Collaborative. https://www.fibroid.com/treatments/uterine-fibroid-embolization/
- Uterine Artery Embolization | Patient Care. (n.d.). Weill Cornell Medicine. https://weillcornell.org/services/obstetrics-and-gynecology/fibroid-and-adenomyosis-program/our-services/uterine-artery-embolization
- Uterine Artery Embolization. (2020, October 7). ucsfhealth.org. https://www.ucsfhealth.org/treatments/uterine-artery-embolization
- Uterine artery embolization. (2023, November 28). Wikipedia. https://en.wikipedia.org/wiki/Uterine_artery_embolization
- Professional, C. C. M. (n.d.). Uterine Artery Embolization. Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/17954-uterine-artery-embolization
- Uterine Artery Embolization. (2023, November 28). Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/uterine-artery-embolization