
Popliteal Artery
Table of Contents
Introduction
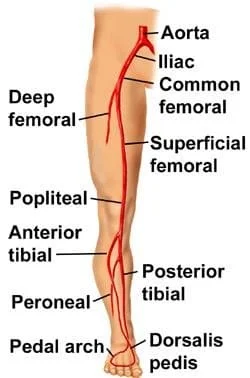
In the distal part of the adductor magnus muscle, the popliteal artery is a deeply situated continuation of the femoral artery opening. It passes through the popliteal fossa before dividing into the anterior and posterior tibial arteries at the popliteus muscle’s bottom border.
The popliteal artery, which crosses the intercondylar fossa, is the deepest (most anterior) structure in the fossa. It passes next to the knee’s joint capsule. The knee joint’s capsule and ligaments are supplied by five genicular branches of the popliteal artery. The superior lateral, superior medial, middle, inferior lateral, and inferior medial genicular arteries are the genicular arteries.
They take part in the formation of the periarticular genicular anastomosis, which is a network of vessels that surrounds the knee and supplies collateral circulation, preventing the popliteal artery from kinking, and sustaining blood flow to the leg during full knee flexion.
What is the Popliteal Artery?
Your legs’ femoral arteries extend into your popliteal arteries. To supply blood to the lower limbs, they begin in the middle of your thighs and travel behind your knees. By resting your fingers on the back of your knee above the popliteal artery, you or a medical professional can feel your popliteal pulse.
The femoral artery continues into the popliteal artery. From the femoral triangle, the femoral artery descends, travels medially over the anterior thigh, and then crosses the adductor hiatus to become the popliteal artery. The widest and most distal gap in the adductor magnus connection along the femoral shaft is known as the adductor hiatus.
The popliteal artery passes through the popliteal fossa and is the femoral artery’s continuation. It begins at the intersection of the middle and lower thirds of the thigh at the Adductor Magnus opening, travels downward and laterally to the femur’s intercondyloid fossa, and then moves downwards vertically to the lower border of the popliteus, where it splits into the anterior and posterior tibial arteries.
The popliteal artery, which arises from the femoral artery in the inner thigh, crosses the popliteal fossa, or the space behind the knee joint, and then divides into the anterior and posterior tibial arteries. It supplies most of the major muscle groups in the legs, including the knee joint, with blood through its numerous branches.
Anatomy of the Popliteal Artery
There are two popliteal arteries in your body: one on the left and one on the right. The femoral arteries, which are the big blood veins that supply blood to your legs, continue into these arteries.
In the distal region of the adductor magnus muscle, the popliteal artery is a deeply situated continuation of the femoral artery opening. It passes through the popliteal fossa before dividing into the anterior and posterior tibial arteries at the popliteus muscle’s lower border.
The popliteal artery, which crosses the intercondylar fossa, is the deepest (most anterior) structure in the fossa. It passes next to the knee’s joint capsule. The knee joint’s capsule and ligaments are supplied by five genicular branches of the popliteal artery. The superior lateral, superior medial, middle, inferior lateral, and inferior medial genicular arteries are the genicular arteries.
The arteries divide into the tibioperoneal (or tibiofibular) trunk and the anterior tibial artery below the knee joint. Smaller branches that emerge from this stem deliver blood to your fibula and the back of your calf.
The popliteal artery may bend as a result of their involvement in the formation of the periarticular genicular anastomosis, a network of vessels encircling the knee that provides collateral circulation capable of sustaining blood flow to the leg during full knee flexion.
Your legs’ femoral arteries split off to form the popliteal arteries, which supply blood to your lower limbs and knees. The popliteal pulse, which runs behind your kneecap, is where they are located. Atherosclerosis, aneurysms, and blood clots are a few conditions that can damage an artery, increasing the chance of limb loss and producing intermittent claudication, or leg pain.
All of these branches from the popliteal artery eventually supply blood to your foot after passing through your lower leg or calves.
Structure of the Popliteal Artery
The femoral artery continues as the popliteal artery. It emerges from the popliteal fossa beneath the soleus muscle’s fibrous arch.
Relationships:
- Anteriorly: The popliteus muscle, the knee joint, and the popliteal surface of the femur.
- Posteriorly: Skin, fascia, tibial nerve, and popliteal vein.
- Laterally: Plantaris, the lateral gastrocnemius in the lower section, the biceps femoris, and the lateral condyle of the femur in the upper part.
- Medially: The tibial nerve, popliteal vein, and medial head of the gastrocnemius in the lower section, and the semimembranosus and the medial condyle of the femur in the upper part.
Course of the Popliteal Artery
The popliteal artery is the femoral artery’s continuation, starting in the adductor hiatus of the thigh’s adductor magnus muscle. Since adipose tissue surrounds it, it is largely locked in place within the popliteal fossa. It lies deep in the gastrocnemius muscle and is attached distally by the soleus muscle’s fascia.
It moves downward further and crosses the popliteal fossa, which is behind the knee joint. The popliteal artery goes between the popliteal and gastrocnemius muscles in the posterior compartment of the leg after passing obliquely via the popliteal fossa.
After going through the tendinous arch between the two heads of the gastrocnemius and into the deep portion of the posterior compartment of the leg, it instantly divides into the anterior and posterior tibial arteries. The popliteal artery, which runs next to the knee capsule, is the popliteal fossa’s deepest arterial structure.
Although it is only a little artery, it supplies the majority of blood to the muscles in the lower legs, the knee ligaments, and the knee joint.
The popliteus muscle may be closest to the popliteal artery’s terminal bifurcation. Three arteries branch off from the popliteal artery: the anterior, posterior, and fibular arteries in about 6% of people.
Function of the Popliteal Artery
The human body’s circulatory system includes the popliteal arteries. These are the arteries in the periphery.
As the main blood supply to the knee’s bones and tendons, the main function of this artery is to transport blood to those tissues. Furthermore, it provides the gastrocnemius, soleus, and popliteus muscles, which are key hamstring and calf muscle groups.
In medical practice, the patient can feel the pulse of the deep-seated popliteal fossa by having them lie down and lift their flexed knee while keeping other muscles relaxed. If this pulse is absent or very faint, femoral artery blockage may be the cause.
Peripheral arteries circulate blood to bodily parts that are distant from the heart.
Blood is supplied to the popliteal arteries by the following:
- Fibulas (The tiny bones on the outside of the lower legs)
- Knee pits (popliteal fossa) and knee joints.
- Nerves and muscles of the lower leg.
- Tibias (larger bones on the inner of the lower legs)
- Ankles and feet.
Branches of the Popliteal Artery
The main source of blood supply to the knee joint is the popliteal artery.
Five genicular branches from the popliteal artery go toward the periarticular genicular anastomosis, which supplies the ligaments and knee joint capsule.
The branches of the popliteal artery from proximal to distal are the following:
- Superior medial and lateral genicular arteries
- Medial and lateral sural arteries
- Middle genicular artery
- Inferior lateral genicular artery
- Inferior medial genicular artery
- Muscular artery
- Anterior and posterior tibial arteries split off at the terminal.
- Superior lateral and medial genicular arteries: The popliteal artery gives rise to the superior lateral and medial genicular arteries, which then curve around the corresponding femoral condyles to supply the femoral condyle bone, the surrounding knee joint synovium, and the superior portion of the patella.
- Middle genicular artery: Behind the distal femoral intercondylar region, the single, smaller middle genicular artery divides off from the popliteal artery and travels anteriorly, piercing the posterior portion of the knee joint capsule. It provides the posterior portions of the menisci, the posterior cruciate ligament, and the posterior portion of the anterior cruciate ligament.
- Inferior lateral and medial genicular arteries: The popliteal artery branches off into the inferior lateral and medial genicular arteries, which go around the tibial condyles and deep into the knee’s collateral ligaments. The anterior portion of the anterior cruciate ligament, the inferior region of the patella, the collateral ligaments and tendons, and the knee joint capsule are all supplied by these arteries.
- Muscular branch: The popliteal artery’s primary function is to give blood to the muscles located in and around the lower leg, knee, and thigh. Numerous muscle branches of the popliteal artery deliver blood to the plantaris, gastrocnemius, hamstring, and soleus muscles. The deep femoral and gluteal arteries of the thigh anastomose with the superior muscle branches of the popliteal artery.
- Sural arteries: Large blood vessels called the sural arteries emerge on either side of the popliteal artery, supplying the soleus and plantaris muscles with blood flow. The medial and lateral heads of the gastrocnemius muscle, which are among the superficial muscles of the posterior leg, receive some of their supply from the sural branches. Extra cutaneous branches, sometimes referred to as sural cutaneous branches, help nourish the superficial fascia and skin in the surrounding areas.
- Tibial arteries: The anterior and posterior tibial arteries divides out from the popliteal artery near the inferior border of the popliteus muscle.
Anatomical Variations
There could occasionally be differences in the popliteal artery’s structure. The top three are as follows:
- Higher Origin of Tibial Artery: The popliteal posterior and anterior tibial arteries’ terminal branches might occasionally start higher than normal.
- Trifurcation: This occurs when the popliteal artery divides into the anterior and posterior tibial arteries, which supply blood to the front and back of the lower legs, respectively, and the peroneal artery.
- Hypoplastic/Aplastic Posterior Tibial Artery: This is an uncommon condition when the tibial artery at the popliteal artery’s end does not fully mature.
Supplies Structures:
The genicular anastomosis that supplies the knee joint is formed by the five genicular arteries that arise from the popliteal artery and receive additional arterial contributions from the descending genicular artery, the anterior tibial recurrent artery, and the descending branch of the femoral circumflex artery.
The proximal and distal regions of the posterior leg’s superficial muscles and the posterior thigh’s distal muscles are supplied in part by the muscular branches and sural arteries. Additionally, the skin around the knee joint is supplied by cutaneous veins.
Clinical Importance:
- Popliteal pulse: It could be challenging to feel the popliteal pulse due to the deep location of the popliteal artery. The most typical way to palpate this pulse is to have the patient lie down on their side with their knee bent to release the hamstrings and popliteal fascia. The area of the fossa where the popliteal artery and tibia are connected is where the pulsations are most noticeable. At the inferior side of the popliteal fossa, one may then feel the popliteal artery pulsing. This is crucial because a weak or nonexistent popliteal pulse could indicate vascular impairment and femoral artery blockage.
- Popliteal aneurysm: Edema and pain in the popliteal fossa are typically the result of a popliteal aneurysm, which is an abnormal dilatation of all or part of the popliteal artery. A stethoscope can be used to identify aberrant artery sounds (bruits) and palpable pulsations (thrills) that help differentiate a popliteal aneurysm from other masses. The tibial nerve is deeply connected to the artery, which means that an aneurysm could compress or extend the nerve’s blood supply (see vasa vasorum).
- In this situation, the skin covering the medial aspect of the calf, ankle, or foot is the typical site of pain transferred from such nerve compression. Due to the artery’s close proximity to the femur’s popliteal surface and the joint capsule, injuries such as distal femur fractures or dislocations of the knee may cause the artery to burst, causing bleeding.
- Moreover, an arteriovenous fistula (communication between an artery and a vein) may arise from a lesion due to their close proximity and confinement within the fossa. Leg and foot loss could ensue if these incidents are not recognized and treated quickly. Blood can go through the genicular anastomosis and avoid the blockage to reach the popliteal artery distal to the ligation if the femoral artery needs to be clamped.
After abdominal aortic aneurysms, popliteal aneurysms are the second most common form of aneurysm. People who are born with a masculine gender designation typically develop popliteal aneurysms.
- Popliteal artery haemorrhage: While it is rare, dislocation of the knee can happen as a result of a strong force being applied to the joint or from severe, high-energy trauma. Because the popliteal artery is so close to the joint, there is a significant risk of injury following a dislocation of the knee.
- A dislocated knee can stretch the popliteal artery, perhaps leading to a contusion, tear, rupture, or breakage. Damage to the calf muscles and popliteal vein may result from this. Limb loss may result from this if treatment is not received.
- Popliteal artery entrapment syndrome: PAES is a condition when the popliteal arteries are compressed by the knee region’s muscles and tendons. The popliteal artery passes between the two heads of the leg’s gastrocnemius muscle. It makes your calves hurt and cramp when you walk or engage in other strenuous activities.
- We refer to this as intermittent claudication. Any deviation from the norm in this area may result in intermittent claudication, which is pain during muscular contraction caused by insufficient blood flow. This causes the popliteal artery to be repeatedly injured, which increases the risk of arterial thrombosis, thromboembolism, and aneurysm formation. Athletes are most commonly affected by PAES, particularly men under 30.
The cause of the popliteal artery compression can be utilized to categorize cases of popliteal artery entrapment syndrome. Types 2 and 3 are caused by an aberrant insertion of the medial head of the gastrocnemius muscle, whereas types 1 and 4 are caused by anomalies in the popliteal artery.
Type 5 involves the trapping of the popliteal vein and popliteal artery, while type 6 is popliteal artery compression that occurs when a leg moves but does not result from anatomic abnormalities. The surgical release of the popliteal artery is achieved with a myotomy, or muscle excision, of the medial or lateral head of the gastrocnemius.
- Cystic adventitial disease: This medical condition arises when a cyst develops within the wall of the popliteal artery, thereby diminishing blood flow. People may develop popliteal artery stenosis or narrower arteries over time. Males assigned to this gender at birth are primarily affected. The symptoms include pain in the lower legs that gradually worsens when walking or exercising; these are known as intermittent claudication symptoms.
- Popliteal artery atherosclerotic disease: Blood clots and plaque can narrow the arteries, causing partial or whole blockages (occlusions). A higher chance of gangrene and limb loss exists. Similar to other forms of occlusive peripheral artery disease, the most common causes are high cholesterol, diabetes, smoking or using tobacco products, and people over 65.
- Popliteal cysts: These can be seen on ultrasonography and are highly prevalent. This fluid-filled mass that arises on the back of your knee is also known as a Baker’s cyst. It may result in oedema and pain. The cyst could restrict your knee’s range of motion and bending. Baker’s cysts are brought on by damage to the knee joint, such as arthritis or a torn meniscus. A popliteal cyst usually has little effect on the popliteal artery’s ability to function, even though they are both located behind your knee.
Risk factors for popliteal artery disease:
Among the risk factors for disorders of the popliteal artery are:
- Coronary artery disease.
- Diabetes.
- High blood pressure.
- High cholesterol.
- Male sex.
- Having obesity.
- Smoking or using tobacco products.
What are the signs of popliteal artery disease?
Leg discomfort or heaviness during walking or physical activity is a common symptom of popliteal artery disorders. When you rest, the heaviness, cramps, and agony go away. Intermittent claudication is the medical term used to describe this condition.
You might additionally experience:
- Lower leg swelling, or edema.
- Foot ulcers that don’t heal (sores).
- Pain in your foot, kneecap, or calf.
How are disorders of the popliteal arteries diagnosed?
To identify issues related to the popliteal artery, your healthcare professional may use the following tests:
- Ankle-brachial index (ABI) is calculated by pulse volume recordings (PVR) using Doppler and blood pressure to evaluate the arterial blood flow in your legs.
- Vascular ultrasonography evaluates your legs’ blood flow.
- An angiography, such as a CT or MRA scan, looks for signs of impaired blood flow in your lower extremities. The popliteal artery can be assessed with catheter angiography. This is an invasive test that is usually saved for unique situations that require further imaging.
What are popliteal artery disorders commonly treated with?
Depending on the disease, different popliteal artery illnesses require different treatments. Among them are:
- Drugs that prevent blood clots and decrease cholesterol and blood pressure.
- With catheter angioplasty and stenting, a constricted artery is opened using a balloon device, and the artery is kept open by placing a stent (a mesh device) inside.
- Bypass grafting involves rerouting a blocked artery so blood can travel through a newly formed blood vessel.
- Cyst removal surgery or muscle and tendon release to relieve tension on the popliteal artery.
Summary
Following its passage through the adductor hiatus of the adductor magnus muscle, the superficial femoral artery continues as the popliteal artery. It then travels posteriorly to the knee and anteriorly to the popliteal vein, which is its accompanying vein, until it bifurcates into the anterior tibial artery and the common trunk of the posterior tibial and peroneal arteries.
The main arterial supply in the knee and lower leg regions is the popliteal artery, which is located in the popliteal fossa. Several tributaries supply blood to the popliteal vein, which is located posterior to the popliteal artery. In addition, the popliteal artery supplies blood directly to many muscles, such as the plantaris, soleus, gastrocnemius, and distal parts of the hamstring. Popliteal artery damage can result in several conditions in the body.
FAQs
What is the popliteal artery used for?
Numerous branches of the popliteal artery give blood to the knee and lower extremity tissues. The superior medial and superior lateral genicular arteries begin above the knee joint and link to the deep femoral artery to supply collateral blood flow close to the knee.
Where is the pulse of the popliteal artery?
Your popliteal artery is the source of the popliteal pulse’s name. The blood flow from your leg to your foot is facilitated by this essential blood route. This means that your popliteal pulse is behind your knee. By doing this, the artery in the soft tissue is kept from the bones and tendons.
Which popliteal artery branch is the major branch?
The popliteal artery divides into the anterior and posterior tibial arteries, which are its two terminal branches, at the lower margin of the popliteus muscle after passing through the popliteal fossa.
Which nerve does the popliteal artery accompany?
The popliteal artery, popliteal vein, and tibial nerve are located inside the fossa. The tibial nerve, popliteal vein, and popliteal artery are the structures that are present in the following order, from medial to laterally.
What are the popliteal artery’s three branches?
Three branches of the popliteal artery are the anterior tibial artery, posterior tibial artery, and sural artery.
Reference
- Bowers, Z., Nassereddin, A., Sinkler, M. A., & Bordoni, B. (2023, July 24). Anatomy, Lower Limb and Bony pelvis: Popliteal Artery. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK537125/
- Gurarie, M. (2022, March 25). The Anatomy of the Popliteal Artery. Verywell Health. https://www.verywellhealth.com/popliteal-artery-anatomy-4687681
- Micheau, A., & Hoa, D. (2024, February 8). Popliteal artery. e-Anatomy – IMAIOS. https://www.imaios.com/en/e-anatomy/anatomical-structure/popliteal-artery-1553674040
- Popliteal Artery | Complete Anatomy. (n.d.). www.elsevier.com. https://www.elsevier.com/resources/anatomy/cardiovascular-system/arteries/popliteal-artery/19258
- Professional, C. C. M. (n.d.). Popliteal Artery. Cleveland Clinic. https://my.clevelandclinic.org/health/body/22708-popliteal-artery
- Popliteal artery. (2023, July 19). Kenhub. https://www.kenhub.com/en/library/anatomy/popliteal-artery
- Popliteal artery. (2023, March 5). Wikipedia. https://en.wikipedia.org/wiki/Popliteal_artery



4 Comments