

Sternum bone
Table of Contents
Introduction
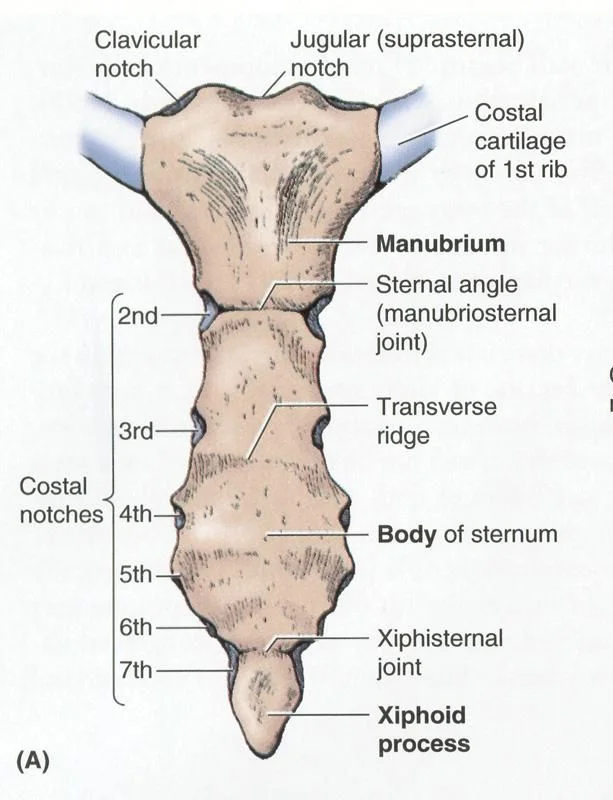
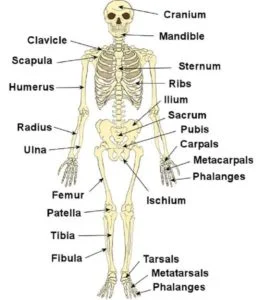
The sternum is the centrally located anterior portion of the chest wall and is a partially T-shaped vertical bone. There are three anatomical divisions in the sternum: the manubrium, body, and xiphoid process. The anterior rib cage’s costal cartilage connects the sternum to the ribs.
The xiphoid process is the narrower distal segment that creates the partial T-shape, while the manubrium is the broad superior segment of the body. The sternum is a significant bony structure that is of surgical significance due to its anatomical position and variations. This article also discusses the sternum’s clinical significance, in addition to its anatomy.
Structure of Sternum
The narrow, flat bone known as the sternum is located in the middle of the front of the chest. The clavicles (collarbones) are supported by the top of the sternum, and its edges join the costal cartilages of the first two pairs of ribs. The inward surface of the sternum is likewise the connection of the sternopericardial tendons. Additionally, the sternocleidomastoid muscle is connected to its top. The sternum comprises three principal parts.
Manubrium
Body (gladiolus)
Xiphoid process
The sternum is naturally angled forward, downward, and obliquely. It has a slightly arched front and a curved back; broad above, in the shape of a “T,” narrows where the manubrium joins the body, narrows again below the middle of the body, and narrows again to the lower extremity. The male sternum is typically about 1.7 cm longer than the female sternum in adults.
Manubrium
The broad upper portion of the sternum is called the manubrium (Latin for “handle”). It has four borders thanks to its quadrangular shape that narrows at the top. At the manubrium’s upper broadest point, the suprasternal notch, also known as the jugular notch, can be found in the middle. A notch can be felt between the two clavicles. The right and left clavicular notches are located on either side of this notch.
The manubrium joins the sternum’s body, the clavicle, and the first pair of ribs’ cartilage. The substandard line, oval and unpleasant, is covered with a flimsy layer of ligament for verbalization with the body. The horizontal lines are each obvious above by a downturn for the main coastal ligament, and underneath by a little feature, which, with a comparative aspect on the upper point of the body, shapes a score for the gathering of the coastal ligament of the subsequent rib. There is a narrow, curved edge that slopes downward toward the middle between the depression for the first costal cartilage and the demi-facet for the second. Additionally, the pericardium is joined to the manubrium’s posterior side by the superior sternopericardial ligament.
Body of Sternum Bone
The body, or gladiolus, is the sternal part that is the longest. It is thought to only have a front and back surface because it is flat. Three transverse ridges cross the bone in front of the third, fourth, and fifth articular depressions to define its flat front and upward and forward orientation. The pectoralis significant appends to it on one or the other side. An orifice of varying size and shape can occasionally be seen at the point where the third and fourth parts of the body meet. This is the sternal foramen. Three transverse lines, though less distinct than those on the front, also mark the slightly concave posterior surface; The transverse thoracic begins on either side of its lower part.
The body meets the manubrium at the location of the sternal angle. At the point where the sternum projects the most forward, the sternal angle can be felt. Notwithstanding, in certain individuals, the sternal point is curved or adjusted. The sternal angle is a useful landmark during physical examinations because this is where the second rib attaches.
Each external line, at its predominant point, has a little feature, which with a comparable feature on the manubrium, shapes a depression for the ligament of the subsequent rib; underneath this are four rakish discouragements that get the ligaments of the third, fourth, fifth, and 6th ribs. A small facet on the inferior angle joins a similar one on the xiphoid process to form a notch for the seventh rib’s cartilage. These particular discouragements are isolated by a progression of bent interarticular spans, which lessen long from above descending, and compare to the intercostal spaces. The sternum and the majority of the true ribs’ cartilages articulate at the points where their basic component segments meet. This is clearly evident in some other vertebrates, whose bones are separated for long periods of time.
The sternal angle is a useful landmark during physical examinations because this is where the second rib attaches. The lower line is thin and expresses the xiphoid interaction.
Xiphoid process
The pointed xiphoid process can be found at the sternum’s inferior end. Inappropriately performed chest compressions during cardiopulmonary revival can cause the xiphoid cycle to snap off, driving it into the liver which can cause a lethal drain.
A thin layer of compact bone covers the sternum, which is made up of highly vascular tissue and is thickest in the manubrium, which is located between the articular facets of the clavicles. The pericardium is connected to the posterior xiphoid process by the inferior sternopericardial ligament.
Joints
The ligaments of the main five ribs get together with the sternum at the sternocostal joints. The clavicles articulate with the right and left notches, respectively. It is simple to locate the costal cartilage of the second rib because it articulates with the sternum at the sternal angle.
One of the intercostal nerves innervates the transverse thoracic muscle, which is superiorly attached to the lower sternum’s posterior surface. It works to depress the ribs through its inferior attachment, which is the internal surface of costal cartilages two through six.
Functions of Sternum
One of the huge elements of the sternum is to safeguard the lungs, veins, and heart from any sort of injury, and it’s one of the longest and biggest level bones present in our body. The sternum is responsible for the following two major body functions:
- Support: Providing support for our chest and upper abdomen is one of the sternum’s most important functions. It provides support to the rib cage, collarbone of your body, and many other parts of your skeleton system.
- Protection: The sternum is in the middle of your chest, and many organs like the heart, lungs, and blood vessels are close by. consequently, it shields them from all forms of harm.
Development
Two cartilaginous bars, one on the left and one on the right associate with the rib ligament on each side to shape the sternum. The cartilaginous sternum, which is ossified from six centers, is formed when these two bars fuse along the middle to form the sternum. one for the manubrium, four for the body, and one for the xiphoid cycle.
The solidification places show up in the spans between the articular melancholy for the coastal ligaments, in the accompanying request: during the sixth month of fetal life, in the manubrium and first body part; during the seventh month of fetal life, in the second and third body parts; during the first year of life, in its fourth piece; between the fifth and eighth years of the xiphoid process.
The segments’ upper parts are where the centers begin, and they gradually descend. These may also occasionally include the appearance of two small episternal centers, one on each side of the jugular notch; They probably come from Monotremata and lizards’ episternal bones.
There are times when multiple centers, varying in number and position, form some of the segments. As a result, there may be two, three, or even six centers in the first piece.
At the point when two are available, they are for the most part arranged one over the other, the upper being the bigger; Rarely more than one is present in the second piece; The irregular union of the third, fourth, and fifth pieces often results in the rare occurrence of the sternal foramen or the vertical fissure that occasionally intersects this portion of the bone and is referred to as the “fissure sterni” malformation; The manner in which the cartilaginous sternum is formed further explains these conditions.
A fissure may divide the upper end of the sternum, which occurs less frequently still. By the time you’re 25 years old, all of your body’s centers have joined together. This process begins around puberty and progresses from the bottom up.
Before the age of thirty, the xiphoid process may join the body, but this happens more frequently after forty; On the other hand, in old age, it may not always be together. The manubrium may occasionally be joined to the body by bone in advanced life. At the point when this happens, nonetheless, the hard tissue is for the most part just shallow, the focal piece of the interceding ligament remaining unossified.
The body of the sternum is divided into four, not three, parts called sternebrae in infancy. sternebra).
Embryology
The sternum develops independently from a pair of sternal bands known as “sternal bars,” which are concentrations of mesenchymal cells on either side of the midline, during the sixth developmental week of fetal life. These two sternal bands both emerge from the parietal layer of the lateral plate mesoderm by the tenth week of intrauterine life. They then migrate and fuse in a craniocaudal direction to form the sternal plate, transforming into pre-cartilaginous structures.
In the seventh seven-day stretch of intrauterine life, the mesenchyme consolidates bringing about the development of the essential cartilaginous model of the three sternal portions (manubrium sterni, the body of the sternum, and the xiphoid cycle). Six sternebrae, or horizontal divisions, make up the cartilaginous sternal model. The manubrium sterni and the xiphoid process are ultimately represented by the superior-most sternebra and the inferior-most sternebra, respectively. The four sternebrae that are situated in between are what represent the body of the sternum.
Blood Supply and Lymphatics
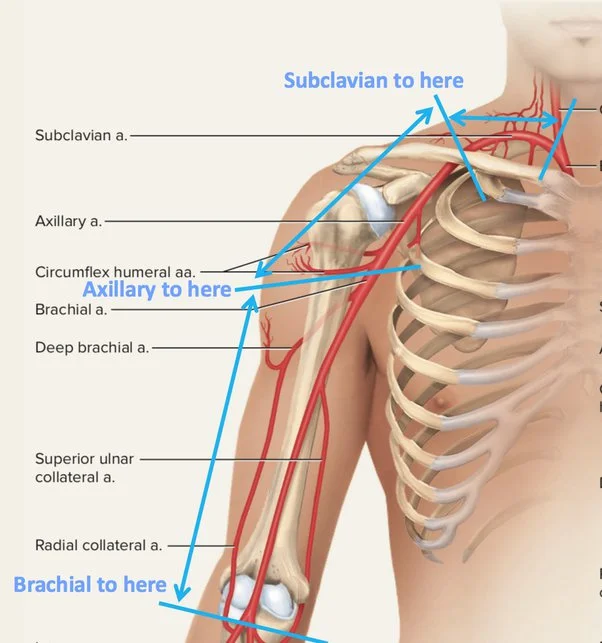
The medial horizontal branches of the right and left internal thoracic arteries, which either originate directly from the first part of the subclavian arteries bilaterally or occasionally from a common trunk, provide the majority of the sternum’s blood supply. The sternal, anterior intercostal, perforating, and non-collateral branches are produced by the internal thoracic artery. The intercostal spaces are primarily home to the sternal branches of the internal thoracic arteries, which are the primary branches that supply the sternum. The sternal blood supply appears to be enhanced by perforating branches in addition to sternal branches.
After sternotomy procedures, the sternum’s blood supply plays a significant role in healing. Understanding the sternum’s blood supply is also important because sternal infections are common after the internal thoracic artery is harvested for coronary artery bypass grafting.
For venous waste, the inside thoracic veins channel into the brachiocephalic vein on each side.
Muscles of Sternum
There are a few muscles (muscles of the neck, muscles of the chest, muscles of the foremost stomach wall) connected to the sternum. The manubrium sterni is where the sternocleidomastoid, sternohyoid, and sternothyroid all attach. The body of the sternum and the xiphoid process is joined by the transverse thoracic muscle. Another significant muscle attached to the sternum’s body is the Pectoralis major. The diaphragm, the most important muscle for breathing, and the abdominal muscles, including the transversus abdominis, rectus abdominis, and external oblique muscles, are able to attach to the xiphoid process.
Physiologic Variants of Sternum Bone
When compared to males, females typically have a sternum that is shorter and thinner.
Anatomic Variations
The sternum can be found in many different forms. Varieties are most normal in the distal-most district of the sternum. The bifid xiphoid is one of the most common variations of the sternum.
Additionally, there are anatomical variations of the sternal angle. For instance, the sternal angle can be misplaced, resulting in an incorrect counting of the ribs during the physical examination of the chest as well as errors in procedure during nerve blocks and needle thoracotomies. In addition, sternal angle misalignment can make blunt chest trauma more likely to result in sternal fracture. Here and there an extra sternal symphysis “point” can exist, which on imaging studies can copy a sternal crack, horrendous gap, or osteolytic sore.
One more inherent deformity of the front chest wall is the sternal split, which results from the disappointment of the midline combination of the sternum. The sternal cleft can be completely or partially separated depending on the degree of separation. The heart and major vessels are left unprotected and exposed by the sternal cleft. Another reason why a narrow sternal cleft is of clinical significance is that it can be mistaken for a sternal fracture.
A sternal foramen that is circular in shape may result from an incomplete fusion of the cartilaginous sternal model. During thorax imaging studies, this anomaly should not be mistaken for one. The sternum’s anatomical variations should be well-understood by radiologists and surgeons. Besides, the absence of consciousness of the sternal foramen is a subject of worry for the criminological pathologist or anthropologist during the measurable assessment of the skeletal remaining parts.
Clinical importance
Sternotomy/cardiothoracic surgery
To gain access to the thoracic organs during open cardiothoracic surgery, the sternum must be divided and splayed open. Open abdominal aortic aneurysm repair and coronary artery surgery both benefit from this approach. Sternotomy, on the other hand, is becoming less and less common as radiologically guided, minimally invasive procedures like EVAR (endovascular aneurysm repair) have emerged. The patient experiences less morbidity and has a shorter recovery time thanks to the more recent methods.
Sternoclavicular joint dislocation
This is an unprecedented crack, and because of its area in the extraordinary vessels, is possibly quickly hazardous. Side effects will incorporate irritation around the area, and assuming the extraordinary vessels are compromised, abrupt demise.
Sternal fracture
A motor vehicle accident or high-impact direct trauma from another cause is the most common cause of this rare fracture. The most frequently injured part of the bone is the manubrium. The ribs frequently fracture as well due to their close proximity and direct connection. Compromise of vital organs is possible.
Bone marrow biopsy
Because there is limited access to the iliac crest, bone marrow biopsy is performed at the sternum in obese or overweight patients.
Pectus excavatum
Pectus excavatum, otherwise called channel chest, is a condition wherein the sternum and prevalent ribs develop strangely, bringing about an indented chest appearance. Ehler’s Danlos syndrome and Marfan syndrome, both of which involve a defect in collagen, are potential causes.
Pectus carinatum
Pectus excavatum is the opposite, and it occurs when the sternum and ribs grow abnormally, causing them to protrude outward. This condition also occurs in a number of syndromes, including Down’s syndrome, Marfan syndrome, and osteogenesis imperfect. The chest has the shape of a bird.
Broken Xiphoid Process
During CPR, when it is at risk of being broken, the xiphoid process presents a safety risk due to the stark differences in size and strength between it and the rest of the sternum.
The person performing CPR is probably unaware that a fracture has occurred while they are saving a life. Continued CPR after a broken xiphoid process can cause this sharp part of the sternum to penetrate one of the underlying organs, resulting in a damaged heart, spleen, liver, or diaphragm.
FAQs
Together with your ribs, the sternum safeguards the torso organs like your heart, lungs, and blood vessels in your chest. Support. Your sternum likewise gives an association that highlights different pieces of your skeletal framework, including your collarbone and a large portion of your ribs.
The pectoralis major and sternocleidomastoid sternal fibers are attached to the anterior surface.. The posterior surface gives attachment to sternohyoid and sternothyroid muscles.
Infection, inflammation, injury, or the sternum’s own cartilage breaking down can all cause pain in this area. Pain in this area can also be caused by issues with nearby organs like the heart, lungs, and esophagus. This incorporates respiratory failure, pleurisy (a lung irritation), and indigestion.
The costochondral joint is comprised of the ligament that associates your ribs to your breastbone (sternum). The pain of costochondritis is sharp or aching. The aggravation can begin out of nowhere or grow gradually and spread across your chest.
Hormones like adrenaline and cortisol, for example, can be produced in response to stress. This can make it hard to inhale and raise your pulse and circulatory strain. Additionally, your chest muscles may contract and your throat may constrict. Any of these can burden the chest.
Most of the time, a broken sternum will heal on its own. The pain may not go away for three months or more. You have been thoroughly examined by the doctor, but problems can arise later. Get medical attention as soon as you notice any issues or new symptoms.

3 Comments